Most children diagnosed with ASD will present with late onset verbal communication, and at least one third of these children will remain minimally or completely nonverbal throughout their lifespan, speaking few or no words. Challenges with verbal language can negatively affect many areas, including socialization, academics, independent living and employment. The objective of this paper was to systematically review interventions for the treatment of nonverbal and minimally verbal individuals with ASD. This review exclusively selected studies that targeted verbal communication in minimally and nonverbal individuals diagnosed with ASD. The interventions provided, the outcomes of these interventions, measures used to assess change, and pre- post measures were included.
What is the current evidence base for interventions for non- and minimally verbal individuals with Autism Spectrum Disorder (ASD)?
A literature search was conducted through ProQuest (Mendeley reference manager). Articles were extrapolated from seventy data bases. Databases surveyed included Medline, Periodicals Archive Online, Periodicals Index Online, PRISMA Database, ProQuest Central, PsycARTICLES and PsycINFO. A complete list of all databases included is available on ProQuest (http://tls.search.proquest.com/titlelist/jsp/list/tlsSingle.jsp?productId=10000255).
The publication span entered was 1960 to 2018. Reliability for coding was examined and was uniformly above 90% concordance.
Our search yielded 2,007 articles, of which 29 studies met our inclusion criteria. Inclusion criteria included: (1) Research Design: Studies that involved systematic, experimentally controlled investigations, such as randomized controlled trials, quasi-experimental designs, and single-case designs; (2) Diagnosis: only studies that included minimally verbal, nonverbal, and preverbal participants diagnosed with ASD were included; and (3) Targeted verbal communication: the goal of the intervention was to initiate or improve verbal communication, including the production of words, word attempts, or sounds. This review found that there was a wide variety of interventions provided, comparisons across interventions were lacking, and dependent measures varied considerably.
Presently, pediatricians and service providers are unable to provide evidence-based treatment recommendations regarding speech and language interventions for non- and minimally verbal individuals with ASD. Limited evidence suggests that verbal-focused treatments in natural settings with parent participation is effective, as research regarding the most effective and efficient interventions for this high need group is lacking. Lack of uniformity in regard to dependent and pre- post measures, participant ages, and description of interventions implemented make comparing outcomes across studies difficult. Uniform standards for identifying MV and NV children with ASD is needed in future studies and additional details on the intervention procedures in futures studies is also needed.
Autism, Nonverbal, Minimally verbal, Expressive words, Communication treatment
ASD: Autism Spectrum Disorder; MV: Minimally-Verbal; NV: Non-Verbal
In this systematic review, no consistencies across intervention recommendations were identified. For example, some studies recommended the use of augmentative programs (signs/pictures/computer programs) along with or before targeting verbal communication whereas other studies indicated that augmentative programs are not necessary. Regardless of program, most recommend the use of naturalistic intervention procedures.
Currently, there are no consistent recommendations for pediatricians and practitioners to make for treating nonverbal and minimally verbal children with ASD. Systematic intervention research for this population is needed.
Parents rely on pediatricians and service providers for referral to effective interventions when their child is diagnosed ASD. Although social and behavioral symptoms of ASD may manifest in the first year of life, the delayed onset of language is the most common reason for a diagnostic consultation by parents [1] and is one of the most concerning symptoms of ASD [2]. Although many children with ASD are "high functioning" and communicate verbally, a high proportion will persist as nonverbal or minimally verbal.
Recently, the literature has highlighted the pressing need to study children with ASD who have extremely limited verbal abilities, identifying this subgroup of ASD as grossly under-represented in the intervention literature [3-5]. That is, in the last almost 60 years, relatively few studies have focused on intervention for targeting first word production in this population after the age of two years [6]. In the absence of specific guidelines and definitive strategies supported by objective data, children with ASD may receive ineffective or misguided interventions. Training programs, clinics, and schools cannot deliver best practices, and children with ASD may suffer the consequences of an inability to verbally communicate in the absence of a credible evidence base. To be clear, nearly all children with ASD are nonverbal or low verbal as toddlers, but many of these children become verbal before age three years. The focus of this review is on children with ASD who persist as nonverbal or low verbal after two years of age.
According to the DSM-5 [7], a defining characteristic of ASD is persistent deficits in social communication. Typically developing children produce first words between 10 and 18 months, whereas children with ASD are reported to do so at an average age of 36 months [8]. Further, a third of children diagnosed with ASD will remain minimally verbal or totally nonverbal [9].
