A bronchopleural fistula (BPF) is a pathologic communication between a bronchus and the pleural space. BPF has a high morbidity and mortality, therefore a timely diagnosis is of great importance. Methylene Blue has been used for the localization of BPF for decades and although other diagnostic tools are available, it remains favorable because it is widely available, safe and easy to perform. In this case report we would like to stress the ongoing relevance of this diagnostic method by presenting 2 cases in which instillation of Methylene Blue was used in current practice to localize BPF.
Bronchopleural fistula, Post-operative, Empyema, Complication, Interventional pulmonology, Bronchoscopy, Methylene blue, Diagnostic
BPF: Bronchopleural Fistula; COPD: Chronic Obstructive Pulmonary Disease; CT: Computed Tomography Scan; PET: Positron Emission Tomography; FDG: Fluoro-Deoxyglucose; DLCO: Diffusion Capacity; VATS: Video Assisted Thoracic Surgery
A bronchopleural fistula is a pathologic communication between a bronchus and the pleural space. BPF can originate at every level of the bronchial tree (major, lobar, or segmental bronchus) and differs from an alveolopleural fistula as there is no connection between the pleural space and the lung parenchyma. BPF is a rare but feared complication after thoracic surgery, mostly pneumonectomy and lobectomy, due to its high morbidity and mortality [1]. Prevalence is estimated between 0.5% and 4% with a substantial greater risk in post-pneumonectomy patients compared to patients who underwent lobectomy or sublobar resection [2]. Comorbidities like diabetes, chronic obstructive pulmonary disease (COPD), malnutrition, older age and previous chemo-and/or radiation therapy as well as perioperative factors including a right sided approach and remaining tumor at the bronchial margin are predisposing factors for the development of BPF [3]. Other nonsurgical etiologies like malignant, infectious and inflammatory disease invading into the pleural space have been described but are even more uncommon. Although well established, BPF remains a challenging diagnosis and difficult to treat complication of thoracic surgery and the pulmonologist is often involved in the process [1]. Diagnostic methods for the localization of BPF include bronchoscopy to detect proximal mucosal defects, Methylene Blue instillation, sequential balloon occlusion of the bronchi for more distal defects and bronchography with ventilation scintigraphy [4]. While the latter has more and more been abandoned, the use of Methylene Blue during bronchoscopy is still a very useful, safe and cheap tool. Since pleural puncture is a routine intervention in the pulmonary practice, no extra expertise is necessary for the visualization of BPF. In this case report we would like to stress the ongoing relevance of this diagnostic method by presenting 2 cases in which Methylene Blue was used in current practice to localize BPF.
A 63-year-old male with COPD and a history of stage IB squamous cell lung carcinoma underwent induction chemoradiotherapy followed by a bilobectomy of the right lower and middle lobe. 4 weeks post-surgery he presented at the emergency department with acute fever, malaise and a worsening productive cough since 10 days. At evaluation he had a dull percussion of the right lower lobe and fine crackles were heard over the right hemithorax. Blood tests showed elevated inflammatory markers (C-reactive protein, erythrocyte sedimentation ratio and leukocytosis), a neutrophilic predominance and slightly elevated lactic acid. A chest radiograph showed pleural fluid filling the post-lobectomy space and a consolidation in the adjacent lung parenchyma. Blood cultures were drawn and broad spectrum antibiotics were promptly started at the emergency department. A computed tomography (CT) scan of the chest during the first day of hospitalization revealed an air-fluid level and air within the pleural fluid in the post-lobectomy space apart from the known consolidation in the right upper lobe. A complicated pleural effusion was suspected and the same day a pleural puncture was ordered. Evacuation of the pleural fluid showed brown, stinky pus which led to the diagnosis of an empyema. Because air was noted in the pleural fluid and the patient had a history of semi recent surgery there was a suspicion for BPF. A bronchoscopy was planned for the evaluation of a bronchial defect using Methylene Blue. First off, a new pleural puncture was performed, using a 28 millimeter Boutin needle. We diluted 1 milliliter (10 mg/ml) of Methylene Blue in 60 milliliters of normal saline and slowly injected this into the pleural cavity through a small catheter using a three-way-valve (Figure 1a). We waited a few minutes before initiating bronchoscopy to give the dye some time to mobilize. However the patient started coughing in between procedures and a clear blue phlegm was collected, making the diagnosis of BPF very likely (Figure 1b). Bronchoscopy revealed a dehiscence of 2 centimeters of the post-operative bronchial stump at the level of the intermediate bronchus with Methylene Blue coming out of the center of the dehiscence (Figure 1c and Figure 1d).
