Paracetamol overdose is an important cause of drug toxicity and pediatric overdose emergencies remain a significant global issue. Paracetamol is a known toxin to several tissues, but extrahepatic manifestations are not so well established as hepatotoxicity. Acute kidney injury occurs in up to 2% of paracetamol overdoses, generally coexisting with hepatotoxicity.
A 14-year-old female adolescent presented to the emergency department 24 hours after a purposeful overdose of 22.5 grams of paracetamol taken with suicidal intent. Three hours after pills ingestion, she started with vomiting and abdominal pain. Renal function started to deteriorate on day 3, at the peak of liver injury, with oliguria refractory to diuretic therapy and nephrotic proteinuria. Corticosteroid therapy and hemodialysis were initiated with a favorable clinical recovery.
This case highlights that paracetamol overdose nephrotoxicity may be an important cause of concern and future research should focus on better understanding this phenomenon and preventing additional kidney damage.
Acetaminophen, Acute kidney injury, Acute tubular necrosis, Hepatotoxicity, Nephrotoxicity, Paracetamol
AKI: Acute Kidney Injury; HD: Hemodialysis; INR: International Normalized Ratio; NAC: N-acetylcysteine; NAPQI: N-acetyl-p-benzoquinoneimine
Since its clinical introduction in 1950, paracetamol (also known as N-acetyl-p-aminophenol or acetaminophen) has become the most used analgesic and antipyretic worldwide [1-3]. Although it is remarkably safe when used at therapeutic doses, pediatric overdose emergencies still remain a significant global issue [1,2]. Paracetamol is the drug most commonly used in teenager deliberate overdoses, particularly in their first attempts [4].
Paracetamol overdose is simultaneously a frequent cause of drug toxicity and a common presentation to the emergency department [5,6]. It is considered the leading cause of acute liver failure and can be life threatening [5,6]. The incidence of this poisoning and the severity of its outcomes are quite variable throughout the world [7].
In what concerns clinical presentation, early nonspecific symptoms may include nausea, vomiting, abdominal pain and malaise [8]. Even though this symptomatology may improve over the first 24 hours, progressive hepatic injury may manifest as early as day 3 with right upper quadrant pain and tenderness [8].
Paracetamol is a known toxin to both the liver and extrahepatic tissues [3,9,10]. Repeated supratherapeutic ingestion as well as acute overdose may be deleterious and while the induced liver necrosis has already been extensively studied, extrahepatic manifestations are currently not so well described in the literature [8,9,11]. Acute kidney injury (AKI) occurs in up to 2% of patients with paracetamol overdose and it is generally seen in association with hepatotoxicity, being a rare entity when isolated [3,9]. In most cases, AKI becomes evident after hepatotoxicity and may complicate fulminant hepatic failure [8].
Oral ingestion results in a peak concentration one or more hours after ingestion and with normal hepatic clearance, around 90% of paracetamol will suffer conjugation to a nontoxic product and be excreted in urine [5,6]. The remainder will be metabolized by the hepatic cytochrome P450 to the toxic intermediate N-acetyl-p-benzoquinoneimine (NAPQI) [6]. Therefore, the major pathophysiology of large dose paracetamol-related systemic toxicity results from the balance between NAPQI and baseline glutathione levels in the whole body [6]. N-acetylcysteine (NAC) given for up to 72 hours reliably replete glutathione and prevents injury, being most effective when begun within 10 hours after ingestion [1-7]. In what concerns paracetamol-induced renal failure, the role of NAC therapy still remains unclear [8].
Paracetamol is a small water-soluble molecule with a low volume of distribution which is effectively filtered by hemodialysis (HD) [9]. Although HD is not a well-recognized treatment option for paracetamol overdose, in the rare instance of AKI, it may have its role [9,12].
We aim to emphasize the potential clinical relevance of nephrotoxicity following paracetamol-induced severe hepatic damage, as well as the likely important contribute of hemodialysis as rescue therapy.
A 14-year-old female adolescent presented to the emergency department with vomiting and abdominal pain for 21 hours. She had taken a purposeful overdose of 22.5 grams of paracetamol 24 hours ago, with suicidal intent. She had no past medical history of note, no known allergies and took no regular medications.
Her physical examination revealed a body temperature of 36.8 °C, a pulse rate of 122 per minute and blood pressure of 117/66 mmHg. Furthermore, it stood out a mild jaundice and her abdomen was more painful on palpation of the right hypochondrium. She was neurologically and hemodynamically stable and there were no other major findings during observation.
