Idiopathic pulmonary fibrosis (IPF) is a chronic and progressive lung disease characterized by severe fibrosis and poor prognosis. We aimed to reveal to different radiological findings of IPF and to describe a different perspective on the complexity of diagnosis. We retrospectively evaluated patients with IPF between January 2015 and April 2019 in the Department of Pulmonary Medicine, VM Medical park Samsun Hospital, Samsun, Turkey. Totally 51 patients were included in this study; 35 (68.6%) were male and 16 (31.4%) were female. The mean age was 70.8 years (min, 50-max, 86). The mean FVC, FEV1 and FEV1/FVC were 1970 ml (53%), 1860 ml (63%) and 94.4%, respectively. The diagnostic efficacy of chest roentgenograph was 58.7% in patients with IPF. The number of cases with "propeller blade" distribution (PBD) (Figure 1 and Figure 2) was 32 (62.7%). The acute attack of IPF was observed in 10 (19.6%) patients. In conclusion; it should be kept in mind that the difference in HRCT findings in the diagnosis of IPF may vary depending on the environment in which patients live. Also, we think that the external environment affects not only the diagnosis, but also the course of the disease and the acute attack and it should be supported by other studies.
Idiopathic pulmonary fibrosis (IPF), Giraffe patterns, Radiology, Acute exacerbation
Idiopathic pulmonary fibrosis (IPF) is a chronic and progressive lung disease characterized by severe fibrosis and poor prognosis, still unknown etiology. In this disease with a poor prognosis with a survival time of about 3-5 years after diagnosis, early diagnosis is important, while the diagnosis of IPF is usually delayed [1,2]. Since the chest X-ray is not disease-specific, high resolution computed tomography (HRCT) of the lung should be performed for diagnosis in all patients with suspected IPF. We retrospectively evaluated the radiological findings of patients diagnosed with IPF. In this study, we aimed to reveal to different radiological findings of IPF and to describe a different perspective on the complexity of diagnosis.
We retrospectively evaluated patients with IPF between January 2015 and April 2019 in the Department of Pulmonary Medicine, VM Medical park Samsun Hospital, Samsun, Turkey. The 2018 ATS/ERS/JRS/ALAT guidelines used for diagnosis of IPF suggested four diagnostic entities: a) UIP, b) Probable UIP, c) Indeterminate for UIP, and d) Alternative diagnosis. The HRCT criteria for a UIP diagnosis include the presence of honeycombing with or without peripheral traction bronchiectasis or bronchiolectasis and a basal and subpleural distribution. Although ground-glass opacity is common in UIP, it must be less extensive than the reticulation and be superimposed on a fine reticular pattern to be characterized as an UIP pattern. Another common feature on HRCT is mediastinal and hilar lymph node enlargement, which is present in upto 70% to 86% of patients with a UIP pattern (typically < 15 mm) [3,4]. We are classified of HRCT findings as UIP pattern with presence of honeycombing pattern (a), reticular pattern (b), traction bronchiectasis (c), ground glass opacities (d) and exacerbation type (e). Open lung biopsy was performed in suspected cases and confirmed histopathologically.
The study was performed in accordance with the ethical principles in the good clinical practice (GCP) guidelines, applicable local regulatory requirements, and the protocol was approved by local ethics review boards. All the patients read the patient information form about the study procedure and written informed consent was obtainned.
Totally 51 patients were included in this study; 35 (68.6%) were male and 16 (31.4%) were female. The mean age was 70.8 years (min, 50-max, 86). The mean FVC, FEV1 and FEV1/FVC were 1970 ml (53%), 1860 ml (63%) and 94.4%, respectively. The diagnostic efficacy of chest roentgenograph was 58.7% in patients with IPF. The radiologic progression during several years in patients with IPF were shown in Figure 3, Figure 4, Figure 5 and Figure 6. The most common comorbidity was malignancy (10.8%) in patients with IPF and lung cancer with IPF was shown in Figure 7. The number of cases with "propeller blade" distribution (PBD) (Figure 1 and Figure 2) was 32 (62.7%). The acute attack of IPF was observed in 10 (19.6%) patients. Radiologic findings of acute exacerbation in patients with IPF were showed in Figure 8, Figure 9 and Figure 10. HRCT patterns in patients with idiopathic pulmonary fibrosis were demonstrated in Figure 11 and Figure 12.
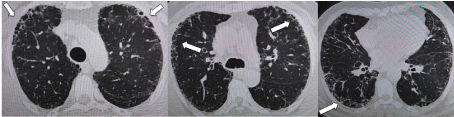 Figure 1: HRCT images are showing the "propeller blade" distribution (white arrows) in IPF.
View Figure 1
Figure 1: HRCT images are showing the "propeller blade" distribution (white arrows) in IPF.
