We present the case of a half-blood Mexican male, 48-years-old, with a family and medical history of multiple thromboembolic events that are directly associated with the diagnosis of sticky platelet syndrome. This condition has presented diverse complications of procoagulant activity due to insufficient management therapy. Sticky platelet syndrome is an autosomal disorder that is associated with thromboembolisms. It distinguishes itself from others due to its hyperaggregability at lower doses of anti-aggregation platelet agents. Its exact epidemiology remains unknown, and it is treated with aspirin at a lower dose or clopidogrel in cases of resistance. The lack of significant studies adds a halo of mystery to this pathology and encourages further investigation.
Sticky platelet syndrome, Thrombophilia, Platelet disorders, Platelet hyperaggregability, Acetylsalicylic acid, Clopidrogel, Thromboembolism
Sticky platelet syndrome is probably an autosomal dominant disorder [1] associated with venous and arterial thromboembolic events [2]. Platelets stick together too much in response to low doses of agents that stop platelets from sticking together, such as adenosine diphosphate (ADP), epinephrine, or both [3]. Clinically, it manifests as episodes of arterial or venous occlusion, including acute myocardial infarction, angina pectoris without coronary disease, brain stroke, transient ischemic attack in young patients, and ischemic optic neuropathy [1-5]. It can also cause thrombosis in atypical sites [3] and is frequently associated with psychogenic stress disorders [6]. This hereditary thrombophilia is considered the second-most common cause in individuals of Mexican descent [7].
Current research suggests that polymorphic genes, such as GAS6, PEAR1, and GP6, play a principal etiopathogenic role [8]. These genes make platelet surface receptors called membrane glycoproteins, which may make a person more likely to have a prothrombotic state in which platelets stick together too much when ADP or epinephrine is present [3,8]. However, although cases with familial recurrence exist, there is not enough research to determine if the syndrome follows an autosomal dominant or recessive inheritance pattern [9].
Due to the lack of studies on this syndrome, its exact prevalence worldwide remains unknown. In Mexico, several studies have reported certain numbers; however, their credibility is low due to self-citation practices. Nevertheless, a constant finding in epidemiological studies is that the syndrome rarely is diagnosed without hematological abnormalities. Sticky platelets are often caused by resistance to activated protein C, the factor V Leiden mutation, the HR2 haplotype, the Hong Kong mutation, protein C deficiency, antithrombin 3 deficiency, protein S deficiency, the factor 2 G20210A mutation, high levels of coagulation factor VIII, or lupus anticoagulant or antiphospholipid syndrome [10,11].
The diagnosis of sticky platelet syndrome is complex due to a lack of knowledge about the pathology and the absence of a globally accepted consensus [12]. A complete screening is usually performed to detect prothrombotic states and induce platelet aggregation using epinephrine or adenosine diphosphate [3]. The diagnosis is made by seeing increased platelet aggregation in platelet-rich plasma samples when lower doses of inducers (EPI and ADP) are used [13].
Platelet agglutination can lead to the temporary or permanent occlusion of blood vessels [14]. Sticky platelet syndrome is therefore considered a risk factor for vascular events [15]. However, not all patients with SPS are symptomatic or experience thrombotic complications. The clinical manifestations vary depending on the individual and their particular complications.
The most common complications in these patients are arterial thromboembolism (ischemic stroke, ischemic heart disease, ischemic peripheral arterial disease), venous thromboembolism (deep venous thrombosis, pulmonary embolism), and thromboembolic events in classic locations (such as deep venous thrombosis of the lower extremity, pulmonary embolism) or atypical locations (such as embolisms in dural venous sinuses, central veins, and optic veins). Additionally, pregnant individuals may experience recurrent miscarriage and fetal growth restriction, while transplant recipients may have microvascular free flap failures [3,4,8,9,12,14].
Aspirin treatment at a lower dose has been accepted as a therapeutic option for this syndrome. In cases where hyperaggregability persists despite aspirin treatment, clopidogrel can be added [16]. This is because aspirin decreases the conversion of arachidonic acid to prostaglandin G2, prostaglandin H2, and thromboxane A2. Clopidogrel inhibits platelet aggregation by inhibiting the union of ADP with the platelet receptor and the subsequent activation of the GPIIb-IIIa complex mediated by ADP [17].
The patient is a 48-year-old Mexican male with a family medical history that includes a relative from Spain, while the rest of the family members are Mexicans. In his family history, his father passed away at the age of 78 due to a stroke, and his mother, who is currently 88-years-old, has deep venous thrombosis.