The late onset of communication in children who will be subsequently diagnosed with ASD is the primary reason parents bring their child in for initial evaluation [1]. Challenges with social communication along with restricted and repetitive behaviors (RRBs) are required for the diagnosis of ASD. RRBs often present as repetitive play in young children and few interests in older individuals. Challenges with socialization, particularly when interacting with peers, tend to persist across the lifespan, even for those who develop age appropriate communication. ASD encompasses a largely heterogeneous group, and symptomology varies considerably across individuals ranging from nonverbal/minimally verbal to highly verbal. RRBs range from repetitive motor behaviors to excessive interest in particular, often idiosyncratic topics. Those children with ASD falling into the persistent NV and MV subtype also have a higher probability of generally slower intellectual development and a higher incidence of behavioral sequelae.
This systematic review analyzes current intervention studies for this population, outcomes, and measures used to assess change. We reviewed studies since 1960 when interventions for ASD were first published. Outcomes are analyzed and recommendations are provided.
A literature search with a publication span from 1960 to 2018 was executed using Vanderbilt's ProQuest using Mendeley reference manager (https://www.mendeley.com/reference-management/reference-manager) from seventy data bases using the key words "autism", "autistic", "Asperger", "autisms", or "ASD" AND "minimally verbal", "minimally fluent", "preverbal", "pre-verbal", "nonverbal", or "non-verbal" "mute" AND "vocabulary", "words", "communication", "language", or "lexical." ProQuest databases surveyed included Medline, Periodicals Archive Online, Periodicals Index Online, PRISMA Database, ProQuest Central, PsycARTICLES and PsycINFO. A complete list of all databases included is available at ProQuest (http://tls.search.proquest.com/titlelist/jsp/list/tlsSingle.jsp?productId=10000255). This search yielded a total of 2007 articles. Only articles with interventions provided in English were included because the authors were not qualified to review interventions in other languages. Duplicates were removed, and a title screening to exclude articles that did not include nonverbal or minimally verbal individuals or did not provide treatment yielded 237 articles with 90% reliability for inter-reviewer article triage.
Only scholarly articles and peer-reviewed articles were included. Reports, dissertations, conference papers, and/or proceedings were not included. Additionally, articles were excluded if the titles indicated that they (a) Were assessment only or other non-treatment articles; (b) Did not target verbal behavior(s) (e.g., receptive communication, reading, vision); (c) Included highly verbal participants or advanced communication goals (e.g., Asperger Disorder, conversation, language structures); (d) Were commentaries, book reviews, reviews of the literature, errata; (e) Had fewer than two participants; or (f) Were conducted in a spoken language other than English. The final criterion was adopted due to the authors' and coders' limited expertise in the pantheon of spoken languages appearing in the topic search rather than any prior assumption as to the relative advantages or disadvantages of any particular spoken language.
First, all of the titles were independently read and screened by the first (primary coder) and last (reliability coder) authors, who had the most experience in the field, using the following inclusion criteria:
1. Titles that included "minimally verbal" children with ASD
2. Titles that included "nonverbal" children with ASD
3. Treatment/intervention articles targeting verbal communication skills
Duplicates were removed, yielding a total of 1,231 articles. This title search yielded 237 articles out of 1,231. Reliability for the title screen of the articles was 90%. Articles from the title screening that were included by only one coder (either the primary or reliability coder) were included for the abstract screening.
Following the title search, abstracts from the 237 articles were screened using the additional following specific inclusion and exclusion criteria:
Research design: Studies that involved systematic, experimentally controlled investigation intervention were included. Example research designs meeting inclusion criteria were randomized controlled trials, quasi-experimental designs, and single-case designs with at least two participants. Uncontrolled case studies (e.g., N = 1) were excluded from this review. In order to ensure the study was evaluating intervention effectiveness, at least one dependent variable had to be a child outcome measure.
Treatment: Only articles that implemented an intervention for (or that resulted in) expressive verbal communication or interventions to evoke first words as the independent variable were included.
Diagnosis: Participants, or the majority of participants in the study, were required to have been diagnosed with ASD, and the participants diagnosed with ASD and had to have been identified as minimally verbal, nonverbal, preverbal or another description of the communication abilities of the participants relating to the production of first words.
