Endotracheal suctioning is a common procedure for intubated patients. In Songklanagarind hospital, the sterile technique for endotracheal suctioning is used routinely in all areas except in the operating theater.
To compare bacterial contamination from endotracheal secretion between the clean and the sterile technique.
This prospective randomized controlled trial in 276 patients of age more than 18-years-old who had American Society of Anesthesiologists (ASA) class I-III and scheduled for elective surgery and had no risk of aspiration were enrolled and randomly assigned into two groups. The patients with general anesthesia with oroendotracheal intubation were included. Endotracheal suctioning was performed by the decision of anesthesiologists or anesthetic nurses with sterile or clean technique regarding the group assignment. Secretion collected from the suction catheter was sent to the microbiology laboratory for microbial culture. The microbiologic bacterial results were reported within 7 days. Patients were followed up for respiratory symptoms every day for 7 days after the surgery.
There were the non-pathogenic and pathogenic bacterial growth, and fungus from the culture of endotracheal secretion similarly in both clean and sterile groups. The clean group had positive bacterial growth of 64.2% and the sterile group had 57%. The difference was not statistically significant (p = 0.346). The contamination score in the clean and sterile group were 19 and 15 respectively. The incidence of respiratory symptoms such as a cough without fever was low (5%) postoperatively and there was no postoperative pneumonia in both groups.
The incidences of bacterial contamination from endotracheal suctioning with clean and sterile technique were similar. But the clean group tended to has higher contamination than the sterile group.
Endotracheal suctioning, Bacterial contamination
Because of the limitation of the secretion clearance in mechanically ventilated patients, the regular endotracheal suctioning is needed and it's a common procedure during intraoperative period for maintaining bronchial hygiene and prevention of secretion obstruction. However, the endotracheal suctioning has the potential to dislodge viable bacteria from the endotracheal tube into the lower airway. Therefore, aseptic technique is essential in order to prevent upper and lower respiratory tract infection corresponded to The American Association of Respiratory Care [1] suggestion related to the endotracheal suctioning.
The previous studies of intraoperative endotracheal suctioning has been investigated for the evidence of ventilator-associated pneumonia (VAP) only by comparing the opened suction and closed suction system [2]. For the multi-used closed suction system, the patient and the ventilator circuit need not to be disconnected to each other, therefore, the potential for dispersal of micro-organisms reduces. However, the contaminating bacteria from the initial pass of the suction can grow in the warm, humid plastic sheath [3]. Many studies reported that the type of the tracheal suction; opened versus closed, had no effect on development of VAP [4-6]. Bacterial contamination has been reported from the gloves and equipments such as ventilators [7]. With sterile tracheal suction, bacterial cultures were positive in 67% of patients after intubation for 24 hours and the most common organisms was Streptococcus species (28%) [8].
The clean, open suctioning technique is a routine practice in the operating theater in Thailand. The operating theater is generally a sterile area, so the disposable gloves with sterile suction catheter are commonly used in our and many hospitals. Sometime, lubricant gel is also applied with the suction catheter.
This study aimed to compare bacterial contamination from the endotracheal suctioning by using the clean and sterile technique.
This study was registered at the clinicaltrials.in.th with the registration number: TCTR20150709002. After the approval from institutional ethics committee, patients aged more than 18-years-old who had American Society of Anesthesiologists (ASA) class I-III and scheduled for elective surgery were enrolled in this study. The patients who had recent respiratory tract infection, gastro-eosophageal reflux disease, risk of aspiration, intubated patient, immune-compromised patients and patients who had tracheal cuff leakage before suctioning were excluded from the study. The inform consent was obtained from every patient.
Patients were randomly assigned into two groups (Clean group and Sterile group) by using computer-generated randomization table. The randomization codes were then enclosed and sealed in opaque envelopes. At the operating theater, demographic data were recorded by anesthetic nurses or anesthesiologists. After oroendotracheal intubation was performed successfully by one attempt with conventional laryngoscope with no stylet and lubricant gel, the tracheal cuff was checked for leakage by palpation then the anesthesiologists or anesthetic nurses opened the concealed envelopes to identify the assigned group.
During extubation at the end of surgery, endotracheal suctioning was performed for one of these following reasons; routine practice, presence of the secretion in the endotracheal tube or increased airway pressure. All patients were pre-oxygenated with 100% oxygen 3-5 minutes before suction and were suctioned with suction catheter number 14 French, which was not larger than 2/3 of internal diameter of endotracheal tube. Endotracheal secretion was collected only from the first time of suction in each patient. Peripheral oxygen saturation was monitored during endotracheal suctioning. Oxygen saturation below 94% was recorded as desaturation.