View Figure 1
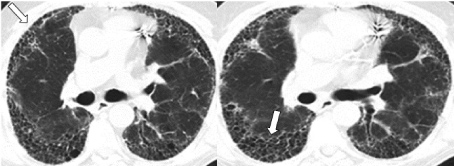 Figure 2: HRCT images are showing the "propeller blade" distribution (white arrows) in patient with IPF.
View Figure 2
Figure 2: HRCT images are showing the "propeller blade" distribution (white arrows) in patient with IPF.
View Figure 2
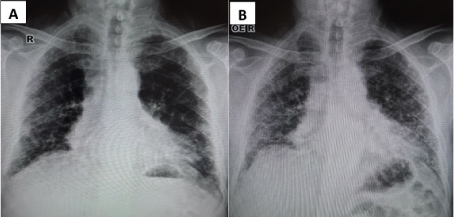 Figure 3: A) Chest roentgenographies are showing the progression of IPF from diagnosis and B) 2 years later.
View Figure 3
Figure 3: A) Chest roentgenographies are showing the progression of IPF from diagnosis and B) 2 years later.
View Figure 3
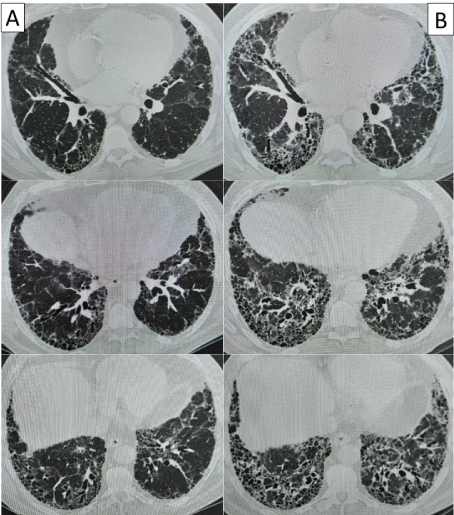 Figure 4: A) HRCT images of patient in Figure 1 are showing the progression of IPF from diagnosis and B) 2 years later.
View Figure 4
Figure 4: A) HRCT images of patient in Figure 1 are showing the progression of IPF from diagnosis and B) 2 years later.
View Figure 4
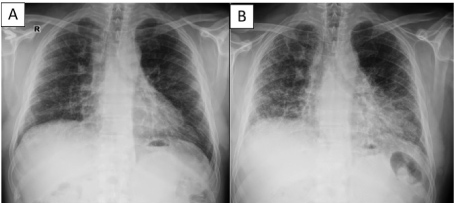 Figure 5: A) Chest roentgenographies are showing the progression of IPF from diagnosis and B) 3 years later.
View Figure 5
Figure 5: A) Chest roentgenographies are showing the progression of IPF from diagnosis and B) 3 years later.
View Figure 5
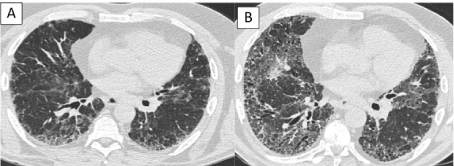 Figure 6: A) HRCT images of patient in Figure 2 are showing the progression of IPF from diagnosis and B) 3 years later.
View Figure 6
Figure 6: A) HRCT images of patient in Figure 2 are showing the progression of IPF from diagnosis and B) 3 years later.
View Figure 6
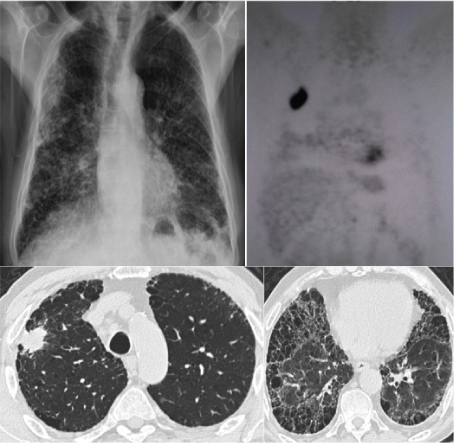 Figure 7: Chest roentgenography, PET CT scan and HRCT images are showing the lung cancer comorbidity in a patient with IPF.
View Figure 7
Figure 7: Chest roentgenography, PET CT scan and HRCT images are showing the lung cancer comorbidity in a patient with IPF.
View Figure 7
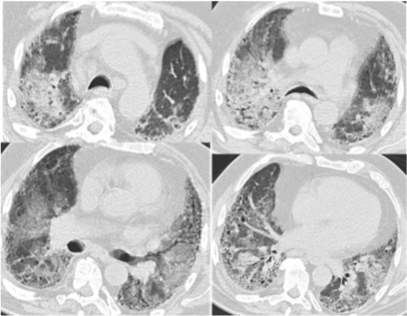 Figure 8: HRCT images are showing the ground glass opacities due to acute exacerbation in a patient with IPF.