Measurement: Included studies involved verbal behavior (words, word attempts, or sounds) as a dependent variable. Nonverbal modes of communication-augmentative, sign language, etc.-that did not include verbal output or explicitly state that the approach was used as a bridge to verbal communication were excluded. That is, articles that included picture supports, or other visual symbols were included only if the outcome dependent measure(s) were focused on verbal communication. Similarly, voice generating devices (e.g., touch talkers, DynaVox systems) were excluded unless the outcome measure(s) focused on verbal communication by the child.
Participants: Individuals diagnosed with Asperger Disorder, PDD-NOS, or whose target behavior included socialization, receptive language, non-verbal communication exclusively, or whose treatment program included an augmentative system or nonverbal communicative system (e.g., pointing) that were not explicitly a precursor to verbal speech were also excluded.
The first (primary coder) and last (reliability coder) authors screened the first 50 articles with 96% reliability. The second and third authors screened the first 50 abstracts with 87% reliability. Next, half of the abstracts from the 237 included from the title review were screened by the first (primary coder) and fourth (reliability coder) author and the remainder were screened by the second (primary coder) and third (reliability coder) author. The reliability for the abstract selection was 89%. Any abstracts that were included by only one coder (either the primary or reliability coder) were included for the full article review. The abstract search yielded 67 articles.
These 67 articles that specified intervention to individuals who were nonverbal or minimally verbal were read in full and analyzed for a parent education program. Nineteen of the 67 articles (28%) were reviewed for reliability purposes relating to inclusion/exclusion. During the write-up, the first author found two articles that appeared to meet our exclusion criteria. The last author read these articles and concurred that they should be excluded from the analysis (one was conducted in a foreign language, and the other targeted nonverbal social behavior in individuals with Asperger Disorder who were highly verbal). Thus, reliability on inclusion/exclusion was 89%.
The 29 articles meeting the inclusion criteria were then fully reviewed and coded for: (a) Age of participants/sample size/male-female inclusion rates; (b) Dependent measures; (d) Pre- post intervention measures; (d) Descriptions of treatment provided; and (e) Study outcome. Following the creation of the summary table (Table 1), an independent coder re-checked articles for accuracy. Numerical findings in the Results were checked, and five that were below 100% were analyzed by another author independently and the matching score was reported.
Table 1: Treatments used in the studies for nonverbal and minimally-verbal children with ASD. View Table 1
Four studies used the same data base (same participants), with similar findings, therefore only one study with the largest N was used in the calculations [10-13]. There were 649 unique participants with ASD that received intervention in the 26 independent studies. Twenty-four of the studies reported number of males and females included; 84% of participants were males (n = 496) and 16% of participants were females (n = 91). Gender was not reported for 62 participants. The age span of the participants ranged from 1 year 4 months to 23 years. A closer analysis revealed that eight studies exclusively targeted children in the toddler/preschool years (under 4 years 11 months), with a total of 295 participants [14-21]. Eight studies included participants exclusively in elementary school (ages 5-12;11) with 115 participants [10,22-33]. Participants in nine studies [6,31-37] included a combination of preschool and elementary school aged children with 220 participants. The remaining study included a combination of elementary/adolescents/adults with 19 participants [38]. In regard to the assessment of change measures, most studies (77%) had direct measures of speech sounds, word approximations, words, or utterances. Two studies only reported standardized test scores (PEP-R, CDI/Mullen/Vineland) [20,36]. One study measured behaviors related to communication (social engagement/affect) and described each participant's outcome [19].
Most studies reported improvements in communication. In regard to interventions for toddler and preschool children, seven of the eight studies used strategies based on Applied Behavior Analysis (ABA); two used traditional ABA discrete trials procedures such as modeling, shaping, and rewarding desired behavior [14,16], and three studies used Pivotal Response Treatment (PRT) that focuses on motivational components (e.g., child choice, natural rewards, task variation, rewarding attempts) [17,18,20]. One study used a parent-mediated intervention that focused on parent responsiveness to child communication and using communication during action routines [15]. The remaining study targeted engagement in natural environments, social communication, and emotional regulation [21]. One study compared a picture system (PECS) to a verbal only intervention (PRT) and found no group differences [20]. Another study compared group parent education with individual parent education and found that, while all children improved, the individualized parent education group demonstrated greater improvements in communicative areas [21].
