Background: Diabetic retinopathy is a complication of type 2 diabetes resulting from long-term accumulated damage to retinal blood vessels and one of the life-threatening complications and is the most common cause of acquired blindness in adults and it affects 93 million people worldwide. DR is the principal cause of blindness in adults of working age and responsible for a worsening in quality of life despite preventable and treatable causes. To date, most of the epidemiological research on DR in Ethiopia has been limited to prevalence estimates from cross-sectional studies. This study determined the incidence of retinopathy and its predictors among type 2 diabetic patients.
Methods: Hospital-based retrospective follow-up study was conducted among 420 adults with newly diagnosed type 2 diabetic patients from January 1, 2014, to December 31, 2019. Data were extracted from medical records and entered into Epi info version7.2.2.6and exported to Stata 14 for analysis. Bivariable and multivariable Cox proportional hazard model were used to identify predictors of diabetic retinopathy. In a multivariable analysis variable having a p-value < 0.05 in the Cox; PH model was considered as predictors of diabetic retinopathy.
Results: Overall, 19.5% (95% CI; 16.2-23.8) of the study population developed diabetic retinopathy, with a median survival time of 30.4 months. Congestive heart failure [AHR: 2.53 (95% CI; 1.49, 4.29)], chronic kidney disease [AHR: 5.02(95% CI; 2.73, 9.26)], hypertension [AHR: 2.07(95% CI; 1.17, 2.89)], and HBA1c [AHR: 10.5 (95% CI; 5.6, 19.6)] were found to be predictors of diabetic retinopathy.
Conclusion and recommendation: The incidence of diabetic retinopathy among type 2 diabetes patients was high in this study area. Especial emphasis should be given for patients with heart failure, chronic kidney disease, high baseline BP (> 140/90 mmHg) and high baseline HBA1c (≥ 7%).
Incidence, Diabetic retinopathy, Predictors, Type 2 DM, Gondar, Ethiopia
AHR: Adjusted Hazard Ratio; AOR: Adjusted Odds Ratio; ATR: Adjusted Time Ratio; CHF: Congestive Heart Failure; CHR: Crude Hazard Ratio; CKD: Chronic Kidney Disease; CI: Confidence Interval; Cr: Creatinine; DM: Diabetes Mellitus; DR: Diabetic Retinopathy; HTN: Hypertension; HBA1c: Hemoglobin BA1c; HDL: High Density Lipoprotein; LDL: Low Density lipoprotein; SRS: Simple Random Sampling; UOGCSH: University of Gondar Comprehensive Specialized Hospital; USA: United States of America
Diabetes mellitus (DM) is defined as metabolic disease presented with the chronic raising of blood glucose with the disorder of carbohydrate, fat, and protein metabolism due to problems in insulin production, insulin function, or both [1,2].
The overall worldwide magnitude of diabetes in 2019 was estimated to be 9.3% (463 million individuals), rising to 10.2% (578 million individuals) by 2030 and 10.9% (700 million) by 2045 in adults aged 20-79 years [3]. A systematic review done in 2018 showed that the magnitude of type 2 DM in Africa estimated to be 4.83% [4]. Studies conducted in Ethiopia showed that the magnitude of type 2 DM in Ethiopia was found to be 5.3% and complications associated with increasing type 2 DM burden are the major causes of morbidity and pre-mature mortality with the consequence of negative economic impact resulted in public health challenge [5-7].
Diabetic retinopathy (DR) is a complication of type 2 diabetes resulting from long-term accumulated damage to retinal blood vessels and one of the life-threatening complications and is the most common cause of blindness in adults [8,9]. DR is characterized by signs of retinal ischemia (retinal microvascular abnormalities, microaneurysms, hemorrhages, cotton wool spots, and neovascularization) and/or signs of increased retinal vascular permeability and It particularly affects patients with type 2 diabetes (T2DM) whose vision may be threatened by diabetic macular edema (DMO) [10]. The epidemic raised in diabetes poses significant public health and socioeconomic challenges through diabetic complications, of which diabetic retinopathy (DR) or damage to the small blood vessel of retina is the most common and feared diabetic complication that result in blindness [11].
There are 93 million people are living with DR globally [12]. Studies done across many countries indicated that the burden of DR was geographically heterogeneous, including in low and middle-income countries [13].
