Methotrexate is an essential drug in the treatment of children with acute lymphoblastic leukemia. A complication of methotrexate includes neurotoxicity - it presents with signs and symptoms ranging from headache to stroke-like symptoms.
An 11-year-old girl with lymphoblastic lymphoma, who presented a history of leukoencephalopathy, which mimicked stroke one week after receiving high doses of intravenous methotrexate. The patient's symptoms completely improved within two days without sequels. Ten days after a new administration of methotrexate presented right-side hemiparesis and dysarthria. Again, with full resolution. Brain magnetic resonance scan was indispensable for diagnosis. The patient was discharged home without neurological symptoms.
Neurotoxicity associated with methotrexate is transient and most patients continue to receive this therapy without intercurrences. It is important that healthcare professionals recognize this entity.
Methotrexate, Neurotoxicity, Lymphoblastic lymphoma, Pseudo-stroke, Dextromethorphan
The acute lymphoblastic lymphoma (ALL) is the most common form of leukemia in children, being its treatment one of the leading causes of death associated to cancer [1,2].
The therapeutic protocol in use to treat this disease in Porto's IPO is the one indicated by the EORTC-CLG (the European Organization for Research and Treatment of Cancer - Children Leukemia Group). The metastasis of the central nervous system (CNS) is quite frequent. Since the 90s, in the majority of the first line treatment protocols used as prophylaxis to prevent CNS metastasis, holo-cranial radiotherapy has been replaced by high doses of intravenous methotrexate (HD-MTX) as it crosses the hematoencephalic barrier, eradicating and protecting the CNS against the leukemic cells. In the above-mentioned protocol, the CNS prophylaxis is realized by giving 4 doses of HD-MTX (5 g/m2), with calcium folinate (as safety, after 42 hours from the MTX) every 15 days, associated to the intrathecal therapy (rest period).
However, as with any drug, its usage is associated with some side effects: Neurological toxicity, skin toxicity, renal toxicity, hematological toxicity and hepatic toxicity. The neurological toxicity prevalence ranges between 2.3% and 15% and it can be characterized either by an acute or prolonged picture [2,3].
The dextromethorphan (lipophilic amine and N-methyl-D-aspartate NMDA receptor antagonist) crosses the hematoencephalic barrier and once given to patients with neurotoxicity it seems to have some positive effect [4,5].
An 11-years-old teenager with lymphoblatic lymphoma T, on treatment as per EORTC-CLG group AR2 protocol, under intensive chemotherapy (rest period). One week after the second cycle of HD-MTX (with adequate MTX clearance) the patient has been admitted for a transitory episode of right hemiparesis (including face) and ataxia. Two days later the teenager developed a transitory language alteration and dysarthria. During this context it has been performed a cranial-cephalic MRI that highlighted a small lesion on the left corona radiata with hyper signals on the long TR sequences and with restriction on the water molecules diffusion, suggesting an acute ischemic lesion of the left middle cerebral artery (MCA) in the perforating arteries area; an ecoDoppler of the neck vessels has been performed without any relevant outcome and a Bubbel test, that didn't show the presence of a right-left shunt. The neurological deficits resolved spontaneously until discharge.
After the episode the patient received, as planned, the third HD-MTX cycle of the rest period without any complication during this treatment. However, ten days after, the patient started developing new focal neurological deficits, presenting at the neurological examination a left central facial paraesthesia, paresthesias of the left limbs, dysarthria and dysphagia. The exam results weren't compatible with a vascular lesion, introducing the hypothesis of a case of neurotoxicity induced by MTX.
The patient did another cranial-cephalic MRI that showed, in addition to the left corona radiata lesion (not in recent stage), an alteration of the signal intensity on the right corona radiata. The patient presented again a progressive and spontaneous resolution of the neurological deficits and has been discharged four days after, completely asymptomatic. It has been decided to do not administer the fourth cycle of HD-MTX and to carry on with the remaining treatment. After two months the protocol maintenance phase started, consisting of administering HD-MTX (5 g/m2) every 10 weeks [6].
Taking into account the toxicity registered during the intensive stage of treatment and with the aim to do not suspend the administration of this drug, important for the protection of the CNS, it has been opted to lower the dosage (with later increase according to the clinical and imaging evolution) and associate dextromethorphan (20 mg, 3 times a day). This way, the first cycle of the maintenance stage has been realized with 10% of the total dose of HD-MTX planned in the protocol (500 mg/m2), without any side effect registered, particularly neurological. The cranial-cephalic MRI realized 10 days after wasn't showing any change, highlighting just the known lesions on the left and right corona radiata.
On the following cycles, as no side effect had been recorded, the dosage was gradually increased about 10% until reaching the dosage of 3.5 g/m2. After this stage, as the HD-MTX clearance started to become slower than expected, there hasn't been any more increasing in the drug dosage.
After each cycle, was performed an imaging valuation with cranial-cephalic MRI, that always showed the already described lesions unchanged.