From her initial blood tests (Figure 1), it is to highlight the derangement of liver function, with important elevation of aminotransferases and the already affected hepatic synthetic function, with prolonged international normalized ratio (INR) and elevation of D-dimers. Her blood gas showed mild compensated metabolic acidosis with a pH of 7.41, base excess of -5.6 mmol/L, bicarbonate of 20.6 mmol/L and lactate of 4.1 mmol/L. Electrolytes and renal function were within normal values. Paracetamol dosing was of 0.048 ug/mL (< 4 ug/mL) and urinary drug research was negative [1].
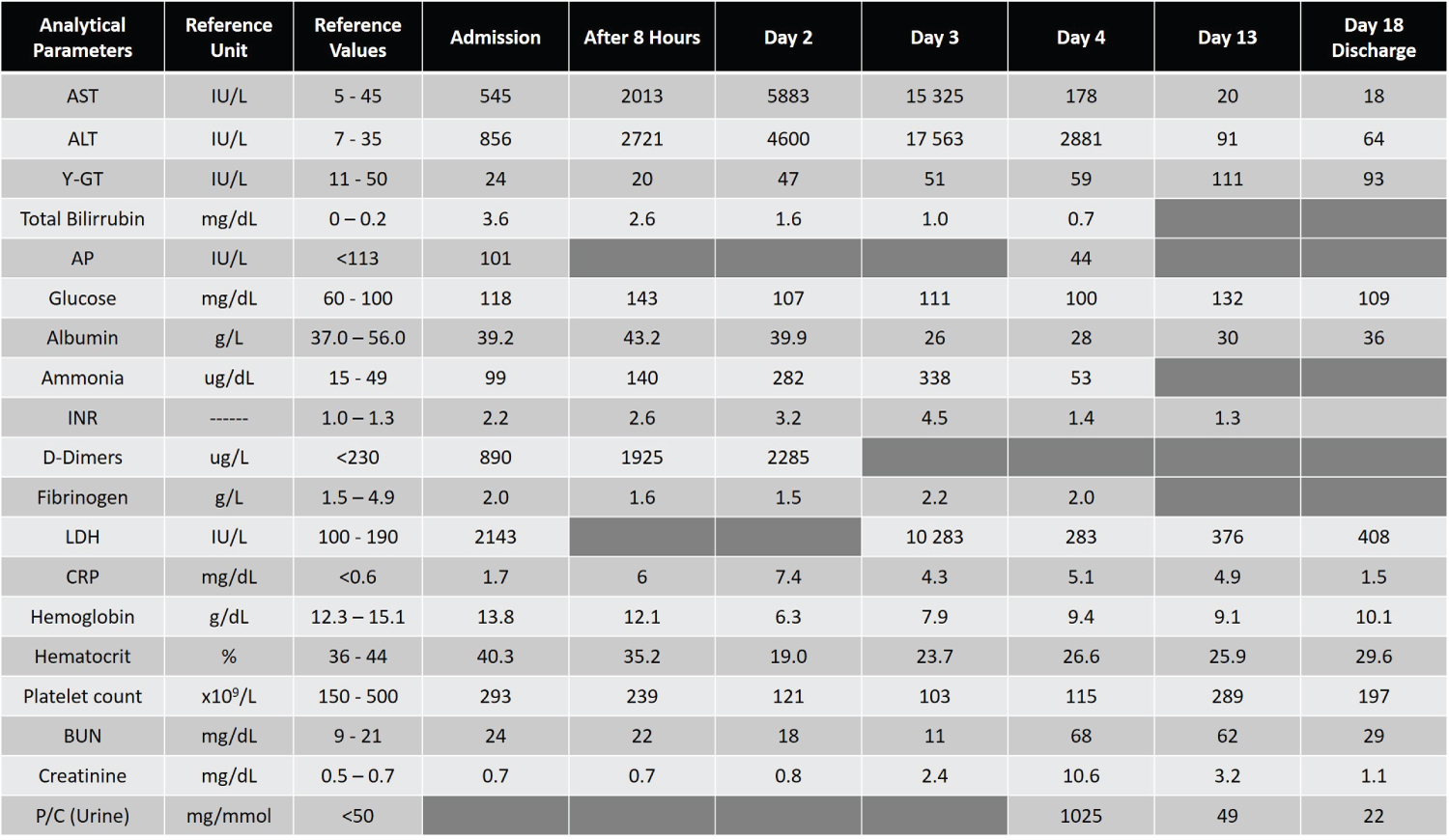 Figure 1: Analytical investigation from admission to discharge (day 18).
Figure 1: Analytical investigation from admission to discharge (day 18).