View Figure 8
Figure 8: HRCT images are showing the ground glass opacities due to acute exacerbation in a patient with IPF.
View Figure 8
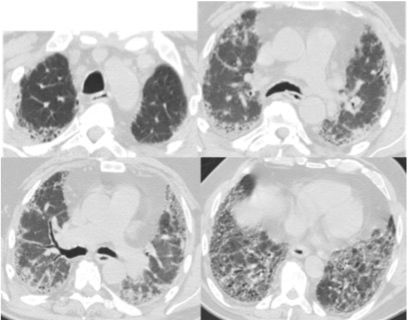 Figure 9: HRCT images of patient in Figure 8 are showing the basal UIP after acute exacerbation in a patient with IPF.
View Figure 9
Figure 9: HRCT images of patient in Figure 8 are showing the basal UIP after acute exacerbation in a patient with IPF.
View Figure 9
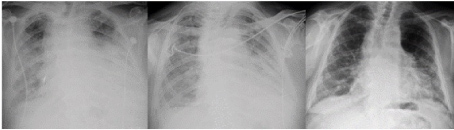 Figure 10: Chest roentgenographies of patients in Figure 8 and Figure 9 are showing the acute exacerbation and response to treatment in patients with IPF.
View Figure 10
Figure 10: Chest roentgenographies of patients in Figure 8 and Figure 9 are showing the acute exacerbation and response to treatment in patients with IPF.
View Figure 10
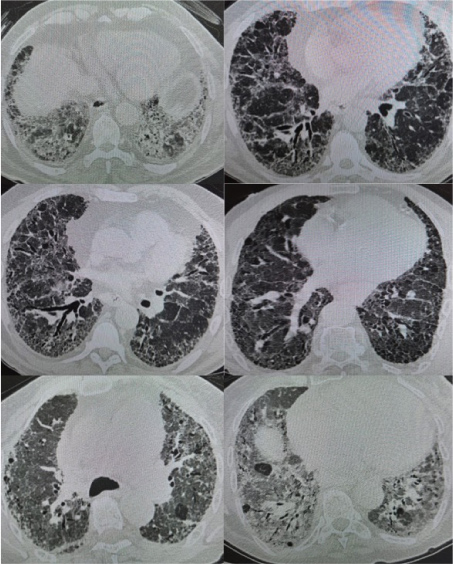 Figure 11: HRCT images of patients with IPF are showing the different patterns as UIPad, UIPabc, UIPabc, UIPac, UIPacd and UIPacd, respectively.
View Figure 11
Figure 11: HRCT images of patients with IPF are showing the different patterns as UIPad, UIPabc, UIPabc, UIPac, UIPacd and UIPacd, respectively.
View Figure 11
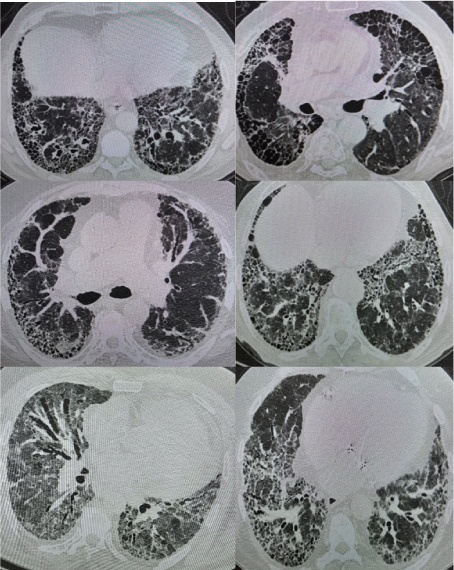 Figure 12: HRCT images of patients with IPF are showing the different patterns as UIPabc, UIPab, UIPabc, UIPac, UIPabcd and UIPab, respectively.
View Figure 12
Figure 12: HRCT images of patients with IPF are showing the different patterns as UIPabc, UIPab, UIPabc, UIPac, UIPabcd and UIPab, respectively.
View Figure 12
HRCT findings form the basis of IPF diagnosis. Typical tomographic findings seen in IPF are called UIP pattern. The positive predictive value of HRCT findings for ERP is 90-100% in various studies. Honeycombing, a common feature of IPF seen on HRCT, is crucial for an accurate diagnosis. Unfortunately, identification of honeycombing is not always straight forward, and there is some disagreement regarding its imaging features [5]. In the presence of a typical clinical presentation (> 50 years of age, insidious onset progressive dyspnea), the typical UIP pattern in HRCT may be clinically diagnosed with IPF without a biopsy in the multidisciplinary approach if other possible causes of UIP are excluded [6-10]. In our study, the average age of the errors was 70.8 and the lowest age was 50 years and the oldest patient was 86-years-old. We noted that the diagnostic efficacy of chest roentgenograph was 58.7% in our patients with IPF.