The MTX (4-Amino-10-methylfolic acid) is the folic acid antagonist. This drug is used in the lymphoblastic lymphoma T treatment to prevent or treat lesions on the CNS, either endovenously on high doses or intrathecal administration. The MTX restricts the dihydrofolate reductase, forbidding the folic acid transformation into tetrahydrofolic acid (essencial for the homocysteine remethylation into methionine), and consequently blocks the cellular replication. It's important to highlight that with the application of this drug it has been possible to reduce the usage of the holo-cranial radiotherapy and the associated side effects [3].
However, its usage with any other drug isn't harmless. The neurotoxicity is one of the side effects associated to the MTX usage and it can change according to the dosage, route and frequency of administration. The factors that increase the incidence risk are: High dosage, intrathecal administration and young age [2,3].
The probably responsible mechanisms for the neurotoxicity aren't clear yet but they are thought being multi-factorial [2]. According to the literature, there could be and alteration of the folate homeostasis in the CNS and/or a direct neuronal lesion [1]. The following condition happens: The inhibition of the hydrofolate reductasis, caused by the MTX, affect the increment of the homocystein levels in the blood and in the liquor that consequently increase the homocystein levels. This way, not only this substance actuates as direct vascular toxic for the endothelium, but also its metabolism will actuate as agonist of the NMDAR, probably resulting from this condition the neurological findings associated to the neurotoxicity [1-3]. Moreover, a secondary neurological lesion could occur such as the adenosine releasing from the endothelial cells and fibroblasts [3]. Nowadays, it's stated that exists a genetic polymorphism associated to neurogenesis that could contribute to the neurotoxicity sensibility caused by the MTX - GSTP1, MTHFR, SHMT1 [1].
Some drugs such as trimethoprim/sulfamethoxazole, non-steroidal anti-inflammatory drugs, penicillin, proton pump inhibitors, acetylsalicylic acid and nitric oxide can lead to a delayed MTX clearance and increase its neurotoxicity; for these reasons they have to be avoided before and after the MTX administration on high doses [5,7,8] Figure 1).
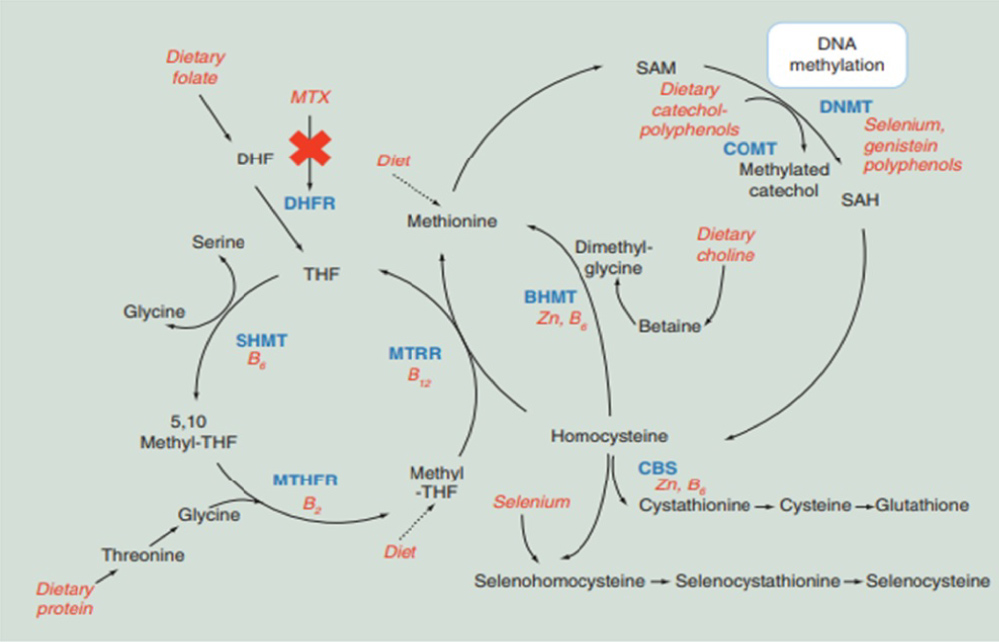 Figure 1: Probable reactions involved in the MTX associated toxicity [ CITATION For17 \l 2070].
Figure 1: Probable reactions involved in the MTX associated toxicity [ CITATION For17 \l 2070].
BHMT: Betaine-Homocysteine S-Methyltransferase; CBS: Cystathione Beta Synthase; COMT: Cystathionine Beta Synthase; DHF: Dihydrofolate; DHFR: Dihydrofolate Reductase; DNMT: DNA Methyltransferase; MTHFR: Methylenetetrahydrofolate Reductase; MTRR: Methionine Synthase Reductase; MTX: Methotrexate; SAH: S-Adenosylhomocysteine; SAM: S-Adenosylmethionine; SHMT: Serine Hydroxymethyltransferase; THF: Tetrahydrofolate.