In October 2021, he received the second dose of the AstraZeneca vaccine against SARS-CoV-2.
The patient reported experiencing high psychogenic stress days before his hospitalization.
The patient arrived at the emergency department on September 9 th , 2021, reporting sudden pelvic pain the day before with a visual analog scale (VAS) pain score of 10/10, which radiated to the sacrum. While standing, a postural change caused the pain, which subsided when the person lied on their upper back. It limited his ability to walk. During the physical examination, there was pain upon touching the sacrum and bilateral femoral zones. The testicles appeared normal upon visual inspection, with minimal pain upon touch. There was no edema in the extremities, and femoral, popliteal, dorsalis pedis, and posterior tibial pulses were present with immediate capillary refill.
During the medical interview, the patient mentioned a stroke event in 2012 as part of his medical history. Upon evaluation, a patent foramen ovale was detected and treated in the same year. Additionally, the patient developed deep venous thrombosis and was diagnosed with pulmonary thrombosis the following month, which was treated with the placement of a venous cava filter.
Due to the recurrence of thrombotic events, the patient underwent a "hematological profile," which resulted in the diagnosis of type 2 sticky platelet syndrome in 2012 and aggregometry confirmation (Figure 1). He was prescribed rivaroxaban for 3 years, which was discontinued in 2015 until his hospitalization date. The patient reported not taking aspirin (Table 1).
Table 1: Research of sticky platelets. View Table 1
During his hospitalization, a contrast abdomen tomography was taken (13/11/21) (Figure 1, Figure 2 and Figure 3).
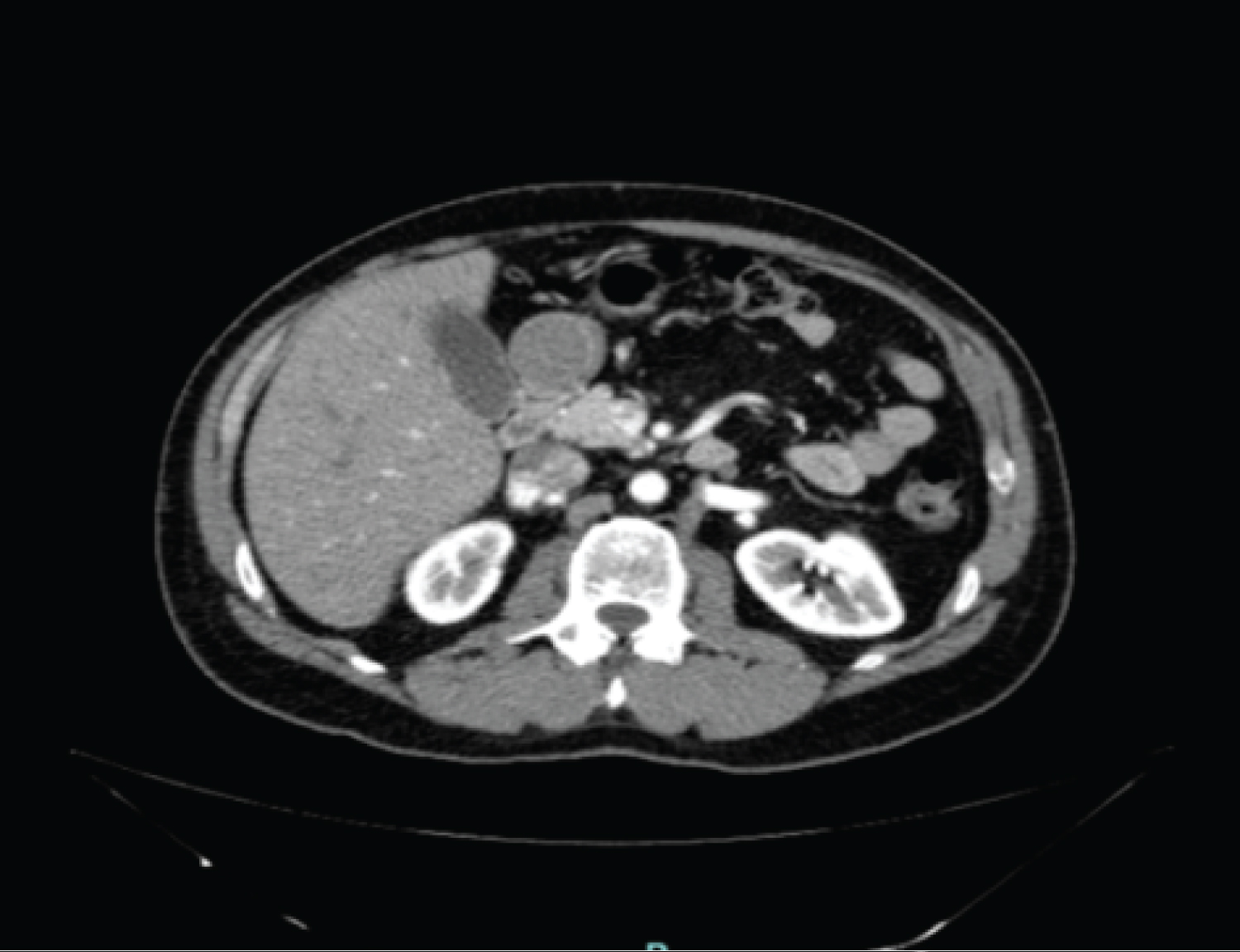 Figure 1: A thrombus that extends from the lower vena cava shows a vena cava filter.