Another HRCT characteristic that can be helpful in making a diagnosis of UIP is the so-called "propeller blade" distribution (PBD). This variant gets its name from the fact that, when seen on sequential axial images from caudal to cranial, the honeycombing or reticulation changes from being predominantly posterior to anterior [11]. In our study, the rate of PB distribution was 62.7%. We think that the definition of IP giraffe pattern in IPF. Is similar to the patterns of giraffes in IPF and that radiological confusion in these patients can be explained a little. Each giraffe has its own pattern style. In this style, each giraffe has its own particular order. Although there are some disagreements about the exact number of subtypes in the scientific world, there are nine giraffe patterns. These are Reticulated, Kordofan, Nubian, Angola, South Africa or Cape, Rothschild or Ugandan, West Africa or Nigerian, Thornicroft and Masai (Figure 13).
 Figure 13: The world’s giraffe patterns are showing just like IPF patterns.
View Figure 13
Figure 13: The world’s giraffe patterns are showing just like IPF patterns.
View Figure 13
They are all immediately recognized as giraffe stains, but some stand out slightly more than other subspecies models. For example, Angola giraffes have drawn indentations in most of their stains. Rothschild’s giraffes have wavy edges in their stains and are a flat cream under the knees. Masai giraffes have stains similar to deep, rounded oak leaves. The dots make it easy to see giraffes in the zoo environment, but it acts as a camouflage in the wild. They live mostly in African savanna, and they are full of long grasses and trees that provide shady shadows. Random dots make it difficult for hunters to detect in harmony with moving shadow patterns. us; We think that different patterns in giraffes depending on the external environment and external factors, radiological findings may be different depending on the external environment in which they live and breathe in IPF patients. So that, we are classified of HRCT findings as UIP pattern with presence of honeycombing pattern (a), reticular pattern (b), traction bronchiectasis (c) and ground glass opacities (d). We think that this classification will facilitate to solving the complexity of IPF diagnosis (Figure 14 and Figure 15).
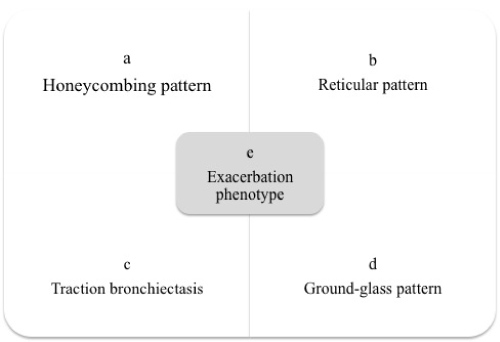 Figure 14: The figure showing the IPF classificationwith HRCT patterns.
View Figure 14
Figure 14: The figure showing the IPF classificationwith HRCT patterns.
View Figure 14
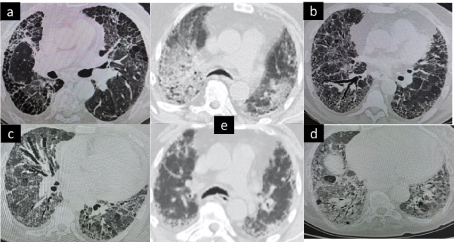 Figure 15: The HRCT images are showing IPF classification with patterns.
View Figure 15
Figure 15: The HRCT images are showing IPF classification with patterns.
View Figure 15
IPF, a disease with high mortality, may be associated with acute respiratory distress in many patients in days, although there is a decrease in respiratory function over the years [12]. This table is called P IPF acute exacerbation maktad if the original diagnostic criteria are met. The frequency is 10-20%, even up to 40% [13,14]. In our study, the rate of acute exacerbation of IPF was 19.6%.
Acute exacerbation of IPF is an important mortality (short-term mortality rate close to 50% and median survival is 3-4 months) and is a cause of morbidity [15]. In a patient diagnosed with IPF or newly diagnosed with IPF, clinical worsening of dyspnoea, radiologically elevated bilateral iced glass densities and/or consolidation appearances on the UIP view on the ground suggest the possibility of acute exacerbation [13,16,17]. According to the updated definition, IPF-acute exacerbation is characterized by acute respiratory deterioration clinically associated with a newly emerged, alveolar abnormality.
In conclusion; it should be kept in mind that the difference in HRCT findings in the diagnosis of IPF may vary depending on the environment in which patients live. Also, we think that the external environment affects not only the diagnosis, but also the course of the disease and the acute attack and it should be supported by other studies.
"The authors have no conflicts of interest to declare". All of authors approved the datas and manuscript.
The research article data used to support the findings of this study are available from the corresponding author upon request.