For elementary school-aged children seven of the twelve studies added some type of augmentative device, such as pictures, computer, gestures, or signs in addition to verbal communication. Five studies focused on verbal communication without an augmentative system. Of those five studies that used various verbal approaches (pre-linguistic milieu Teaching [22], NLP/PRT [35], Melodic Intonation Treatment (MIT) [25], a non-labeled intervention that focused on modeling/attention/hearing tube/manual manipulation, and auditory motor mapping [37]) all resulted in improvements in verbal communication. However, MIT participants did not show significantly greater outcomes than those receiving a traditional treatment. In regard to interventions that used a combination of treatments, one study found that a combination of a speech generating device (SGD) and verbal production was more effective than an intervention focusing on joint attention, play, engagement & regulation (JASPER), with a verbal component [10].
Another study that used a picture system of communication (PECS) found that some children improved in their use of requests (both verbal and with the picture cards), but PECS did not result in improvements in communication used for social purposes [33]. Further, the picture system did not enhance the verbal communication of the children who were already using some verbal communication at baseline. A study using simultaneous communication (speaking and signing together) compared with a verbal only approach found no difference between the verbal outcomes of the groups [24]. Finally, a study that compared sign alone, speech alone, sign with speech, and alternating sign and speech found that the only group that used significantly fewer spontaneous words was the sign only group [29].
Studies that included a combination of preschoolers and elementary school aged children did not use augmentative communication but, similar to the preschool studies, directly targeted communication. One used Auditory Motor Mapping Training alone and compared this with added Speech Repetition Therapy. The AMMT + SPT produced the best outcomes [30]. Several studies used ABA or naturalistic ABA procedures and those studies showed improvements in verbal communication (varied vocalizations, vocalizations, words) in all participants [22,34,36,37]. One study used the Treatment and Education of Autistic and Communication related handicapped Children program (TEACCH) but did not report communicative gains [36] and another compared the Denver Model to Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) techniques and showed greater gains with the Denver model [37].
Finally, the study that included a large age range (i.e., elementary/adolescents/adults) primarily included nonverbal participants and began with having the participants walk on uneven parallel bars above the ground then added pictures with signs and verbal modeling of the word [38]. After intervention researchers found improvements in sign use for all participants but only 7/19 participants learned some spoken words.
Moreover, this systematic review suggested that a majority of the participants in the studies, aged between 1;4 to 23 years, demonstrated communicative gains following intervention. Several studies suggested moderating factors. For example, children with higher skills at the start of intervention had a more positive response to the intervention. Measured pretreatment areas that were suggestive of more positive communicative outcomes included greater sound imitation, more mild symptoms of ASD, and the presence of social orienting. Additionally, the presence of functional language by age five was reported to be correlated with more positive outcomes in children with ASD. Overall, the level of evidence from these studies must be classified as preliminary or weak and the overall data available is quite limited, especially relative to that for verbal children with ASD.
Nonverbal and minimally verbal individuals with ASD arguably represent the phenotype with the greatest support needs; however, this subgroup has been largely understudied in the research literature. Our searches through nearly 60 years of research only yielded 29 studies (and only 26 with unique participants) that focused exclusively on verbal communication to nonverbal or minimally verbal individuals with ASD. Within this literature base, there was a variety of reasons that precluded us from making conclusive evidence-based recommendations and made it difficult to compare findings across studies. These included: (1) Definitions: A lack of uniform terminology for defining "nonverbal" and "minimally verbal" was noted across studies. Some classified individuals who could say a few words as "nonverbal" and other studies combined nonverbal and minimally verbal children in their research. Further, there was great heterogeneity in age groups with some studies focusing exclusively on preschool children (who could also be considered preverbal or prelinguistic) while other studies included elementary school aged children, adolescents, and adults. As such, the most effective interventions based on verbal status and age could not be determined due to a small number of studies in each area; (2) Measurement Systems: The reviewed studies varied greatly in how pretreatment behaviors were measured, how progress and outcomes were measured, and whether assessments included various settings and different communicative partners. The field requires a more uniform paradigm; standardized measures across settings would allow for more precise comparisons of procedures and systematic aggregation of findings across studies. Additionally, a greater understanding of prognostic pretreatment indicators (particularly in preschoolers) would be helpful in understanding the relative communicative gains of an intervention, moderating factors, and the likelihood of response to intervention; (3) Diversity of Interventions: Although the most common effective procedures were rooted in applied behavior analysis principles (ABA), there was great variability in intervention procedures within ABA (i.e., discrete trials, pivotal response training) and for non-ABA procedures (auditory-visual mapping, Melodic Intonation Therapy), again creating challenges in understanding best practices. Given these challenges, we were still able to make some general preliminary findings, as follow.