According to a systematic review, DR affects 30.2-31.6% of diabetes patients in Africa, Specifically; the incidence of DR is increasing rapidly in Sub-Saharan Africa countries imposing a huge economic burden on these countries [13-15].
Several studies in Ethiopia have shown that the presence and severity of complications related to DR are steadily increasing cause of premature death and disability [15,16]. In a retrospective follow up study conducted at Tikur Anbesa Hospital, Ethiopia, the incidence rate of diabetes retinopathy was 2.65 (95% CI 2.54, 4.05) per 1000 person-years observation [15].
Many studies suggested that the predictors of DR among type 2 DM patients are old age, male sex, high body mass index (BMI), hypertension, poor glycemic control, type 2 diabetes mellitus (T2DM), blood pressure (BP), elevated cholesterol level and long duration of diabetes since diagnosis [17,18].
In developed countries DR is the principal cause of blindness in adults of working age and is responsible for a worsening in quality of life and it is one of the leading causes of blindness in the working age population with devastating consequences, despite being possibly preventable and treatable causes [18-20]. Some articles in Ethiopia indicated that the Incidence of DR among type 2 diabetic patients is increasing and the causes of DR are different in different settings. Despite its burden and variability of causes across studies, there is limited data related to the proposed study in the study area that explore potential risk factors of DR to apply evidence-based interventions for type 2 DM patients.
To date, most of the epidemiological research on DR in eastern Africa including Ethiopia has been limited to prevalence estimates from cross-sectional studies. This study determined the incidence of retinopathy and its predictors among type 2 diabetic patients at chronic follow-up clinic of University of Gondar Comprehensive Specialized Hospital.
In Ethiopia, individuals having type 2 DM and its long-term impact specially DR is the major causes of morbidity besides to its economic crisis and social stigma. Quantifying the burden of the disease and early detection of the risk factors is paramount in the prevention of DR results reduction dependency and social stigma. Literature sources that showed factors exacerbating DR were too limited. Therefore, exploring other potential risk factors and prevention of DR would be imperative.
In Ethiopia, evidences on incidence and causes of DR are lacking. This effort tried to estimate the incidence and causes of DR among diabetics at University of Gondar Comprehensive Specialized Hospital.
Also, the results of this study provide information for health care providers, health institutions, health administrative offices, and policymakers to maximize efforts on the prevention and risk minimization of DR in type 2 DM patients and death due to complications through strict follow-up and regular monitoring of their health conditions.
Hospital-based retrospective follow-up study was conducted at chronic follow-up clinic of University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia among newly diagnosed type 2 diabetic patients who are enrolled between January 1, 2014, and December 31, 2019.
The study was conducted at chronic follow-up clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, which is found in Gondar town. Gondar town is located in North Gondar zone of Amhara Nation Regional State. Gondar town is located 738 km from Addis Ababa, the capital city of Ethiopia, and 113 km from Bahir Dar, the capital city of Amhara Nation Regional State. University of Gondar is one of Ethiopia's main medical universities, and its comprehensive specialized hospital is one of the major teaching hospitals in the country. It is a referral center for specialized medical care for the entire region of Northwest Ethiopia. Gondar is one of the centers where there has been a sustained development of infrastructure to manage chronic diseases (diabetes, hypertension, cardiac diseases, etc.) in a way that effectively includes both urban and rural dwellers, through a network of urban and rural clinics centered on Gondar University Hospital). Diabetes care service is part of the chronic disease management program; routine diabetes care has been supervised by the same care team at both the central and rural clinics for more than 20 years. The hospital gives different inpatient and outpatient services, including chronic clinic follow up. Around 24,552 patients have chronic disease follow-up per year and the hospital has to provide DM follow up service for around 8800 DM patients who come from different areas, and from this figure around 5000 are adult type 2 DM adults aged 18 years and above. The study was conducted from October 15-Nov. 15, 2021, among adult with newly diagnosed type 2 diabetes patients.
Diabetic retinopathy: Diabetic retinopathy was defined as a micro vascular complication of diabetes that was evaluated by clinical examination or indirect ophthalmoscopy by ophthalmologists and classified as present (yes) or absent (no) from the charts based on ophthalmologist decision [21].