View Figure 1
Figure 1: A thrombus that extends from the lower vena cava shows a vena cava filter.
View Figure 1
 Figure 2: It shows the vena cava filter and thrombus that extend by.
View Figure 2
Figure 2: It shows the vena cava filter and thrombus that extend by.
View Figure 2
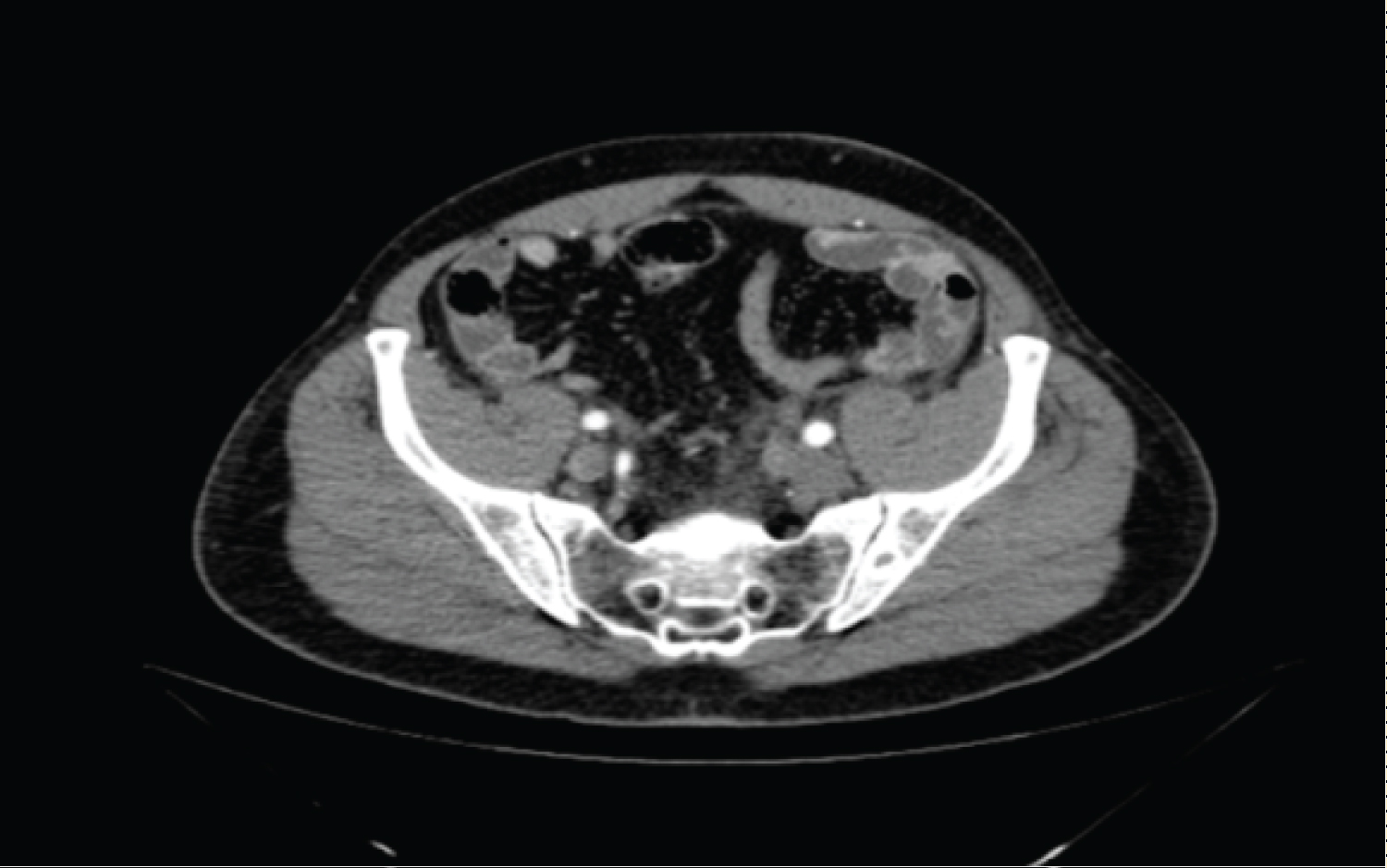 Figure 3: Involvement of both iliac and femoral veins.