ALT: Alanine Transaminase; AST: Aspartate Transaminase Transpeptidase; AP: Alkaline Phosphatase; BUN: Blood Urea Nitrogen; CRP: C-Reactive Protein; Ƴ-GT: Ƴ-Glutamil; INR: International Normalized Ratio; LDH: Lactic Dehydrogenase; P/C: Protein Creatinine Ratio
View Figure 1
She initiated N-acetylcysteine and vitamin K as treatment. For the progressive hyperammonemia disproportionate to the degree of coagulopathy, empirical antibiotic therapy, sodium benzoate and phenyl butyrate were associated later. The electroencephalogram performed had no alterations.
On day 2 of hospitalization, full blood count revealed a drop in hemoglobin to 6.3 g/dL and transfusion was required. Aspartate and alanine transaminases posteriorly rose to 15 325 U/L and 17 563 U/L, respectively, on day 3, and then gradually fell. Despite liver recovery, renal function started to deteriorate from the third day onwards, with oliguria refractory to diuretic therapy and nephrotic proteinuria (urinary protein/creatinine ratio 1025 mg/mmol) by day 4, with plasma creatinine of 68 mg/dL and blood urea nitrogen of 10.6 mg/dL. Furthermore, urine analysis revealed glycosuria 50 mg/dL, leukocyturia 75 cells per microliter and absence of nitrite. On microscopic examination, there were countless erythrocytes, 15 leukocytes per high power field and no granular casts.
Given the history of massive overdose and the emerging AKI, she started corticosteroid therapy and a trial of hemodialysis (HD) was initiated on the Intensive Care Unit (96 hours after ingestion).
Renal biopsy revealed important acute tubular necrosis with foci of tubulointerstitial nephritis and mild mesangial proliferation.
In the following days, the patient's renal function progressively improved and it was possible to discontinue HD by day 13, after 9 sessions performed.
By the time of discharge (day 18), all the monitored analytical parameters were frankly improved. Therefore, the patient completed a month of corticosteroid therapy on an outpatient basis and follow-up in nephrology and child psychiatry consultations was granted.
Paracetamol is an immediate-release antipyretic and analgesic medication with a maximum recommended therapeutic daily dose of 4 grams for adults [6]. It is not only a commonly overdosed drug but also the main cause of acute liver failure in the developed world and its toxicity is closely linked to its metabolism [6,11,12].
Paracetamol is predominantly metabolized by conjugation with sulfate and glucuronide. Up to 10% of the drug is oxidized by CYP450-dependent pathways (mainly CYP2E1 and CYP3A4) to NAPQI, which will be posteriorly detoxified by glutathione and eliminated into urine or bile. The NAPQI that is not detoxified may bind to hepatocytes and produce cellular necrosis [11].
NAC is considered the mainstay of treatment as it dramatically reduces the incidence of hepatotoxicity and progression to hepatic failure when administered within the first ten hours following an acute overdose [8,10]. In patients who receive NAC within the first 8 hours, the risk of hepatotoxicity is less than 5% whereas delays beyond 10 hours are associated with an increased risk of hepatic injury [8]. Therefore, NAC has a clear role in preventing paracetamol-induced liver necrosis. Nevertheless, it seems not to have a similar benefit in preventing nephropathy, but at least seems not to be harmful for the kidney [9]. This further reinforces the concept that discrete mechanisms of toxicity exist between the liver and the kidney [9].
NAC supplements endogenous glutathione stores and promotes conjugation of NAPQI to a non-toxic metabolite [10]. However, with very large paracetamol ingestions, sometimes the supplementation of a standard dose of NAC is inadequate to restore prevailing mitochondrial dysfunction translated, in this clinical case, by a deranged metabolic status [10]. This is because NAC reacts in a 1:1 ratio with NAPQI and, with larger doses; there is more NAPQI than there is NAC [10]. In such contexts, acute liver injury and death can quickly ensue [10].
Paracetamol intoxication typically includes 4 phases [13]. The first consists of anorexia, nausea, vomiting and malaise [13]. The second phase is generally characterized by right upper quadrant pain or tenderness, liver enlargement and oliguria in some patients [13]. Bilirubin and hepatic enzyme levels become elevated and the prothrombin time gets prolonged [13]. In the third stage, usually 3 to 5 days into the course, some of the initial symptomatology may reappear along with signs of hepatic failure, including jaundice, hypoglycemia, coagulopathy and encephalopathy. Renal failure and cardiomyopathy may also turn up [13]. The fourth phase is associated with recovery or progression to death from complete liver failure [13]. However, deaths among adolescents are rare and the majority of paracetamol overdose deaths seem to occur in older adults (less than 2%) [3].