Time to DR: Time to DR was the time gap in years between diagnoses of diabetes mellitus and first episode of DR [21].
Censored: Patients, who did not experience DR until the end of the study, who died or lost to follow up before experiencing DRI within the study period [21].
Event: The occurrence of DR from type 2 DM patients during the follow-up period [21].
Body mass index: Body mass index was defined as physiologic factors that measured in weight in kilograms per square meter of height (kg/m2) and was subdivided as low (low < 18.5 kg/m2, normal (18.5-24.9 kg/m2) and high (≥ 25 kg/m2) according to World Health Organization criteria [22].
Hypertension: Hypertension was defined as an average systolic/diastolic blood pressure of 140/90 mmHg or higher taken on two or more separate days and the measurement was taken from record review [23].
Glycemic control level: It was good glycemic control when fast blood sugar (FBS) was below 130 mg/dL and above indicated value was regarded as poor [24].
Data of cohorts was extracted from medical record by using pre tested structured checklist which was taken from previous studies. The checklist contains socio-demographic, baseline clinical and treatment-related factors. Forms used for laboratory requests, follow-up card, DM registration logbook, and patient cards were reviewed. After taking medical record number of diabetic patients from chronic care follow-up clinic, the patient folder was drawn from card room. The record reviews were done by two Bachelor of Science (BSc) nurses and facilitated by principal investigators. Training was given for data extractors before extraction; pre test was done on 5% of patients. To prevent recollection of data, a commonly agreed code by data collectors was given after reviewing and collecting data from each patient's chart. The outcome of each patient was dichotomized as censored or develops DR. For data quality, the data collection checklist was pre-tested to check the completeness of data items on 5% [20] patient charts before the actual data collection. Two-day training was given for data collectors for the description of the questionnaire and the way they collect data from the patient chart. Each component of the checklist was discussed clearly for data collectors. The data collection process was monitored closely by the supervisor. Finally, the completeness of the checklist was checked.
After the data checked for its consistency and completeness, it was coded and entered into Epi info version 7.2.2.6 by the principal investigator and was exported to Stata 14 for analysis. A statistical summary was used to describe socio-demographic, clinical, and treatment-related variables of the study. The occurrence of DR Incidence was calculated and the rate was calculated for the study period. Incidence rate was calculated by dividing the numbers of new DR cases occurring during the follow-up period to total person-time observation and expressed as per 1000 person-year observation. Log-rank test and Kaplan Meier curve were used to compare different categories of survival probability.
PH assumption was checked graphically and with Schoenfeld residual test (p-value = 0.2042) and Goodness of fit of the model was assessed by using the Cox-Snell residual technique. After applying bivariable analysis, those variables with p-value < 0.2 were entered into the multivariable Cox proportional hazard model to identify predictors of DR. 95% confidence interval of hazard ratio was computed and variable having p-value < 0.05 in the multivariable Cox proportional hazards model was considered as independent predictors of DR.
From 403 reviewed patient charts, 400 were included in the analysis. Of these 60.25% were males. The median and standard deviation of the age of the study participants was 50.5 ± 13.3. Among the study participants 77.5% were married, more than half were urban dwellers and 18.25% were government employees. Regarding the clinical factors that were identified about 56.25% had a history of hypertension, about 25.75% had congestive heart failure, about 17% had diabetic neuropathy, about 9.5% had chronic kidney disease. Regarding on treatment related factors about 46.75% of patients were taking Aspirin exposure and about 32.25% were exposed to Insulin medication (Table 1). A total of 400 patients were followed for 1081.603 person-years. The median survival time of patients to experience the first episode of DR was 30.4 months with a minimum & maximum of 0.0333 & 71.867 months follow up, respectively. During the follow-up, a total of 78 patients developed DR. 19.5% (95% CI; 16.2-23.8) developed DR. Overall, incidence density was 6 per1000 person-year observations (Figure 1).