View Figure 3
Figure 3: Involvement of both iliac and femoral veins.
View Figure 3
Report of bilateral ascendent phlebography, venous thrombectomy of iliac veins and lower vena cava and intravascular ultrasound (IVUS) of iliac veins and lower vena cava (15/11/21) (Figure 4a and Figure 4b).
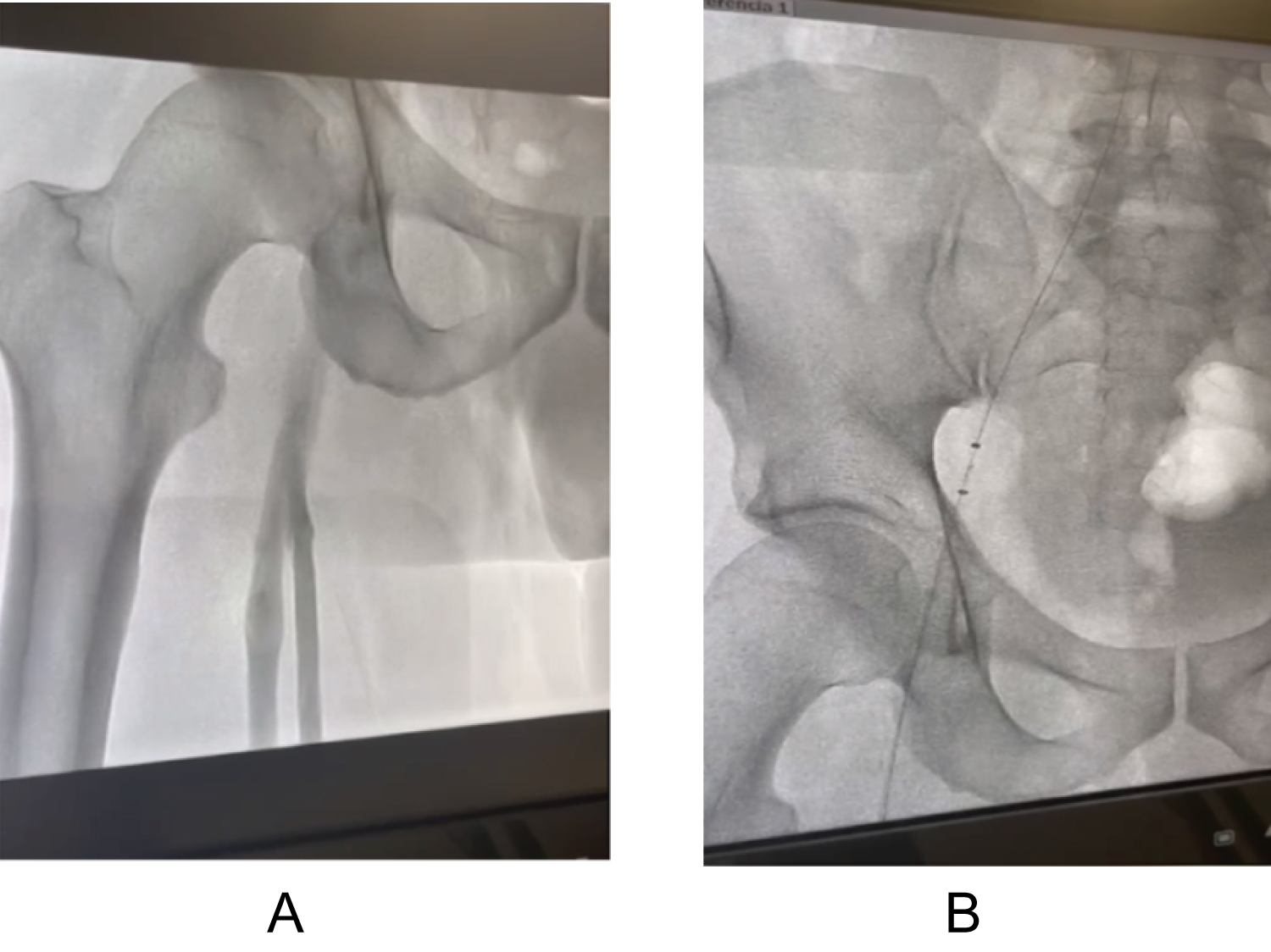 Figure 4: (a and b) Image A shows an X-ray preview at the start of the therapeutic catheterization, while image B is about an X-ray after the intervention.