In the Clean group, the anesthesiologist or anesthetic nurse wearing the non-sterile disposable gloves disconnected the breathing circuit and performed endotracheal suction by using the sterile suction catheter from the package which was opened since at the time of the endotracheal intubation. A sterile suction catheter had a collecting bulb to collect secretion for bacterial culture. The secretion was kept refrigerated overnight at 4º Celsius before sending to the microbiologic laboratory in the morning of the next day.
In the Sterile group, the anesthesiologist or anesthetic nurse wearing the sterile gloves performed the endotracheal suctioning by using the sterile suction catheter which was immediately opened from the package. There was a non-sterile glove wearing assistant to disconnect the endotracheal tube from the breathing circuit to maintain the sterile technique. The rest of the specimen collection steps were the same as in the clean group.
In microbiological laboratory, every specimen was streaked in four quadrants of three plates of the agar (blood, Chocolate and MacConkey agar) for aerobic bacteria and yeast for 7 days. The names of bacteria or yeast were then reported. The enumeration guide of the colonial morphotypes were graded from the estimated colonies in four quadrants of the agar: Rare = in one quadrant only, ignoring a few colonies in the other quadrants; few = up to second quadrants, ignoring a few colonies in the other two quadrants; moderate = up to the third quadrant, ignoring a few colonies in the fourth quadrants; numerous = up to the fourth quadrant). The microorganisms which are not normal flora of the upper airway were reported as pathogen.
All of the patients were followed up every day for 7 days postoperatively for respiratory symptoms such as cough, pneumonia, the need for oxygen supplement or re-intubation. If the patients remained intubated up to 48 hours or re-intubated from respiratory infection within 7 days postoperatively, the endotracheal suctioning was performed again to check whether it was the same pathogen or not. If the patients were discharged from the hospital within 7 days postoperatively, they were called by telephone at the seventh postoperative day.
Withdrawal criteria included patients who had no secretion by suctioning, patients who had indication to change endotracheal tube and positive cuff leak test by palpation before suction.
Sample size was calculated using the bacterial contamination rate with sterile technique of endotracheal suctioning which was 0.67 [4] with 80% power and the drop out of 10%, there for the number of populations was 138 for each group.
The patients' gender, age, ASA classification, surgical site, time from intubation to suction, indication of suction, incidence of desaturation, amount and morphotypes of the microbiological cultures (bacteria, yeast, fungus) were recorded. Data were filled in Epidata version 2.0.7.22 and then analyzed using program R version 2.14.1. Results are expressed as mean ± SD and percentage. Chi-square test and Fisher's exact test was used to compare nominal data. T-test was used to compare continuous data. All data were normal distribution. P-value > 0.05 was used for significant data.
Two hundred eighty-one patients were enrolled from September 2015 to June 2016. Five patients were excluded due to failed intubation in the first attempt. Fifty-six patients were withdrawn from this study due to no secretion from suctioning and one patient was withdrawn due to the violation of sterile technique in the sterile group (Figure 1). There were no significant differences between two groups in term of sex, age, ASA classification, surgical site, time from intubation to suction, indication of suction and incidence of desaturation (Table 1).
Table 1: Patients demographic data. View Table 1
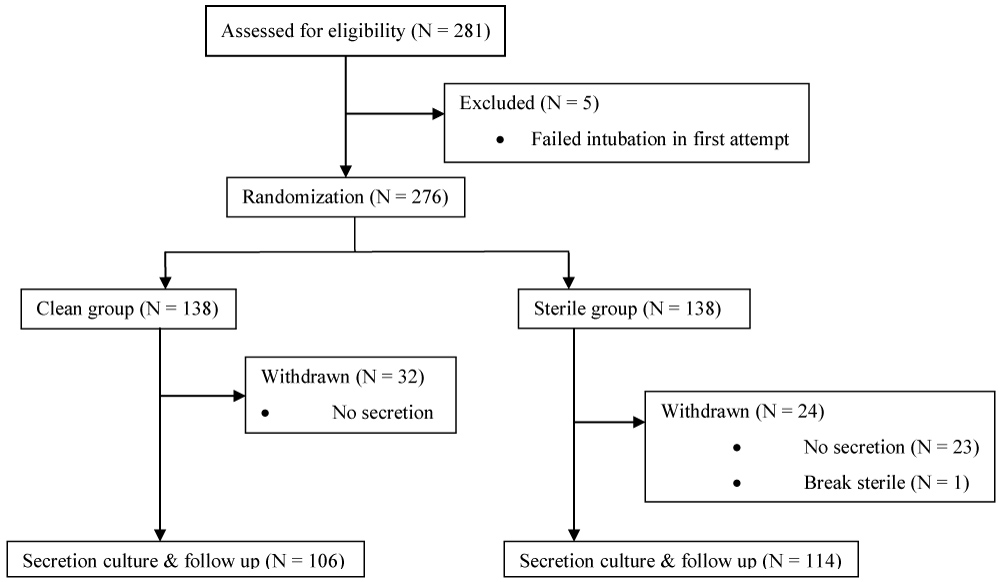 Figure 1: Consortium flow chart in the study.