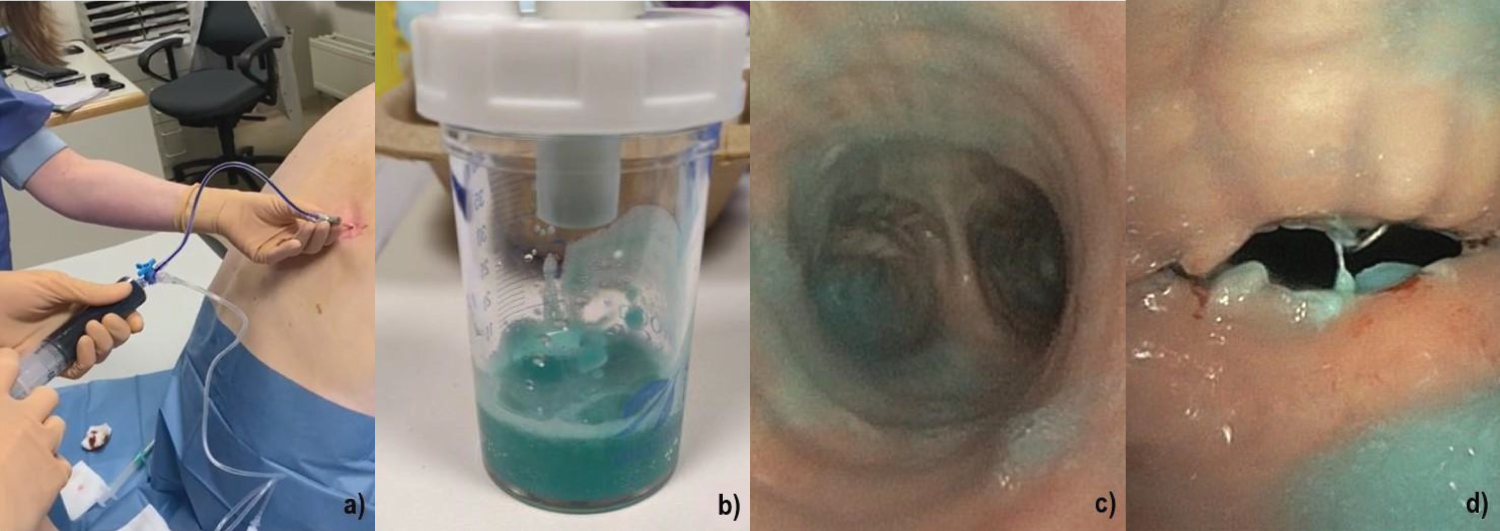 Figure 1: a) Instillation of a Methylene Blue dilution using a three-way-valve and a Janet syringe; b) Sputum after administration of Methylene Blue; c) Tracheal view of a blue phlegm in the right intermediate bronchus; d) Close-up image of stump dehiscence showing Methylene Blue leakage. View Figure 1
Figure 1: a) Instillation of a Methylene Blue dilution using a three-way-valve and a Janet syringe; b) Sputum after administration of Methylene Blue; c) Tracheal view of a blue phlegm in the right intermediate bronchus; d) Close-up image of stump dehiscence showing Methylene Blue leakage. View Figure 1
Investigation of all other bronchi was normal. The patient was then referred to a university hospital and scheduled for a surgical revision of the stump using vascularized flap tissue.