Grouping non- and minimally verbal children across age groups did result in some interesting patterns in the research within the limitations described previously: (1) A verbal only approach is recommended for toddlers and preschoolers. All studies showed improvements in verbal communication using a speech only approach for preschoolers. One study comparing an augmentative vs. a speech only approach did not show that a picture system resulted in greater improvements. One question in for nonverbal children with ASD has been whether the use of an augmentative system would facilitate expressive verbal communication. This review did not indicate this combination was differentially beneficial. (2) Research suggests that targeting pre-linguistic behaviors may not lead to improvements in verbal communication [17]. The most successful programs appeared to directly target verbal communication. Further research on learning trajectories and prelinguistic behaviors should help elucidate those who will become verbal and those prelinguistic areas that potentially could be taught to accomplish better outcomes for all children. (3) When children reach elementary school age, while a greater diversity in treatments was noted, more than half of the studies showed gains in communication using various communicative interventions without an augmentative device. Only one set of participants [10,12,13] (the same participants reported in four published studies) found that a combination of a speech generating device was more effective than intervention alone, however, their intervention was not solely focused on communication. As a whole, these results suggest that treatment focused on non-communication areas (e.g., play, joint attention, attentiveness) in combination with targeting verbal communication may not produce as large of gains in expressive communication as interventions that focus exclusively and directly on verbal communication.
More research is warranted in this area. (4) It does not appear necessary or helpful to manually manipulate the articulators during intervention for children with ASD (e.g., PROMPT). (5) Naturalistic interventions based on ABA procedures, providing considerable opportunities in everyday settings with a parent education component are the most well researched and currently appear to be most effective at producing expressive communication in preschool and elementary school aged children. (6) As a whole, the studies indicated that children who enter intervention at a higher level will also exit intervention at a higher level. Nonverbal children with higher levels of behaviors such as play, joint attention, sound imitation, gross motor imitation, attentiveness, socialization, along with less severe autism symptomology will begin talking sooner. Those with significant deficits in these areas are more likely to remain nonverbal.
In summary, this systematic review indicates the general paucity of intervention studies on minimally verbal or nonverbal children with ASD despite the long-standing high priority for developing effective treatments for these children (e.g., Interagency Council on Autism, 2011, 2017) [3]. The current lack of systematicity reduces available evidence-based treatment options. When comparing the definitions of the studies reviewed, one has to bear in mind that the considerable differences between the studies evaluated makes is difficult to extrapolate the existing studies to practice and to aggregate studies for meta analyses. Furthermore, studies using the same subject pools adversely affect the external validity of an intervention. Research should explicitly state whether the studies involve unique participants.
Despite these challenges, the current literature is a foundation to build future studies and systematic improvements are needed. Moreover, our attempt to accurately describe the current literature in regard to intervention recommendations for nonverbal and minimally verbal participants was hindered by the heterogeneity in the symptoms, varying ages, and different treatments and core lack of systematic, replicated intervention research paradigms that made it difficult to make definitive recommendations for intervention. We do acknowledge the possibility that some studies were missed in the analysis due to non-inclusion of the key words used but do point to the breadth of the original article catchment as reducing the likelihood that a large number of studies were missed. Future research is crucial for addressing the communication needs of the most severely impacted and underserved children with ASD (Figure 1) [39].
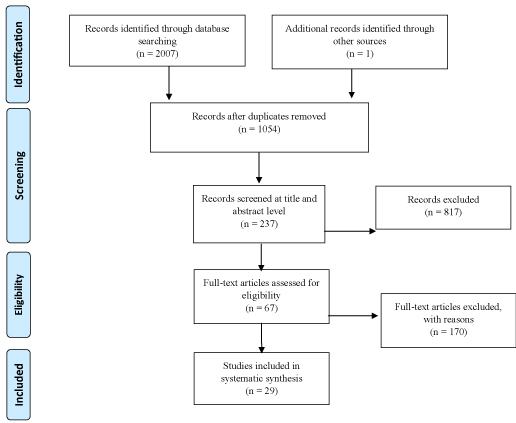 Figure 1: PRISMA 2009 flow diagram [39].
View Figure 1
Figure 1: PRISMA 2009 flow diagram [39].
View Figure 1
The authors wish to express gratitude to the Kind World Foundation, the Weitz Family Foundation, and the Scottish Rite Foundation of Nashville, Tennessee, USA for financial support of this review.