View Figure 1
The neurotoxicity induced by the MTX can be acute, subacute or chronic. It's pointed out that can develop also cases of asymptomatic leukoencephalopathy that could persist exactly after completing the treatment [1]. Its presence is associated to the recurrent exposure to the MTX and exist cases of diffused necrotizing leukoencephalopathy as well [1].
The acute neurotoxicity is a neurological complication with an incidence between 3% and 11% and it mainly affects patients older than 10 years. It occurs hours after the administration of the drug and it manifests with drowsiness, confusion, headache, nausea, vomit and dizziness. The sub-acute neurotoxicity typically occurs between 2 and 14 days after the exposition to prolonged low doses of oral MTX, intrathecal MTX or HD-MTX and it manifests with convulsions, changing in vision, motor deficits, behavior alterations (lethargy) and stroke-like symptoms [1,2,5].
These events are usually transitories and the majority of patients receive the new treatment without complications [1].
The stroke-like symptoms presentation is a benign rare neurological complication, mainly described after the administration of intrathecal MTX. It simulates a transitory cerebral vascular ischemic accident associated with a focal sensory-motor deficit and a language alteration. Moreover, it can occur an oculomotor nerve palsy and ataxia. The evolution is characterized by a fluctuation of the symptom's intensity, with complete resolution within hours or days. The diagnosis is confirmed with a cranial-cephalic MRI.
The relapse risk after the MTX reintroduction in the same circumstances can occur between 10% and 56% of cases but it doesn't justify the exclusion of MTX in the treatment as more than 95% of patients with stroke-like side effects don't present permanent neurological deficit [3].
There are similar cases described and studies performed with antidotes such as aminophylline and dextromethorphan [1]. The aminophylline (inhibitory competitor of the adenosine receptors) still doesn't have a clear benefit, in spite of being one of the elective drugs for the secondary prophylaxis associated to the MTX induced toxicity; the dextromethorphan (DXM - non-competitive NMDA receptor antagonist, non-opioid morphine derivative) evidenced to be beneficial relatively to the neurological deficits caused by the MTX neurotoxicity, when used with the dosage of 1-2 mg/kg [2,4].
Its vantage rely on the ability of this drug to cross the hematoencefalic barrier and theoretically reduce the effects given by the homocysteine toxicity and other similar glutamate on the brain [4]. However, it doesn't exist now a formal indication approved by the Food and Drug Administration (FDA) about the DXM dosage to use on the treatment of neurotoxicity [4]. Other drugs that might going to be used are: Memantine and gabapentin (there are studies in vitro with positive results) [4].
In the case presented, the 11-years-old teenager showed a stroke-like clinical signs one week after the second cycle of HD-MTX - right hemiparesis, ataxia, dysarthria and aphasia with a complete resolution at about 48 hours after. Furthermore, the cranial-cephalic MRI identified results most likely associated to an acute ischemic lesion of the left MCA in the perforating arteries area.
The benignity and transitory nature of these episodes didn't establish a contraindication to continue the treatment, so the teenager carried on with the 3° cycle of HD-MTX, with the symptoms reappearing 10 days after, with left central facial paraesthesia, followed by a paraesthesia of the right limbs, dysarthria and dysphagia. A cranial-cephalic MRI identify a new lesion on the right corona radiata. Following the results, it was assumed by different specialties - pediatrics, neurology and neuroradiology - that we were dealing with a case of sub-acute neurotoxicity.
The hypothesis is supported by the fact that the imaging findings are fundamental in case of pseudo-stroke for its particular characteristics: The early alterations of the diffusion restriction of the white substance normalize within one week which agrees with the described case [3]. Moreover, it's important to say that the cranial-cephalic MRI with broadcast sequences is fundamental to establish the differential diagnosis in immuno-suppressed patients: CNS infections (abscess, meningo-encephalitis), hemorrhagic cerebral vascular accident or ischemic CVA (increased by the usage of asparaginase-chemotherapy) or reversible posterior encephalopathy syndrome (PRES syndrome) - associated to areas of vasogenic edema.
Despite having always verified a complete resolution of the neurological deficits, their presentation was alarming. This way it has been necessary to review the therapeutic plan, but without neglecting the essential document of MTX in treatment, knowing that his suspension could lead to an incomplete reversible complication, as well as the relapse of the disease [1].
In the presented case it has been chosen to gradually reintroduce the drug and to associate it to the dextromethorphan, finding the patient still on treatment at the moment of writing and clinically well. Meanwhile, it has been considered a possible increase of the teenager sensibility to this drug, since with bigger intervals between administrations, clinical or imaging alterations haven't been recorded.
- Neurotoxicity is a known complication associated with HDMTX administration in the treatment of children with lymphoma;
- Effects associated with increased MTX levels are: Excitatory effects on NMDAR and increased oxidative stress, which can lead to regional and local neuronal death and small vessel vasculopathy;
- Neurotoxicity may be acute, sub-acute or chronic;
- It is important to diagnose, identify and use the appropriate antidote;
- Symptoms may be treated previously by administration of dextromethorphan.
None.