Pleural Effusion is a common medical problem with more than 50 recognized causes including disease local to the pleura or underlying lung, systemic conditions, organ dysfunction, and drugs. The majority of malignant PEf is caused by metastatic disease: Most commonly lung cancer in men and breast cancer in women. However, few germinal teratomas have been reported as the main cause of unilateral PEf.
A 17-year-old female patient was admitted to the emergency department presenting a chronic non-productive cough with a six-week progression, non cyanotizing; progressive dyspnea to small or medium efforts, and intermittent chest pain in left-hemitorax witch increase at forced respiratory movements.; pulmonary fields with a decreased vesicular murmur, vocal vibrations; respiratory movements in left hemithorax. Chest radiographic image showed 95% left pleural effusion. Community-acquired pneumonia and massive pleural effusion were established as the initial diagnosis. After 24-h evolution was taken, a simple chest computerized tomography (CT) scan, that shows a left pleural effusion and a structure in the right pulmonary apex with heterogeneous densities, focal calcifications and a displacement of the mediastinal structures towards right hemitorax. Afterwards, a biopsy guided by computerized tomography was performed; histologic diagnosis was established and, classified as a mature and benign teratoma. Subsequently, after 1-month; a complete resection of the tumor was performed successfully without complication.
Benign germinal teratoma is a frequent tumor in the mediastinum and rarely in adjacent organs. However, as in this case it is possible to find it as the cause of a unilateral pleural effusion. Clinical diagnosis should be suspected when there is no apparent clinical pathology to explain unilateral pleural effusion. Normally a CT scan establishes the initial diagnosis and confirmed by biopsy and histopathological studies for it to be removed later.
Pleural effusion, Germinal tumourm, Germinal teratoma
PEf: Pleural Effusion; mmHg: Millimeter of Mercury; CT: Computerized Tomography; CA15-3: Blood Test Usually Used for Breast Cancer Diagnosis; CA19-9: Blood Test Usually Used for Pancreatic Cancer Diagnosis; CA125: Blood Test Usually Used for Ovarian Cancer Diagnosis; BGT: Benign Germinal Teratoma
Pleural effusion (PEf) is the result of fluid accumulation in the pleural space which indicates the presence of pulmonary, pleural or extrapulmonary disease [1]. PEf is a common medical problem with more than 50 recognised causes including disease local to the pleura or underlying lung, systemic conditions, organ dysfunction and drugs [2], as well as, different tumours [3]. The majority of malignant PEf is caused by metastatic disease: most commonly lung cancer in men and breast cancer in women [4]. Other causes of unilateral PEf reported have been manifestations of severe ovarian hyperstimulation, [5,6], acutelymphoblastic leukaemia [7], and a rare presentation of multiple myeloma [8]. However, few germinal teratoma had been reported as a main cause of unilateral PEf without ovarium stimulation as a principal cause. Teratomas are congenital germ cell tumours derived from the three germinal layers. They are classified into mature or immature teratomas according to the degree of cell differentiation. Mature or well-differentiated teratoma tends to act benignly [9]. This report describes the diagnosis and management of a rare case of unilateral pleural effusion, secondary to germinal teratoma in the left pulmonary apex.
Previously to present this case report a written informed consent was obtained from the patient's legal guardian(s) for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
A 17-year-old female patient was admitted to the emergency department. She had a chronic non-productive cough with six-week of evolution with night-time predominance accesses non cyanotizing; progressive dyspnoea to small or medium efforts, intermittent chest pain in left-hemitorax with increase at forced respiratory movements. 12-hours previous to admission she presented fever with 38.2 grade Celsius and diaphoresis. During physic exploration, she presented 15-points Glasgow; arterial tension: 110/70 mmHg; hearth rates: 130 beats per minute; respiratory rate: 27 breaths per minute; oxygen saturation an environment: 86%; integument; pulmonary fields with a decreased vesicular murmur, vocal vibrations; respiratory movements in left hemithorax, rhythmic and tachycardic precordium without murmurs and an asymptomatic abdomen. Chest radiographic image showed 95% left pleural effusion (Figure 1). Laboratory parameters were following: leucocytes 21.1 × 103/mm3, with 80% mature neutrophils, and 4% immature neutrophils; total proteins (TP), 6.3 g/dL; Albumin, 3.0 g/dL Lactic dehydrogenase (LDH), 474 U/L; other biochemical parameters as glucose, creatinine, sodium, potassium, and hepatic enzymes within normal parameters. Community-acquired pneumonia and massive pleural effusion are established as initial diagnosis in the emergency department and empiric treatment with Hartman parenteral solution including ceftriaxone 1 g/24-h and clarithromycin 500 mg/24-h is initiated. After 24 hours a simple chest CT scan showed a left PEf and a strucure in the left pulmonary apex with heterogeneous densities, focal calcifications and a displacement of the mediastinal structures towards right hemitorax (Figure 2).