View Figure 4
Figure 4: (a and b) Image A shows an X-ray preview at the start of the therapeutic catheterization, while image B is about an X-ray after the intervention.
View Figure 4
During hospitalization, an echocardiogram is done, which reports a well-closed foramen ovale without data of pulmonar hypertension; the rest are normal.
After a good rest and hospital vigilance, the patient gets out in a few days, with medical treatment based on aspirin 100 mg every 24 hours and an appointment every 6 months.
This case report provides results that can be explained due to a consistent clinical history of pathological stroke events, deep venous thrombosis, pulmonary thromboembolism, and filter thrombosis of the vena cava. Furthermore, the patient has a family medical history of thrombotic complications that haven't necessarily been attributed to sticky platelet syndrome. These complications could be associated with other types of thrombotic syndromes. However, it is still an important point to consider, as the majority of people with this syndrome often have other concurrent coagulation disorders or abnormalities. The patient's medical records contain detailed documentation regarding the diagnosis procedures, which is beneficial for analysis and understanding of this disease.
On the unfortunate side for the patient, but fortunate for educational purposes, the lack of adequate anticoagulant treatment has contributed to the persistence of complications. This serves to illustrate the pathophysiological aspects of this disease.
Another important aspect of this case is that both of the patient's parents have experienced other types of thromboembolic complications. Although this does not directly explain their thromboembolic issues or rule out other autonomous diseases, it does raise awareness of potential genetic predispositions.
Regarding the diagnostic method used for this patient in 2012, aggregometry was employed based on Mammen's prospective criteria. This confirmed the diagnosis by demonstrating hyperaggregability to two reactive concentrations of epinephrine (EPI) throughout the patient's medical history of thromboembolism. The patient was classified as type II based on these criteria (Table 2).
Table 2: View Table 2
Since the beginning of his diagnosis, the patient has mentioned being treated with rivaroxaban, a therapy that has not been proven yet. However, aspirin treatment at a lower dosage has also not shown superiority compared to other drugs. Due to the lack of data on pharmacological treatments, it is impossible to determine if there is a better option than aspirin at a lower dosage.
It is possible that being treated with rivaroxaban predisposed him to recurrent thrombotic complications, leading to the consideration of treating him with 100 milligrams of aspirin every 24 hours.
Another important point could have been to identify hematological abnormalities in his ancestors through laboratory data. This could have helped determine which individuals had sticky platelet syndrome or other comorbidities that contribute to this platelet disorder. It is worth noting that the patient has Spanish heritage, which many researchers have identified as a risk factor.
A significant lack of research exists, leaving several unresolved aspects. Firstly, lab tests are not standardized, leading to internal laboratory variability. Additionally, patient-specific factors like race, comorbidity, diet, and medication use (such as ASA, NSAIDs, and ADP receptor antagonists), as well as external factors like stressful situations, recent thromboembolism, and pregnancy, can affect cutoff points. Secondly, well-defined criteria for patient selection in platelet tests are lacking. Thirdly, there are several therapeutic points without a solution. Most of the available data is related to acetylsalicylic acid, and there is insufficient research on concurrent treatment for other thrombotic diseases. Furthermore, none of the studies have focused on the safety and efficacy of combined therapy. Lastly, there may be heterogeneity within the syndrome. While autonomic aspects have been discussed, there are differing opinions regarding published data, and not all studies include a detailed medical family history.
The relevance of this case report lies in the fact that the patient, due to therapeutic insufficiency, experiences the majority of the most common complications of this pathology, which also contributes to increased morbidity and mortality. Although there have been updates in the research on this syndrome, discrepancies still exist and there is a lack of evidence. It will be clarified through systematic reviews, meta-analyses, or randomized clinical trials what is relevant in terms of treatment. This highlights that there is still a long way to go before achieving a globally accepted consensus.
Personal information and the anonymity of the patient were preserved by removing all aspects of the manuscript related to the patient's identity. As authors of this case report, our team declares that we have no conflicts of interest. The Hospital San Javier ethics committee has approved the study.