Background: Wernicke's encephalopathy is a metabolic disorder caused by thiamine deficiency, and is characterized by acute mental confusion, ophthalmoplegia and ataxia. Its due to nutritional deficiency arising from prolonged illness affecting nutrition of the patient or requiring parenteral nutrition for prolonged duration, debilitating chronic illnesses like solid organ and lymphoid malignancies. It has been commonly seen chronic alcoholics who have poor oral intake. It is a rare neurologic complication in the setting of hematopoietic stem cell transplantation (HSCT). So, a high index of suspicion should be kept in HSCT patients as delay in early identification may lead to permanent neurologic disability or even mortality.
Material and methods: We report a case of wernickes encephalopathy in post-transplant patient who had poor oral intake and prolonged hospitalization for different complications post-transplant. Based on the review of literature and our experience, it's prudent to have an early radiologic investigation done in suspected patients as clinical features along with typical MRI (magnetic resonance imaging) findings of brain are highly suggestive of Wernicke's encephalopathy following HSCT.
Results: A 55-year-old hypertensive, obese, non-diabetic female, case of relapse acute myeloid leukemia underwent allogeneic stem cell transplant from a matched unrelated donor [MUD], since she had no human leucocyte antigen (HLA) matched siblings. Post-transplant, on day +66 she was evaluated for complaints of severe loss of appetite and vomiting and was suspected to have acute GVHD. She was admitted and immediately started on parenteral methylprednisolone at 1 mg/kg. On day +75 post-transplants, the patient complained of extreme fatigue, dizziness, gait disturbance, and restlessness and soon became bedbound. Neurological examination revealed mild confusion, bilateral horizontal gaze nystagmus, bilateral lower limb ataxia, and truncal ataxia and tremors. Power on examination was 5/5 in all limbs. Based on neurological signs and MRI imaging features, she was diagnosed as Wernicke's encephalopathy secondary to malnutrition. The patient was given a high dosage of intravenous thiamine, 500 mg three times a day, as well as a steadily rising high-calorie and protein meal through a ryles tube feeding. After three days, the patient responded to the treatment with a noticeably improved gait, consciousness, and the absence of tremors and nystagmus. By day 10 of thiamine therapy, ryles tube was removed and patient began active oral feeding. She was able to do activities of self-care.
Conclusion: We report a post HSCT patient with Wernicke's encephalopathy who had poor oral intake and prolonged hospitalization for several post-transplant complications. Poor oral nutrition or prolonged TPN without the addition of thiamine post HSCT might undoubtedly result in WE even though it is an unusual complication of HSCT, therefore, addition of IV thiamine is essential for the patients.
Wernicke's encephalopathy, Thiamine deficiency, Stem cell transplant, AML
Dr. Carl Wernicke, a Polish neurologist who first described Wernicke's encephalopathy in 1881, is honoured by the disease's name. Acute mental confusion, ataxia, and ophthalmoplegia were initially thought to be the classic triad that best described the syndrome, but it was later discovered that only one-third of patients actually experienced this triad [1]. Clinical diagnosis of Wernicke's encephalopathy is possible when a patient exhibits central nervous system (CNS) symptoms that are consistent with radiologic evidence, particularly on brain magnetic resonance imaging [2].
Wernicke's encephalopathy (WE), which is caused by thiamine deficiency, is a fatal neurological condition with an abrupt onset. Some of the causes include alcohol abuse, malnutrition, gastric bypass surgery, HIV infection, total parenteral nutrition (TPN), chronic dialysis, and cancer [3]. Its due to nutritional deficiency arising from prolonged illness affecting nutrition of the patient or requiring parenteral nutrition for prolonged duration, debilitating chronic illnesses like solid organ and lymphoid malignancies. It has been commonly seen in chronic alcoholics who have poor oral intake.
HSCT is frequently associated with anorexia, varying degrees of stomatitis, graft-versus-host disease (GVHD), and infections of the gastrointestinal system, which impair oral intake and sometimes require complete parenteral nutrition for an extended period of time. HSCT patients are thus at risk of developing thiamine deficit since marketed TPN frequently lacks thiamine. Only a few Wernicke's encephalopathy instances associated with HSCT have been recorded globally [4].
We report a post HSCT patient with Wernicke’s encephalopathy who had poor oral intake and prolonged hospitalization for several post-transplant complications. She was diagnosed in time and managed with parenteral thiamine supplementation leading to complete reversal of neurological symptoms. It is wise to perform an early radiologic evaluation in suspected individuals since clinical signs and typical brain MRI (magnetic resonance imaging) findings are strongly suggestive of Wernicke's encephalopathy.
A 55-year-old hypertensive, obese, non-diabetic female, case of relapse acute myeloid leukemia underwent allogeneic stem cell transplant from a matched unrelated donor [MUD], since she had no human leucocyte antigen (HLA) matched siblings. She received a conditioning regimen consisting of intravenous (IV) busulfan and cyclophosphamide. Graft versus host disease (GVHD) prophylaxis consisted of cyclosporin A and a short course of methotrexate. The transplanted cell dose was 7.12 × 10 6 CD34 cells/kg. She was discharged after engraftment of neutrophils and platelet.