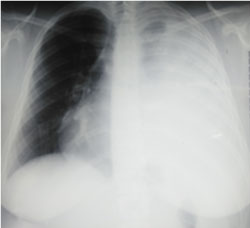 Figure 1: Chest radiography with left massive and unilateral pleural effuse. View Figure 1
Figure 1: Chest radiography with left massive and unilateral pleural effuse. View Figure 1
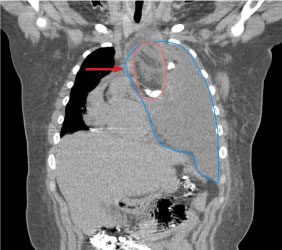 Figure 2: Thoracic tomography showed an atypical mass in the left pulmonary apex, with heterogeneous density (solid, liquid, fat, soft tissues, and calcifications suggestive of dental pieces and/or bone fragments). View Figure 2
Figure 2: Thoracic tomography showed an atypical mass in the left pulmonary apex, with heterogeneous density (solid, liquid, fat, soft tissues, and calcifications suggestive of dental pieces and/or bone fragments). View Figure 2
Tumour markers were investigated (α-fetoprotein, carcinoembryonic antigen, CA15-3, CA19-9, CA125) with values within normal parameters. To the 5th day of the hospital staying has performed a therapeutic and diagnosis thoracentesis (1300 mL/24 h); histochemical analysis of pleural liquid reported: pH 8.0; leucocytes, 379/mm3; LDH, 11,075 U/L; TP, 4.2 g/dL; Albumin, 2.0 g/dL; cholesterol, 65 mg/dL (characteristic parameters for an exudate); posteriorly, microbiological cultures and BAAR stain were reported negatives. At this time, the diagnosis of mediastinal tumour due to probable germinal teratoma is integrated. Afterwards, a biopsy guided by CT was performed, and anatomopathological diagnosis was classifying as mature and benign teratoma (histological imagen unavailable). Subsequently, after 1-month; a complete resection of the tumour was performed successfully (Figure 3) without complication in a third level hospital. One month after the surgery, One month after the surgery, a chest CT control was taken and showed a thorax without tumour or pleural effusion and a normal pulmonary expansion (Figure 4). Currently, the patient has been free of disease and living a normal daily life after one-year evolution.
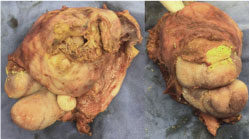 Figure 3: Tumour removed from the left pulmonary apex showing different tissues, (soft tissue, fat, a tooth and fragment of 2 fingers and nails). View Figure 3
Figure 3: Tumour removed from the left pulmonary apex showing different tissues, (soft tissue, fat, a tooth and fragment of 2 fingers and nails). View Figure 3
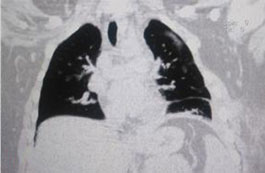 Figure 4: Thoracic tomography without tumour, pleural effuse, total pulmonary expansion and some sites with fibrosis; consequence of the previous surgical procedure. View Figure 4
Figure 4: Thoracic tomography without tumour, pleural effuse, total pulmonary expansion and some sites with fibrosis; consequence of the previous surgical procedure. View Figure 4
The etiology of PEf may be pleural, pulmonary or extrapulmonary. The differential diagnosis for PEf is extensive, however benign germinal teratoma is not mentioned as a common cause [10]. Signs and symptoms may be specific to the respiratory system or nonspecific. Dyspnea is a major, although nonspecific, respiratory symptom which accompanies PEf, commonly with progressive worsening [11]. The patient was initially management with antibiotics due to the principal cause of pleural effusion is an infectious process, as demonstrated by Amit Kumar, et al. [12] who reported that the most common cause of the unilateral pleural effusion, tuberculosis followed by pneumonia. PEf can be transudative or exudative. In cases of transudative PEf, the diagnosis is usually made without much difficulties but exudative pleural effusion requires careful workup [13]. Differential diagnosis that includes parapneumonic effusion, tuberculosis and metastatic cancers which are found to be the cases in a great number of patients. In the present case, the cytological and biochemical parameters in addition negative microbiological results of the pleural fluid were indicatives of an exudate and further workup was continued to determine the possible cause. Primary tumors of the pleura relatively rare the most common being malignant pleural mesothelioma, pleuro-pulmonary blastoma (representing a malingant epithelial neoplams) and solitary fibrous tumor (a mesenchymal tumor). Other primary pleural tumors, like well-differentiated papillary mesothelioma, synovial sarcoma, angiosarcoma, epithelioid hemangioendothelioma and adenomatoid tumor are extremely rare [3] with a median overall survival for the epithelioid type of 16 months, a 2-year overall survival of 34% and a 5-year overall survival of 11% [14]. However, the diagnosis of a malignancy is not feasible due to age of presentation and epidemiological characteristics of the disease itself in our patient as well as the clinical evolution, imagen and histologic characteristics of this case. Patient was diagnosed as a benign germinal teratoma (BGT) and was surgically resected.