A 66-years-old male was seen at the outpatient clinic for a routine oncologic follow-up. He had a history of lung emphysema and a lobectomy of the left lower lobe for a large cell neuro-endocrine carcinoma followed by chemoradiotherapy almost 14 years ago. On positron emission tomography (PET) CT scan, a fluoro-deoxyglucose (FDG) avid focus was noticed in the lobectomy space. Also a new FDG-avid nodule emerged in the right upper lobe but it was not suited for resection due to insufficient respiratory reserve as lung function testing showed a diffusion capacity (DLCO) of 37%. As there was suspicion of a locoregional relapse, a video assisted thoracic surgery (VATS) was planned. Exploration of the lobectomy space showed a hard fibrinous tissue but no suspect lesion. The parietal pleura however had a rather sick appearance so pleural biopsies were taken and afterwards a talc pleurodesis was conducted. Histology results of the biopsies and tissue in the lobectomy space were negative for malignant cells and showed chronic inflammation and anthracosis pigments. Air leak in the chest drainage system persisted 3 weeks after the VATS procedure. The chest drainage system was thoroughly checked for air leaks but was airtight. CT scan of the chest showed air bubbles in the lobectomy space. To exclude the possibility of a late bronchopulmonary fistula, we performed a bronchoscopic evaluation of the lobectomy stump of the left lower lobe with instillation of Methylene Blue through the chest drain. A 50 milliliter Janet syringe was used to dilute 1 milliliter (10 mg/ml) of Methylene Blue in 50 milliliters of normal saline. The chest drain was clamped, disconnected from the collection system, connected to the Janet syringe and unclamped, after which the Methylene Blue could be injected into the chest tube and pleural cavity (Figure 2a). Bronchoscopy after 5 minutes of waiting, showed a normal inspection of both right and left bronchi and there were no blue markings observed. The post-lobectomy stump had a normal appearance (Figure 2b). This investigation could exclude the differential diagnosis of BPF.
 Figure 2: a) Injection of Methylene Blue into chest drain; b) Normal post-lobectomy stump. View Figure 2
Figure 2: a) Injection of Methylene Blue into chest drain; b) Normal post-lobectomy stump. View Figure 2
The patient in the first case was transferred to a university hospital immediately after diagnosis and was scheduled for an urgent surgery the day after. Unfortunately he rapidly progressed into a septic shock for which he was intubated and transferred to the intensive care unit prior to surgery. Surgical cleaning of the empyema and revision of the bronchial stump using a vascularized muscle flap followed two days later and went uncomplicated. The patient is in good health status and working on his revalidation 4 weeks post-operative. The second patient has been further evaluated for causes of persistent air leak. A pleural deficit (alveolopleural fistula) secondary to pleural biopsies during surgery was considered the most plausible etiology. A conservative treatment with a Heimlich valve was started. After 6 weeks he was doing fine and a chest radiograph showed no residual pneumothorax so the Heimlich valve could be removed.
BPF is associated with significant morbidity and mortality, therefore a timely diagnosis is of great importance. Risk factors are well identified and clinical suspicion should be raised in post-surgery patients with prolonged air leaking in the chest drainage system. In our cases, both patients had underlying lung disease and a history of prior chemo and/or radiotherapy making them at risk for BPF. Furthermore the patient in case 1 underwent a right sided lobectomy, which is thought to have greater risk for BPF due to a diminished blood supply to the bronchial stump.
Multiple diagnostic entities have been used throughout time but diagnosis of BPF often remains challenging and guidelines on this subject are lacking. In common practice balloon occlusion during bronchoscopy is time consuming and bronchography with labeled gasses like 133Xe, 81mKr, and 99mTc diethylenetriaminepentaacetic acid ventilation scintigraphy have been left behind. Medical imaging, mostly CT scans, can be very useful to provide additional information of the lobectomy space and its surrounding structures but is not very performant at visualizing or localizing BPF. The use of Methylene Blue for the evaluation of BPF was first described in 1972, although the organic chloride was already known as a treatment for methemoglobinemia, malaria and vasoplegia [4]. It is widely available, inexpensive and fairly easy to use in a broad range of surgical and nonsurgical procedures which makes it an indispensable product in most hospitals. At a concentration of 10 mg/ml, Methylene Blue can be diluted a 50-250 fold in saline to receive a solution that maintains its blue vivid color and is practical to use for injections.
Serotonin syndrome is described at doses above 2 mg/kg but is very rare, especially when using diluted solutions. A side effect of the dye is discoloration of skin and tissue which in some cases can hinder in surgical procedures afterwards and therefore should be taken into account.
With this case report we would like to stress the ongoing relevance of Methylene Blue instillation as a safe, easy to perform and effective technique for the localization of BPF.
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
The authors declare an equal contribution to this manuscript.