View Figure 1
Figure 1: Consortium flow chart in the study.
View Figure 1
The incidence of positive bacterial culture between the clean group and the sterile group was not different (64.2% vs. 57% respectively, p = 0.346) (Table 2). The 95% confident interval of the Clean and the Sterile group were 0.549-0.731, and 0.479-0.661 respectively.
Table 2: Microbiological bacterial report of the clean and sterile groups. View Table 2
The pathogenic bacteria and fungus (Candida albicans) were cultured from the secretion in both groups. The culture was positive for yeast in one patient in the Clean group.
The pathogen contamination was calculated into the score in order to compare the severity of pathogens contamination in both groups. The score was calculated by the formula below.
Pathogens Contamination Score = n × level of contamination
The level of contamination were graded as; Rare = 1, Few = 2, Moderate = 3 and Numerous = 4.
So the Clean group had Pathogens Contamination Score higher than the Sterile group (19 vs. 15 respectively) (Table 3 and Table 4).
Table 3: Microbiology culture report of the clean group. View Table 3
Table 4: Microbiology culture report of the sterile group. View Table 4
Most of the bacterial growth from endotracheal secretion are normal throat flora and some of them are pathogens (Table 3 and Table 4). Most common bacterial growth in both groups was Alpha-streptococcus not group D not pneumonia, and Neisseria spp. which are normal throat flora. One patient from the sterile group who was scheduled for changing vacuum dressing under general anesthesia had Acinetobacter baumannii. In the secretion but he didn't have any postoperative respiratory symptoms within 7 days.
From 276 patients in this study, there were 14 patients (5%) who had respiratory symptoms within 7 days postoperatively. In the Clean group, four patients had a productive cough without fever (one patient had positive culture as Alpha- Streptococcus and Neisseria spp., one patient had negative culture, and two patients had no secretion for bacterial culture). One patient had left lower lung atelectasis and needed oxygen supplement for 3 days postoperatively but he had no secretion from suctioning. One patient was re-intubated on the second postoperative day due to sepsis from intra-abdominal infection, his intraoperative endotracheal secretion culture was positive for Alpha-Streptococcus and Neisseria spp. In the Sterile group, six patients had a productive cough without fever (one patient had positive culture for Alpha- Streptococcus and Neisseria spp., one patient had a positive culture for Staphylococcus coagulase negative, three patients had the negative culture and one patient had no secretion). Two patients needed oxygen supplement (one patient with a history of COPD had bronchospasm and received bronchodilator nebulized for 4 days, his culture of secretion was positive for Alpha-Streptococcus and another patient needed oxygen cannula for 3 days without any other respiratory symptoms).
In this study, the incidences of positive bacterial culture from endotracheal suctioning between the Clean group and the Sterile group were similar (64.2 and 57%, respectively). Several trials related to the endotracheal suction system has mostly been focused on the comparison between closed and open system in terms of the incidences of ventilator-associated pneumonia (VAP) or incidences of contamination in intensive care patients. For the open suctioning system, none of the previous studies compared the clean and sterile endotracheal suctioning in operating theater. In this study, the bacterial contamination rates were similar between the two techniques. It may be due to the clean area of the operating theater, and the low risk of cross-contamination from patient to another patient because one patient at a time is in the theateral together with the change of some new medical equipment after surgery.
The colonization of the airway has been reported that it was prone to the development of nosocomial pneumonia [9,10]. The duration of mechanical ventilation and colonization of the upper respiratory tract are the most important risk factors for VAP [11]. After 24 hours, the patients who were orally intubated for at least 24 hours had sputum cultures positive for pathogens as high as 67% [8]. Speksnijder H, et al. compared sterile endotracheal suctioning to the non-sterile suction procedure on the reduction of airway colonization in the patients on mechanical ventilation for more than 48 hours. They found that the exogenous colonization was not significantly different between the non-sterile (27.5%) and the sterile group (25%) [12]. These incidences were lower than those in our study which might be explained by the differences in the use of selective decontamination of digestive tract and definition of airway colonization. Unlike the operating room, the cross contamination is the major route to nosocomial infection in the intensive care unit [13].