BGT can be found in other organs and may involve in descending order: the ovaries, testicles, sacrococcygeal region, mesiastinum, and other sites [15]. Intrapulmonary teratoma originates from one, or more, of the three germinative layers of the totipotential cells of which can differentiate into any type of tissue [15]. Extra-gonadal germ cell tumors represent 2-5% of all germ cell tumor [16] with an incidence around 1/1,000,000 population [17]. BGC occur in adults as well as children, with the age ranging from 10 months to 68 years and the majority of patients are diagnosed in the first two decades of life. Patients with intrapulmonary BGT present also chest pain (52%), haemoptysis (42%) and cough (39%) [9]. Same presentation occurs in our case except by hemoptysis, but presenting dyspnea to small or medium efforts. Radiologically, lesions are typically cystic, often with focal calcification. CT imaging can estimate the density of diverse elements, such as soft tissues (in most of the cases), fluid (88%), fat (76%), calcification (53%) and teeth [18,19]. similar characteristics have been presented in this case and showed in Figure 3. Surgical resection is the standard treatment because mature teratomas are usually well encapsulated [16,20]. In addition, complete surgical resection of BGT is normally curative. However, survival and resectability can be limited by the size of the tumor, its invasion of adjacent structures, and desmoplasia. Recurrence is rare and generally is associate to incomplete resection of tumor [20].
Benign germinal teratoma is a frequent tumour in the mediastinum and rarely in adjacent organs. However, as in this case, it is possible to find it as the cause of a unilateral pleural effusion. Clinical diagnosis should be suspected when there is no obvious clinical pathology to explain it. Initial diagnosis is confirmed by a CT scan and confirmed by biopsy and histopathological studies for it to be later removed.
The authors, patient and her family are pleased to acknowledge the efficient and professional work the thoracic surgery, radiology, pathologist and ER medical staff of Hospital Santiago Ramón y Cajal of ISSSTE in management and resolved this case.
This case report was not founded.
Full digital images and electronic medical records are available by the Editor-in-Chief of this journal.
All authors have read and approved the final manuscript. MRRG (Emergency Physician) Involved in the initial diagnosis and treatment of the patient. IALG (Medicine pre-grade student): Medical student: involved in the clinical follow-up of the patient and the collection of diagnostic evidences. MEPG (postgrad Student): Involved in manuscript preparation, and manuscript submission. FVA (Clinical Researcher): Manuscript preparation, manuscript editing, and manuscript submission.
Our institution does not require ethical approval for reporting individual cases.s
Written informed consent was obtained from the patient's legal guardian(s) for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
The authors declare that they have no competing interests.
All authors have read and approved the final manuscript. MRRG (Emergency Physician) Involved in the initial diagnosis and treatment of the patient. IALG (Medicine pre-grade student): Medical student: involved in the clinical follow-up of the patient and the collection of diagnostic evidences. MEPG (postgrad Student): Involved in manuscript preparation, and manuscript submission. FVA (Clinical Researcher): Manuscript preparation, manuscript editing, and manuscript submission.