Table 1: Socio-demographic, clinical and laboratory and treatment factors of adults with newly diagnosed type 2 diabetes patients at chronic follow-up clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2020 (n = 400). View Table 1
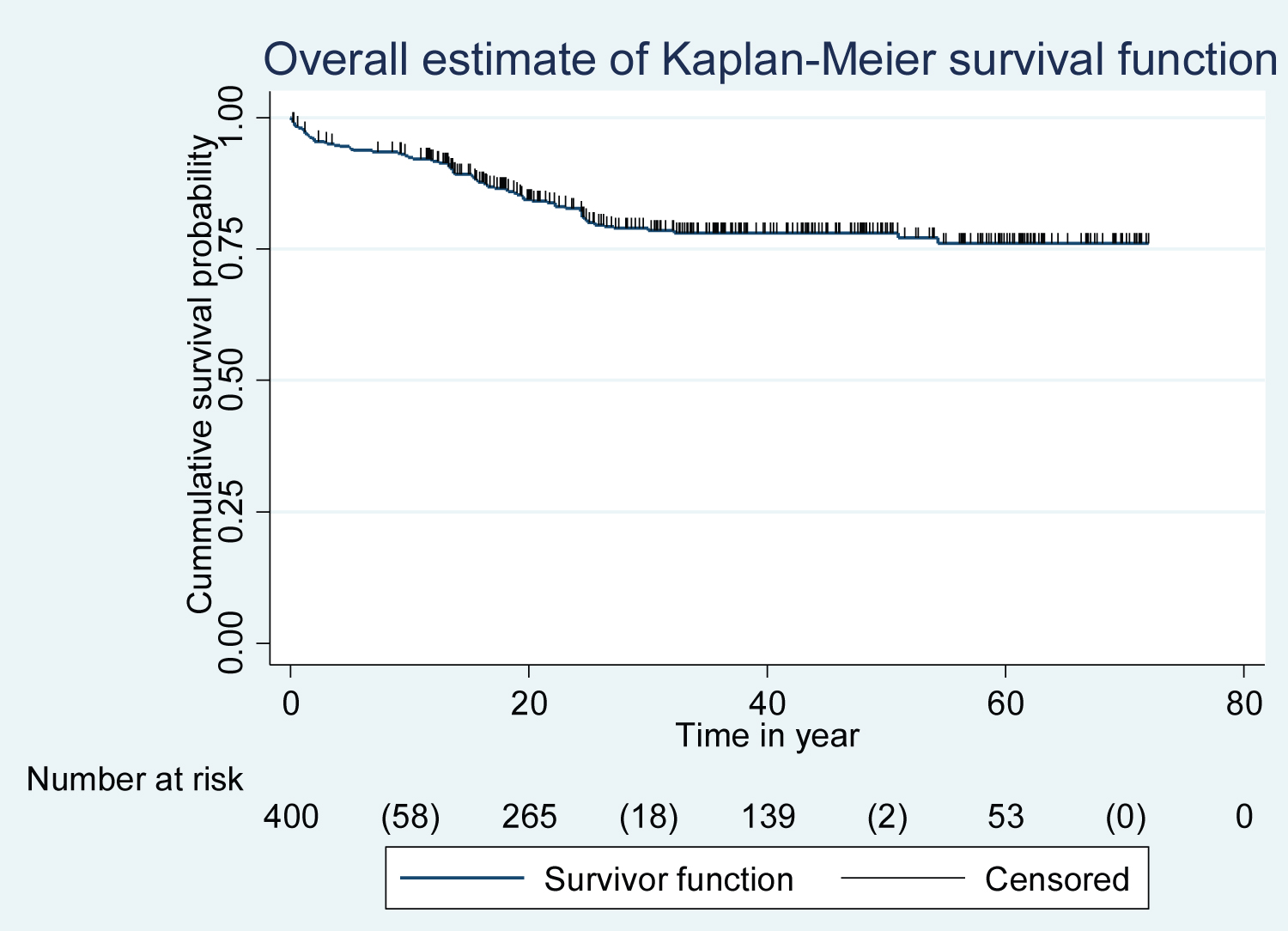 Figure 1: Kaplan-Meier curve of DR-free survival probability among type 2 diabetes patients at chronic follow-up clinic of
University of Gondar Comprehensive Specialized Hospital from January 1, 2014, to December 31, 2019.
View Figure 1
Figure 1: Kaplan-Meier curve of DR-free survival probability among type 2 diabetes patients at chronic follow-up clinic of
University of Gondar Comprehensive Specialized Hospital from January 1, 2014, to December 31, 2019.