Post discharge patient had only mild improvement in appetite and her diet predominantly consisted of beverages, fruits and biscuits. Post-transplant, on day +66 she was evaluated for complaints of severe loss of appetite and vomiting and was suspected to have acute GVHD. She was admitted and immediately started on parenteral methylprednisolone at 1 mg/kg. Upper gastrointestinal tract endoscopy and Biopsy showed mild duodenitis without any evidence of GVHD. The Duodenal biopsy was also stained for giardia lamblia which was negative. Giardiasis was ruled out as its one of the important causes for poor oral intake, vomiting, weight loss in post-transplant patients in tropical countries and thus it could mimic GVHD [2]. As a result, steroids were tapered quickly and stopped after 5 days. She continued to eat poorly and experienced diminished appetite. She became distant, quiet, infrequently initiated conversations on her own and apathetic. On day +75 post-transplants, the patient complained of extreme fatigue, dizziness, gait disturbance, and restlessness and soon became bedbound. Neurological examination revealed mild confusion, bilateral horizontal gaze nystagmus, bilateral lower limb ataxia, and truncal ataxia and tremors. Power on examination was 5/5 in all limbs. On day +78 Patient developed fever and altered sensorium, with CBC showing hemoglobin 7 g/dl, total leucocyte counts 680/cumm, platelet count 16000/cumm. Peripheral smear suggestive of microangiopathic hemolytic anemia (MAHA) with > 1% schistocytes. Serum creatinine was 0.6 mg/dl. Plasma Cyclosporine levels were tested and they were withing normal range on multiple occasions, so calcineurin inhibitor (CNI)-induced neurotoxicity was ruled out. Another differential was transplant associated thrombotic microangiopathic anemia (TA-TMA) and the neurological worsening to be part of the process. Fundus examination of the eye was also done and showed absence of roths spots, retinal hemorrhages or papilloedema.
Cerebrospinal fluid (CSF) analysis was done to rule out meningitis and it tested negative for tuberculosis, cryptococci and fungi. PCR based meningoencephalitis panel in CSF was also negative for causative bacteria and viruses like enterovirus, CMV, Herpes simplex virus 1 (HSV-1), HSV-2, HHV-6, human parechovirus and varicella zoster virus. MRI brain on T2 FLAIR sequence showed characteristic hyperintense foci in medial thalamus and mamillary bodies (Figure 1). So based on neurological signs and MRI imaging features, she was diagnosed as Wernicke’s encephalopathy secondary to malnutrition. The patient was given a high dosage of intravenous thiamine, 500 mg three times a day, as well as a steadily rising high-calorie and protein meal through a ryles tube feeding. After three days, the patient responded to the treatment with a noticeably improved gait, consciousness, and the absence of tremors and nystagmus. By day 10 of thiamine therapy, ryles tube was removed and patient began active oral feeding. She was able to do activities of self-care.
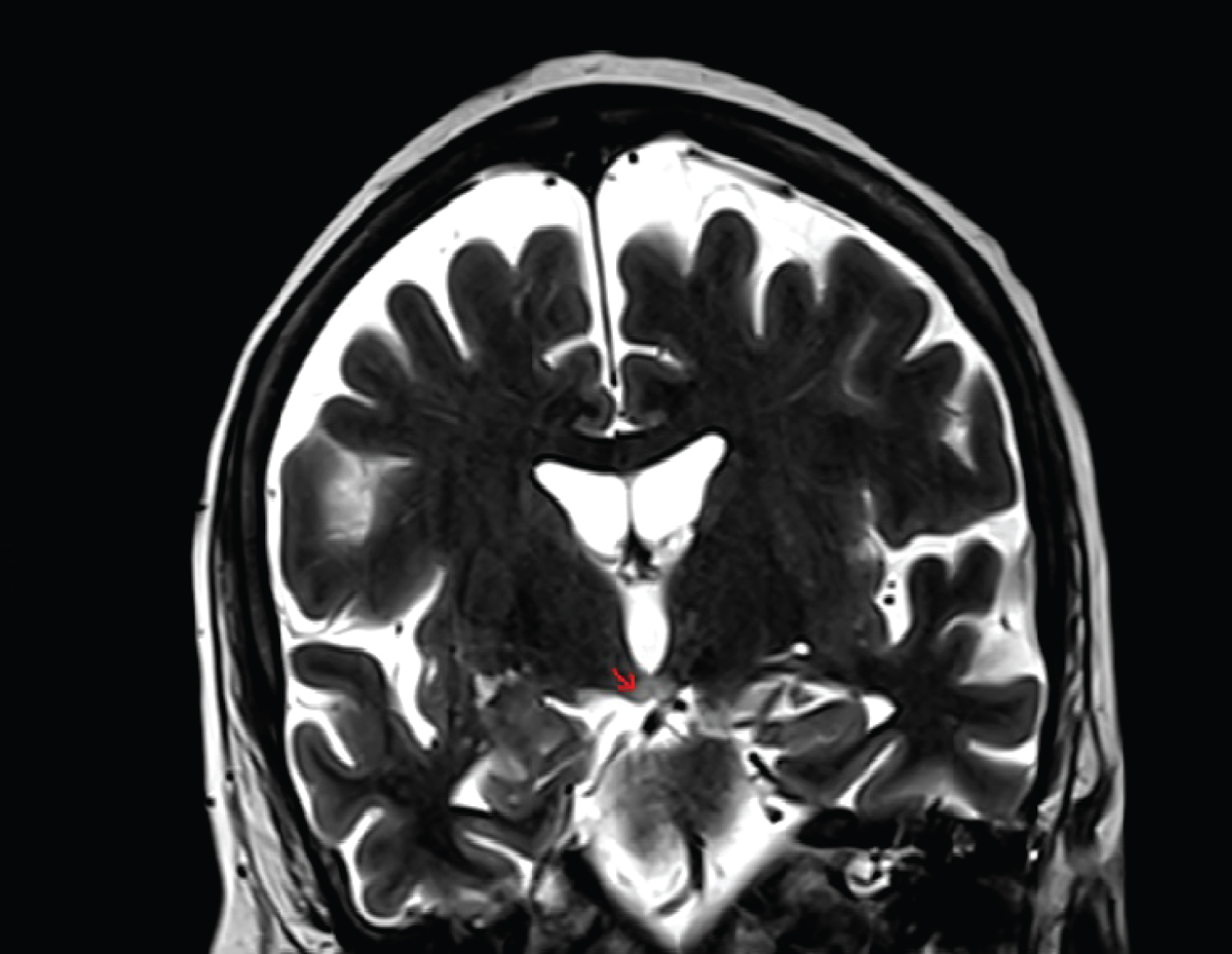 Figure 1: MRI brain on T2 FLAIR sequence showed characteristic hyperintense foci in medial thalamus and mamillary bodies.
View Figure 1
Figure 1: MRI brain on T2 FLAIR sequence showed characteristic hyperintense foci in medial thalamus and mamillary bodies.
View Figure 1
