Since its discovery in December 2019, the Coronavirus disease 2019 (COVID-19) has spread to more than 70 countries around the world. The United States alone has seen more than 1.5 million cases, with more than 100,000 deaths to date [1]. The most common presenting symptoms are fever, cough and shortness of breath with median incubation periods of 5 days [2]. Severe symptoms can develop as a result of the aggressive inflammatory response. The role of bronchoscopy has been limited in severe cases and results are infrequently reported. We report a case of a young male with severe COVID-19 who developed multiple endobronchial polyps in the tracheobronchial tree seen on bronchoscopy examination.
A 29-year-old male with no significant past medical history presented with cough, chills, subjective fevers, fatigue, body aches and shortness of breath for one-week duration. Vitals on admission were BP: 124/74 mmHg, HR: 100 bpm, RR: 20/min, Temp: 97.6 °F. Chest X-ray (CXR) revealed bilateral infiltrates. SARS-CoV-2 polymerase chain reaction test was positive. His condition rapidly deteriorated requiring intubation for acute hypoxemic respiratory failure. Analysis of repeat CXR, arterial blood gas and clinical course was consistent with severe acute respiratory distress syndrome. His hospital course was complicated by septic shock and femoral Deep Vein Thrombosis (DVT). The patient received ceftriaxone, azithromycin, hydroxychloroquine and enoxaparin. After 2.5 weeks since admission his CXR showed worsening infiltrates and a bronchoscopy was performed which showed erythematous mucosa only with mucopurulent material. The patient then developed cytokine storm with high grade fever of 105.9 °F and C-reactive protein of 15.3 mg/dl. His serum IL-6 level was 540 pg/ml and was given tocilizumab. He also received convalescent plasma. A repeat bronchoscopy was performed a week later due to thick secretions and atelectasis showed friable broad-based endobronchial polyps throughout the tracheobronchial tree (Figure 1). Biopsy of lesions was not obtained as patient was high risk for bleeding due to full dose anticoagulation for DVT. The patient was given methylprednisolone for 7-day duration. Eventually patient was stabilized and transitioned to a tracheostomy for continued ventilator support. A repeat bronchoscopy was performed 5 weeks after admission, showing reduction in number of polyps and resolution at multiple sites (Figure 2). The patient was later transferred to a step-down unit where he continued to improve and was finally decannulated and discharged home after 10 weeks of hospitalization.
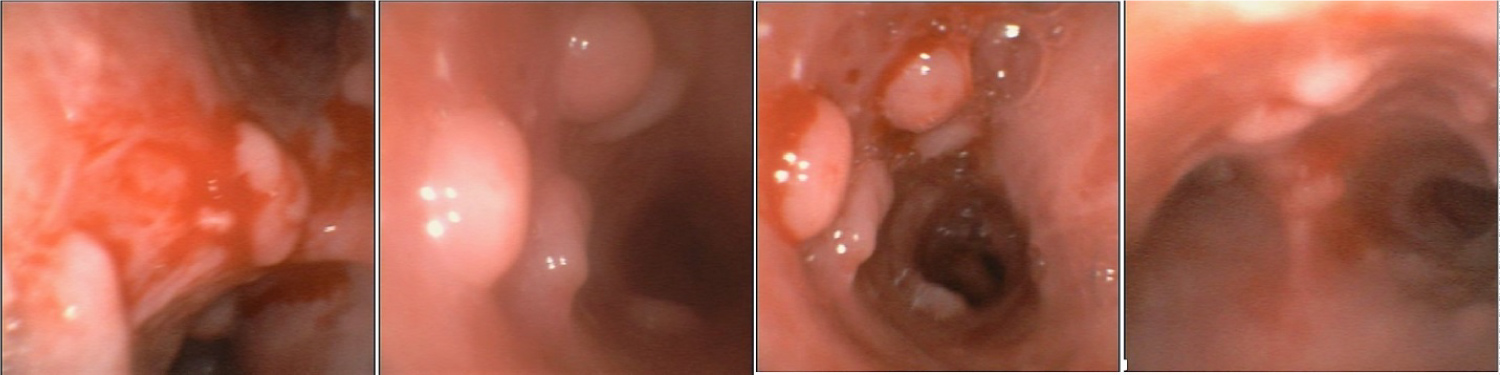 Figure 1: Bronchoscopy showing multiple endobronchial polyps.