View Figure 1
In bivariable analysis variables having P-value < 0.2 were entered in a multivariable Cox proportional hazards model to identify predictors of DR. The bivariable Cox regression analysis showed that congestive heart failure, chronic kidney disease, hypertension, stroke, aspirin exposure, diabetic neuropathy, HBA1c and uncontrolled DM were significant predictors of DR. However, after adjusting for confounders in multivariable analysis using Cox-regression model Congestive heart failure [AHR: 2.53(95%CI; 1.49, 4.29)], chronic kidney disease [AHR: 5.02 (95%CI; 2.73, 9.26)], hypertension[AHR: 2.07(95%CI; 1.17, 2.890)], and HBA1c ≥ 7% [AHR: 10.5 (95%CI; 5.6, 19.6)] were found to be predictors of DR among type 2 adult DM patients (Table 2 and Figure 2).
Table 2: Cox regression analysis of predictors of DR among cohorts of type 2 diabetes patients at chronic follow-up clinic of University of Gondar Comprehensive Specialized Hospital, from January 1, 2014, to December 31, 2019 (n = 400). View Table 2
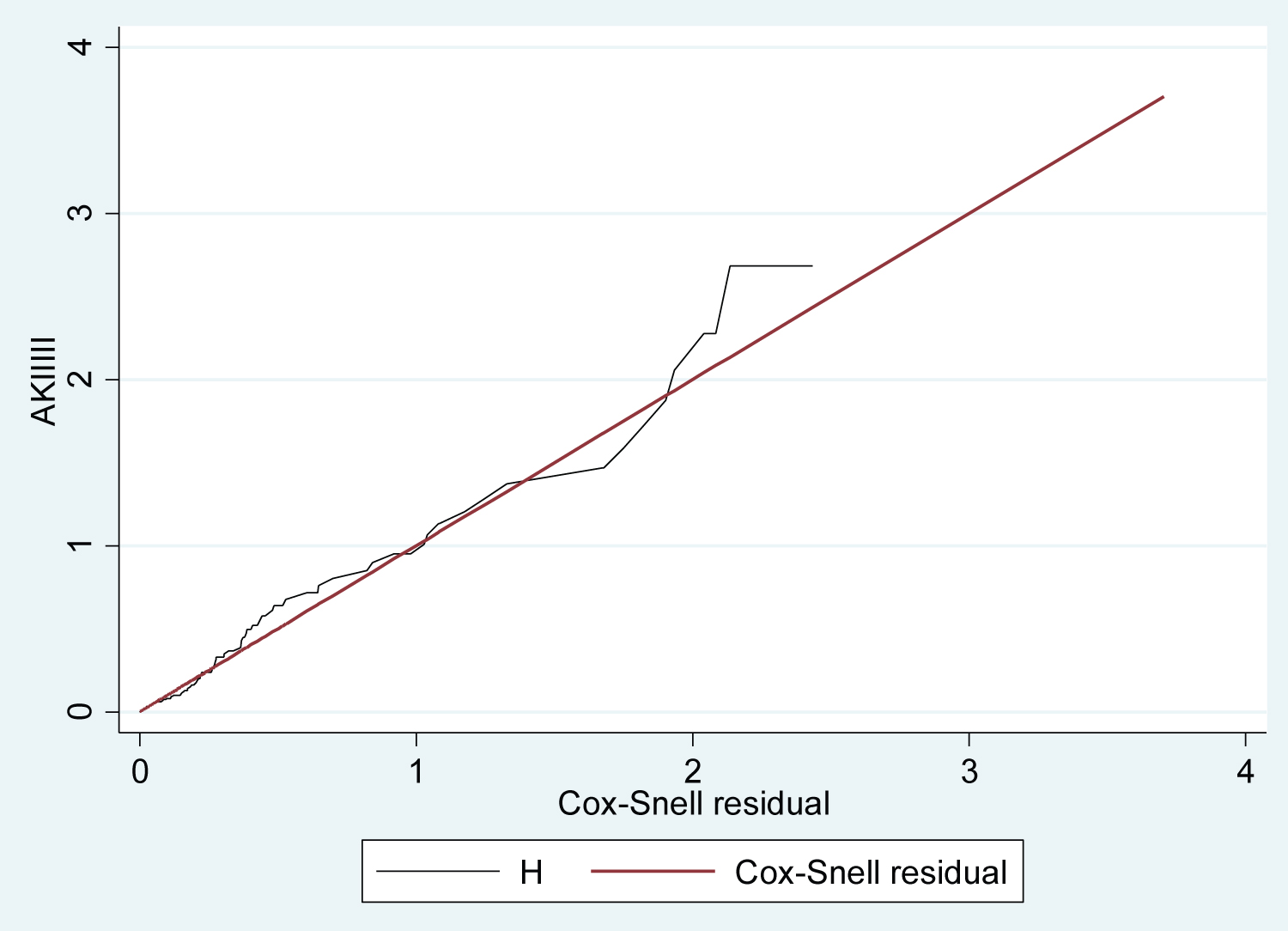 Figure 2: Cox-Snell residuals for Cox- regression PH models of newly diagnosed type 2 diabetes Patients at chronic
follow-up clinic of University of Gondar Comprehensive Specialized Hospital, from January 2014 to December 2019.