Compared to adults, pediatric patients seem to have better outcomes and be less willing to develop acute liver failure, mainly because of their large hepatic cell masses capable of adequately metabolizing paracetamol in a nontoxic manner [2]. Furthermore, younger individuals seem to better compensate for acute hepatic dysfunction through a higher capacity for extrahepatic metabolism of toxic substances like ammonia, which may be substantially metabolized by striated muscle tissue [4]. Even though some authors suggest that the risk of developing acute liver injury is proportionate to paracetamol levels at presentation, for others predicting outcomes and prognosis remains a challenge [12].
This clinical case portrays a teenager who performed an intentional overdose of 22.5 grams of paracetamol and only resorted to health care 24 hours after the ingestion, when she was already quite symptomatic with vomiting and abdominal pain. NAC is believed to be most effective when given within the first 10 hours after overdose, but may still be of benefit in patients who present more than 24 hours later. Therefore, while paracetamol dosing is pending, empirical treatment with NAC should be provided and consultation with a regional poison control center or medical toxicologist is strongly advised [1].
On the other hand, patients who present more than 24 hours after an acute ingestion may not have detectable serum paracetamol concentrations but still manifest symptoms like nausea, vomiting, abdominal pain, renal injury, coagulopathy, hepatic encephalopathy, cerebral edema or hypotension [1]. In this particular case, subtle jaundice, vomiting and right upper quadrant abdominal pain was clinical signs of hepatic injury.
There are several factors associated with hepatotoxicity in pediatric age, such as delay in the onset of symptoms, unintentional multiple overdosing, ingestion of paracetamol along with other hepatotoxic drugs and use of adult rather than pediatric preparations [13]. In this particular case, the main determining factor was delay in initiation of NAC treatment [13].
In what concerns liver enzymes, they typically start increasing within 24 to 36 hours after an overdose and maximal liver injury typically peaks between three to five days with jaundice, coagulopathy or even encephalopathy [8]. Either recovery or progression to hepatic failure will occur over the following several days [8]. In this clinical case, maximal liver injury was documented on day 3 associated with coagulopathy and both improved considerably from then on. Although less common, AKI with oligoanuria refractory to diuretic therapy also emerged by day 3, at the peak liver injury [8]. The relationship between dose and nephrotoxicity is not as clearly delineated as for paracetamol-induced hepatotoxicity and nephropathy may occur at lower doses than those seen with hepatotoxicity [9]. Maximal renal injury is known to lag beyond peak liver injury and recovery is also more protracted, what could be verified in this clinical case [8]. Nephrotoxicity without hepatotoxicity is rarely seen and generally reversible [3].
Relatively to INR, it is known that early increments seen at 12 to 16 hours after an overdose seem to be the result of paracetamol interference in the production of active factor VII and, as a result, may not reflect hepatocellular injury [8]. This effect is usually modest and NAC has also been implicated as a cause of an early increase in the INR [8]. However, in our patient, INR gradually increased until the third day, with frank elevation of D-dimers, what is far more suggestive of coagulopathy, given the clinical setting.
Paracetamol, as a small, water-soluble molecule with a relatively low volume of distribution, is at least a moderately dialyzable compound [12]. However, given the efficacy of NAC in most cases, the use of HD in overdose has been confined to a supportive role as renal replacement therapy in the setting of multiorgan failure or cases where NAC therapy is not sufficient [12]. Therefore, this clinical case constitutes an example of HD as a successful and effective means of correcting the acidosis and removing the paracetamol.
With regard to renal biopsy, it is rarely performed for diagnostic purposes in the setting of paracetamol-induced nephropathy and histopathology usually reflects an acute tubular necrosis-type pattern [9]. At the tissue level, paracetamol toxins most commonly affect the proximal tubule, although the disease may be more diffuse [9]. In this particular case, given the clinical exuberance, renal biopsy was performed to help, in a complementary way with urinalysis, in the differential diagnosis with other important causes of AKI, such as hepatorenal syndrome or prerenal azotemia [9].
To sum up, although detailed pathophysiological mechanism between paracetamol intoxication and AKI may still need further clarification, it is important that physicians remember nephrotoxicity associated with hepatic damage [6]. It also should be kept in mind that despite being rare, nephrotoxicity may occur even without hepatotoxicity and these patients should be monitored for nephrotoxicity [6].
In case of paracetamol poisoning, a thorough history and physical examination with identification of risk factors, NAC therapy based on the potential for hepatotoxicity, supportive care, as well as serial monitoring of urine output, blood pressure and markers of glomerular function are essential to treatment [9].
Future research should aim not only to better understand and manage this phenomenon, but also to develop strategies in order to assist physicians in preventing additional nephrotoxicity [6,9]. The maintenance of hemodynamic stability and adjusting drug doses are two of the fundamental aspects, but there is always room for improvement [1,6,9].
There were no external funding sources for the realization of this paper.
All authors contributed significantly to the elaboration of this manuscript.