View Figure 1
Figure 1: Bronchoscopy showing multiple endobronchial polyps.
View Figure 1
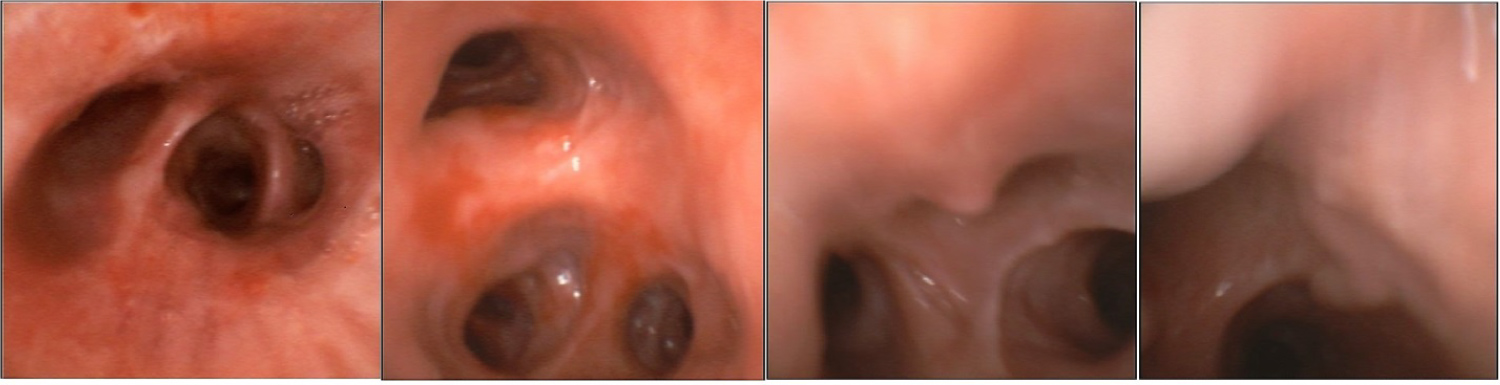 Figure 2: Resolution of endobronchial polyps on repeat bronchoscopy.
View Figure 2
Figure 2: Resolution of endobronchial polyps on repeat bronchoscopy.
View Figure 2
Bronchoscopy examination of COVID-19 pneumonia has not been well documented in literature. Current guidelines from American Association for Bronchology and Interventional Pulmonology (AABIP) for COVID-19 are not supportive of bronchoscopy due to its limited usefulness in this disease process and potential for increased aerosol exposure to health-care workers [3,4]. The few documented COVID-19 bronchoscopy results revealed only mucosal swelling, mucopurulent secretions and congestion [5]. WHO/IASLC classifies inflammatory endobronchial polyps as a distinct type of non-neoplastic tumors of lung [6]. Although endobronchial polyps have been reported in some inflammatory conditions for example bacterial infections and malignancy [7-9], we are reporting the first case of endobronchial polyps related to SARS-CoV-2 infection. A case report by Adams, et al. showed multiple polyps post thermal inhalation injury which resolved after steroid course strongly indicating inflammation as primary cause. The mechanism behind the COVID-19 pathogenesis is thought to be a result of a severe inflammatory response implicating progressive multi-organ damage [10]. Our patient did not have these endobronchial polyps on initial bronchoscopy; their development strongly suggests COVID-19 as the primary insult through inflammatory mechanisms [11-13].
While bronchoscopy has not played a large role during this pandemic, it should be considered to further enhance our understanding of this disease process.