View Figure 2
Figure 2: Cox-Snell residuals for Cox- regression PH models of newly diagnosed type 2 diabetes Patients at chronic
follow-up clinic of University of Gondar Comprehensive Specialized Hospital, from January 2014 to December 2019.
View Figure 2
Log-rank test of equality of survival for the different categories of explanatory variables was done, and congestive heart failure, chronic kidney disease, hypertension, and HBA1c, were predictors of DR among type 2 diabetes patients.
Diabetic retinopathy is a serious problem and the leading cause of morbidity and mortality among adults with type 2 diabetes patients. This study investigated the incidence and predictors of diabetic retinopathy among type 2 DM patients at University of Gondar Comprehensive Specialized Hospital, Ethiopia. A total of four factors were identified as the predictors of DR in type 2 diabetes patients. These factors included hypertension, congestive heart failure, chronic kidney disease and HBA1c. The current study showed that the incidence of DR among type 2 diabetes patients was 19.5% (95% CI; 16.2-23.8) with the median survival time of 30.4 months. The finding of this study was in line with a study conducted in Jimma University Medical Center, Southwest Ethiopia 20.15% [21], and in Tikur Anbesa Hospital, Ethiopia 18.57% [15].
However, the finding of this study revealed that the incidence was lower than in a study done in United Kingdom which shows the incidence to be 11.64 per 1000 people and in Bangladesh the incidence found to be 50.6%, the discrepancy might be, due to the difference in demographic characteristics of study participants, and study setting [25,26]. The result is lower than a prospective follow-up study conducted in Spain indicated the incidence was 26.49%, the variation might be, due to difference in study design, sample size difference, the difference in median follow-up time duration, and socio-economic difference [27]. The result is lower than a retrospective follow up study conducted in South Africa which shows cumulative incidence of DR was 47 cases per 1,000 persons, the variation could be due to longer duration of follow-up time duration (7 year follow-up study), sample size difference, and outcome ascertainment difference [16]. The result is lower than a Longitudinal follow-up study conducted in Arbaminch General Hospital; Gamo Gofa Zone, Ethiopia which revealed the Overall incidence of DR was ~36 cases per 1000 patients per year, the possible reason for the discrepancy could be due to study design, and variation in duration of follow-up [28].
The result is higher than a prospective cohort study done in China revealed that the incidence density of diabetic retinopathy (DR) among type 2 diabetic patients was 1.81 cases per 1000 person-year, the discrepancy could be due to study design difference (prospective cohort study) and sample size difference [29].
The result is higher than a cohort study done in united states which shows the incidence found to be 7.2%, the discrepancy might be due to difference in demographic characteristics of study participants (include age > 21) and difference in early diagnosis and initiation of follow up of diabetic patients, good quality in health care systems and presence of strict monitoring of complications in united states may decrease the incidence of DR [30].
The finding of this study was higher than the findings of studies done Spain 8.07% (95% CI = 7.04-9.22), the variation might be, due to the presence of quality of care delivered for type 2 DM patients in Spain might contribute for a lower incidence of DR, the difference in study design (prospective follow up study) and the difference in contextual differences between the two countries [31].