With the more endotracheal suctioning performed, the more likely the patient would be exogenously colonized [12]. Cook, et al. reported a cumulative increased risk of VAP with time, with 3% per day in the first week of mechanical ventilation [14]. The gram-positive bacteria from the mouth were commonly colonized within 12-36 hours after endotracheal intubation [15,16]. Most of the surgical procedures were not last longer than 12 hours. Therefore, in our study, the duration of mechanical ventilation was possibly inadequate to have bacterial colonization in the lower airway. Additionally, the endotracheal suctioning in each patient was only performed only once at the end of surgery. In this study, one patient in the Sterile group who had Acinetobacter baumannii. In the secretion had multiple recent surgical operations with general anesthesia and endotracheal intubation, so he might have an increased risk for endogenous bacterial colonization in his airway.
Similar VAP rates were found in the earlier trials compared between the closed and the open endotracheal suction system [5,17-20]. Meta-analysis also failed to demonstrate a positive impact of closed suction system on VAP, morbidity and mortality compared to the open systems [21-24]. However, using closed suction system has been demonstrated to decreased in incidence of VAP significantly [2,25]. The use of closed suction system is also recommended as part of a VAP prevention program [1].
The risk of contamination in the clean group was expected to be higher than that in the sterile group. This contamination may cause the respiratory tract infection postoperatively; therefore, all of the patients were followed up for 7 days postoperatively. Even the pathogenic bacteria and fungus were found from the secretion in both groups. The incidence of postoperative respiratory symptoms was not different between the two groups. The incidence was approximately 5%, which were 6 patients in the Clean group and 8 patients in the Sterile group. Most of them developed a cough without fever postoperatively. No patient had diagnosed with postoperative pneumonia within a week. Many potential pathogens such as Staphylococcus aureus and Streptococcus, may be introduced into the lower part of the respiratory tract during intubation [15-17]. Similar to the previous studies, the Streptococcus, and Staphylococcus were the common bacteria in our specimens. Early-onset VAP, which occurs between 48 to 72 hours after intubation, is usually the result of aspiration and is often due to S. aureus, Haemophilus influenzae, or Streptococcus pneumoniae. Late-onset VAP is often caused by antibiotic-resistant organisms, including Pseudomonas aeruginosa, methicillin-resistant S. aureus, Acinetobacter species, and Enterobacter species [12,26]. The gram-negative pathogens were found on 22-28%, and yeast on 6% of the airway devices [8]. George DL, et al. reported a 12.5% prevalence of colonization with gram-negative bacteria [12]. The most common gram-negative species were Pseudomonas aeruginosa (15.6%), Enterobacter species (10.9%), and Klebsiella pneumoniae (7.0%) [27]. Acinetobacter buananii but not Pseudomonas aeruginosa were found in our study. The colonization with Acinetobacter spp. and Pseudomonas aeruginosa was demonstrated to be more frequent in the closed suction group than in the open suction group [4]. In this study, yeast was cultured in one patient in the Clean group but none in the Sterile group. However, the patient did not develop the sign and symptoms of respiratory infection postoperatively.
This study may have some limitations as it was a single center. Anesthetic nurse students, anesthetic nurses, anesthetic residents and staff anesthesiologists who performed intubation had variation in skill level and experience. Although they could intubate successfully in one attempt, it could not be confirmed that the endotracheal tube did not contaminate any oral secretion before passing into the trachea. We used a cuff leak test by palpation on the neck with positive pressure ventilation at 20 cmH2O as a routine. However, we did not monitor intraoperative cuff pressure. The lubricant gel was not applied in our study because it may be a confounding factor of contamination despite it sometimes was used in routine practice of our hospital. The microorganisms in this study were not counted in CFU because the protocol is complicated and has a high cost. Finally, the cultures of tracheal aspirate is not a specific diagnostic method because of the lower respiratory tract colonization and a high percentage of false-positive results. The presence of a potential pathogen in a sputum culture is not definitive for a diagnosis of pneumonia.
There was no significant difference of the bacterial contamination from the open system of the oroendotracheal suctioning between the clean and the sterile technique in the operative environment, but the clean technique tended to has the higher incidence of airway colonization.
The authors report no conflicts of interest.
The authors acknowledge the financial support received from Prince of Songkla University, for their support and encouragement in carrying out this work.