Wernickes encephalopathy is characterized by triad of altered mental status, ataxia and ophthalmoplegia. Thiamine (vitamin B1) insufficiency is a prevalent cause of Wernicke's encephalopathy, which frequently occurs in alcoholics. Thiamine is essential vitamin for producing the energy required for cerebral activities. It contributes as a cofactor for enzymes necessary for the Krebs cycle, such as pyruvate dehydrogenase and alpha-ketoglutarate. Thus, thiamine deficiency causes thiamine-dependent enzymes to function less efficiently, which in turn causes impaired cerebral energy utilization and neuronal damage [5].
There are very few cases of WE in AML reported in the literature. Altered sensorium, tremors and gait imbalances in cancer patients can have a multitude of causes, including hypoxia, infections, electrolyte imbalances, opioid medications, chemotherapy, brain and meningeal metastases, making a diagnosis of WE difficult [6]. It is essential to have suspicion of WE due to the potential for overlapping clinical symptoms between several disorders that can present after a transplant, which can result in diagnostic confusion and a delay in diagnosis. So, the common clinical conditions are- viral encephalitis like HHV6 or HSV, fungal meningoencephalitis, TA-TMA, TTP due to calcineurin inhibitors.
Thiamine levels in blood or erythrocyte transketolase activity can be measured to confirm WE, although these assays are not commonly available [7]. 500 mg of thiamine should be administered three times daily for 2-3 days as an empirical treatment for WE. After 2-3 days, supplements may be stopped if there is no improvement. If an effective response is shown, thiamine 250 mg daily should be maintained until clinical improvement [8].
In study by Taggart, et al., it was shown that, after implementation of ‘vitamin Thursday’ whereby they administered routine thiamine supplement to all the patients undergoing HSCT, no patients have developed WE [9]. There are few isolated case reports of WE in transplant setting which have shown dismal outcome if there is delay in diagnosis [4,10].
Patients with hematologic malignancies who have inadequate oral nutrition should unquestionably add thiamine supplements to their meals or TPN. Brain MRI should be done as soon as symptoms like ataxia, disorientation, or ocular abnormalities appear in these patients, and thiamine infusion should start right away if there is a high suspicion.
Poor oral nutrition or prolonged TPN without the addition of thiamine post HSCT might undoubtedly result in WE even though it is an unusual complication of HSCT, therefore, addition of IV thiamine is essential for the patients.
Wernicke's encephalopathy (WE), which is caused by thiamine deficiency, is a fatal neurological condition with an abrupt onset.
We report a post HSCT patient with Wernicke’s encephalopathy who had poor oral intake and prolonged hospitalization for several post-transplant complications.
Poor oral nutrition or prolonged TPN without the addition of thiamine post HSCT might undoubtedly result in WE even though it is an unusual complication of HSCT, therefore, addition of IV thiamine is essential for the patients.
All authors have no conflict of interest.
No financial support was taken.
Patient Permission to publish the data has been taken from the patient.
The study has been approved by the Institutional Review Board of our Centre.