This study assessed the risk of diabetic retinopathy related to socio-demographic, clinical and laboratory, and treatment related characteristics of the patients based on the records taken from their medical follow-up chart. Factors hypertension, congestive heart failure, HBA1c, and chronic kidney disease were found to be significant predictors of diabetic retinopathy. In this study, we have found that hypertension was independently associated with DR. Patients with hypertension had 2.07 times higher risk to develop DR than patients without hypertension [AHR: 2.07 (95%CI; 1.17, 2.89)] after adjusting of multiple confounders. The finding was consistent with studies conducted in Taiwan [32], Dessie, Ethiopia [24], Jimma University Medical Center, Southwest Ethiopia [21], and China [29]. This might be because in hypertension case the renin-angiotensin system was activated by chronic hyperglycemia, and then the vitreous fluid level of Angiotensin II (AII) was elevated in patients with PDR and diabetic macular edema. AII increased vascular permeability and promoted neovascularization finally leads to DR [33].
This study found that the expected hazard ratio of diabetic retinopathy was 2.53 times higher in patients with congestive heart failure among type 2 DM patients than in patients without congestive heart failure while keeping other covariates constant[AHR: 2.53 (95%CI; 1.49, 4.29)]. This might be associated with congestive heart failure among diabetes patients face for the presence of microangiopathy in the heart was reported to show thickening of the capillary basement membrane, microvascular spasm, and capillary microaneurysms resulting in retinal hemorrhage [34]. This study found that patients with chronic kidney disease were 5.02 times at risk of developing DR among type 2 DM patients than patients without chronic kidney disease [AHR: 5.02(95%CI; 2.73, 9.26)]. This might be related to Retinal pathologic features are associated with inflammatory processes in CKD there are inflammatory processes leading to circulatory abnormalities and reduced vascular reactivity and involve thickening of retinal basement membrane causing DR [35]. In this study, patients with HBA1c ≥ 7% were 10.5 times at higher risk of developing DR among patients with HBA1c < 7% [AHR: 10.5(95%CI; 5.60, 19.9)]. This finding was in concordance with studies done in China [29], and Madrid (Spain) [31]. This might be due to T2D patients who had abnormal level of HbA1c are more frequently prone for hypertension and other micro vascular complications including increase the incidence of DR [36].
One of the major limitations of the current study is the absence of institutional and behavioral factors, which may underestimate the effects and individual variations in the development of diabetes retinopathy. Secondly Because of the retrospective nature of the study, some important complications of diabetes that had a significant association with DR, like chronic kidney disease were missed since we used chart review to obtain the data.
Extracted information's were recorded in the past at the time when a patient came to the health facility, so the collected data were not depended on patient's memory and it minimized recall bias.
In this retrospective follow-up study, findings showed that the incidence of diabetic retinopathy among type 2 diabetes patients at chronic follow-up clinic of University of Gondar Comprehensive Specialized Hospital was high. Hypertension, congestive heart failure, chronic kidney disease, and HBA1c, were predictors of diabetic retinopathy among type 2 DM patients. In light of this finding, in addition to the routine care, especial emphasis should be given for patients with heart failure, chronic kidney disease, high baseline BP (> 140/90 mmHg) and high baseline HBA1c (≥ 7%). Knowing and controlling these factors should be routinely examined, evaluated and recorded. It would be better if health professionals in the DM follow up clinics strive to reduce the incidence of DR through enhancing quality of care and patients' self-care practice. They should provide eye evaluation service as recommended by the WHO at least twice annually for all diabetic patients. Even though the recommended follow up is different based on blood glucose control status it would be better if patients check their general assessment in each follow up especially related to ophthalmic conditions. Finally, prospective study is highly recommended to identify real life determinants of DR.
Ethical clearance and approval were obtained from the ethical review committee of the School of Nursing to behaving with the Institutional Review Board (IRB) of the University of Gondar. Upon this clearance, additional written permission to conduct the study on medical records of DM patients was obtained from the coordinator of chronic clinic follow-up of the University of Gondar Comprehensive Specialized Hospital. Confidentiality of information was maintained through refrain from the recording of the patient's name of the used chart and keeping data anonymous. The information didn't use other than the study purpose.
Our gratitude goes to the University of Gondar, College of Health and Medical Sciences for all necessary services and we appreciate the support from the hospital's administrations and data collector.
There is no funding to report.
The authors declare no competing of interest.