Purpose: There are variable long-term pulmonary outcomes of children with congenital diaphragmatic hernia (CDH). Diagnostic modalities evaluating pulmonary function can be limited by patient compliance. Pulmonary perfusion scintigraphy is a diagnostic tool to evaluate lung development in younger children. Presence of a hernia sac is known to correlate with less severe disease but little has been reported on any correlation with lung size and function. The purpose of this study was to evaluate the relationship between presence of a hernia sac, pulmonary perfusion and CDH defect size.
Methods: Records of all children treated for CDH at our institution from January 2009 to December 2018 were reviewed. A subset of these children underwent lung perfusion scintigraphy. We hypothesized that the presence of a hernia sac would affect future perfusion studies. We assessed this with two linear regression models.
Results: One hundred thirty-three children were treated for CDH over 10 years. Twenty-nine children (22%) underwent pulmonary scintigraphy, 9 of whom (31%) had a hernia sac. There was no correlation between hernia sac presence and improved perfusion (R2 = 0.005, p = 0.7). There was a correlation between area of the defect (cm2), and perfusion difference between the two lungs (R2 = 0.56, p < 0.05). When adjusting for presence of the hernia sac, the fit of the model was unchanged (R2 = 0.57, p < 0.05).
Conclusions: As expected, there is a correlation between CDH defect size and lung perfusion. However, presence of a hernia sac did not impact lung function as determined by perfusion scintigraphy.
Congenital diaphragmatic hernia, Lung perfusion, Outcomes
Congenital diaphragmatic hernia (CDH) occurs in approximately one of 3000 births due to failure of development of the diaphragm muscle resulting in lack of separation between the abdominal and thoracic cavities [1,2]. Abdominal contents develop in the thoracic cavity, resulting in varying degrees of pulmonary hypoplasia. CDH is a challenging condition for pediatric surgeons to manage because of the wide array of outcomes. With respect to pulmonary morbidity specifically, the variety of outcomes can often make it difficult to appropriately counsel parents and provide anticipatory guidance about the course of their child's care. Given recent improvements in neonatal and critical care, an increasing proportion of CDH patients are surviving the neonatal period, and the need to better prognosticate and identify areas of intervention that can improve survival and long-term morbidity has increased [3,4].
The prognostic value of a hernia sac is one factor currently being investigated. A hernia sac is an extension of the peritoneal lining that covers the abdominal contents. In a series of studies from 2013-2018 there is data to suggest that the presence of a hernia sac is associated with improved markers of early pulmonary function [5-7]. Both pre-natal and post-natal assessments were evaluated including observed-to-expected lung-head-ratio [5,8], need for inhaled nitric oxide [9], need for ECMO [5,8], and prevalence of pulmonary hypertension [5,8]. The presence of a hernia sac was associated with decreased need for a mesh patch during surgical repair [5,8]. In terms of survival, the current data are mixed with some studies showing improved survival outcomes [6,7] for patients with a hernia sac and others showing no difference [5].
Pulmonary perfusion in patients with CDH is known to be decreased and thought to slowly improve during the post-natal period before plateauing [10-14]. Our institution has performed pulmonary perfusion scintigraphy on CDH patients as part of their routine follow-up care. While there have been studies evaluating the developmental changes in pulmonary perfusion for CDH patients during the first several months of life, no study to date has evaluated for an association between presence of a hernia sac and perfusion scan results. Understanding the relationship between presence of a hernia sac and pulmonary perfusion will provide insight into mechanisms of the observed improved pulmonary function in this subpopulation of patients.
We conducted a retrospective chart review of all patients treated for CDH at Seattle Children's Hospital who were born between January 1, 2009 and December 31, 2018. All children treated during this time period were eligible for inclusion in the study. Patients were excluded if they did not have an operative report with details about the hernia repair, or if they did not have a perfusion study. Demographic variables included sex, gestational age, birth weight, hernia side, presence of congenital comorbidities need for ECMO, patch repair, need for oxygen at discharge and pulmonary hypertension at time of discharge. Exposure variables included presence of a hernia sac, and defect size classified both by area in square centimeters and according to the CDH Study Group Defect Descriptions [15]. The CDHSG defect descriptions were used to allow for interpretation of results based on an accepted classification system. Defect area was also calculated using the largest diameter and a perpendicular width measurement. This metric was chosen because of recent evidence showing poor inter-rater reliability of judgment of CDHSG based on operative reports [16].
The outcome of interest was degree of ipsilateral perfusion defect. Perfusion scans were ordered per clinical judgment of the provider. Perfusion scans were performed without sedation. The protocol for the scan included intravenous injection of MAA particles labeled with 0.5 mCi of technetium-99 radiotracer, followed by planar imaging of the lungs. Total counts of radiotracer were acquired from anterior and posterior perspectives and geometric mean perfusion to each lung was calculated. Institutional normal values are 55% tracer uptake in the right lung and 45% tracer uptake in the left lung. Ventilation data was not collected. Pulmonary perfusion was evaluated as both a binary (normal vs. abnormal) and continuous variable (difference in perfusion between the affected and unaffected lungs). Classification of normal vs. abnormal was based on the assessment of a board-certified radiologist. Linear regression analysis was performed to assess for an association between presence of a hernia sac and perfusion difference. Two linear regression models were fit to assess for an association between hernia defect size in square centimeters and perfusion difference, one of which adjusted for presence of a hernia sac. This study was approved by the Institutional Review Board at Seattle Children's Research Institute (IRB# STUDY00002052).
From January 1, 2009 to December 31, 2018 there were 133 children treated for CDH at Seattle Children's Hospital. Twenty-nine children (22%) underwent pulmonary scintigraphy, 9 of whom (31%) had a hernia sac. Twenty-one (72%) patients had defect dimensions measured and defect area calculated. Of the patients with missing defect dimensions 3 had hernia sacs and 5 did not. Twenty-three patients (79%) had abnormal perfusion scan results. One patient who did not have a hernia sac underwent perfusion scintigraphy during hospitalization and died prior to discharge. There were no significant differences in descriptive variables between groups defined by presence or absence of a hernia sac (Table 1). For the entire cohort the mean age at perfusion scan was 1.48 years (SD 1.40), and each patient had one perfusion study. When children had abnormal perfusion imaging, the ipsilateral side had decreased perfusion compared to the contralateral side. There were no significant differences in the defect sizes as defined by the CDH Study Group Classifications, defect size in square centimeters, abnormal results of perfusion scintigraphy, or mean difference in perfusion between the two lungs across groups defined by presence of a hernia sac (Table 2). Figure 1 demonstrates the relationship between perfusion difference and area of the hernia defect in square centimeters. Linear regression analysis identified a correlation between these two variables (R2 = 0.56, p < 0.05). The fit of the model was unchanged when adjusted for presence of a hernia sac (R2 = 0.57, p < 0.05). In both models, a 1 square centimeter increase in defect area was associated with a 1.5% greater absolute difference in perfusion of the two lungs.
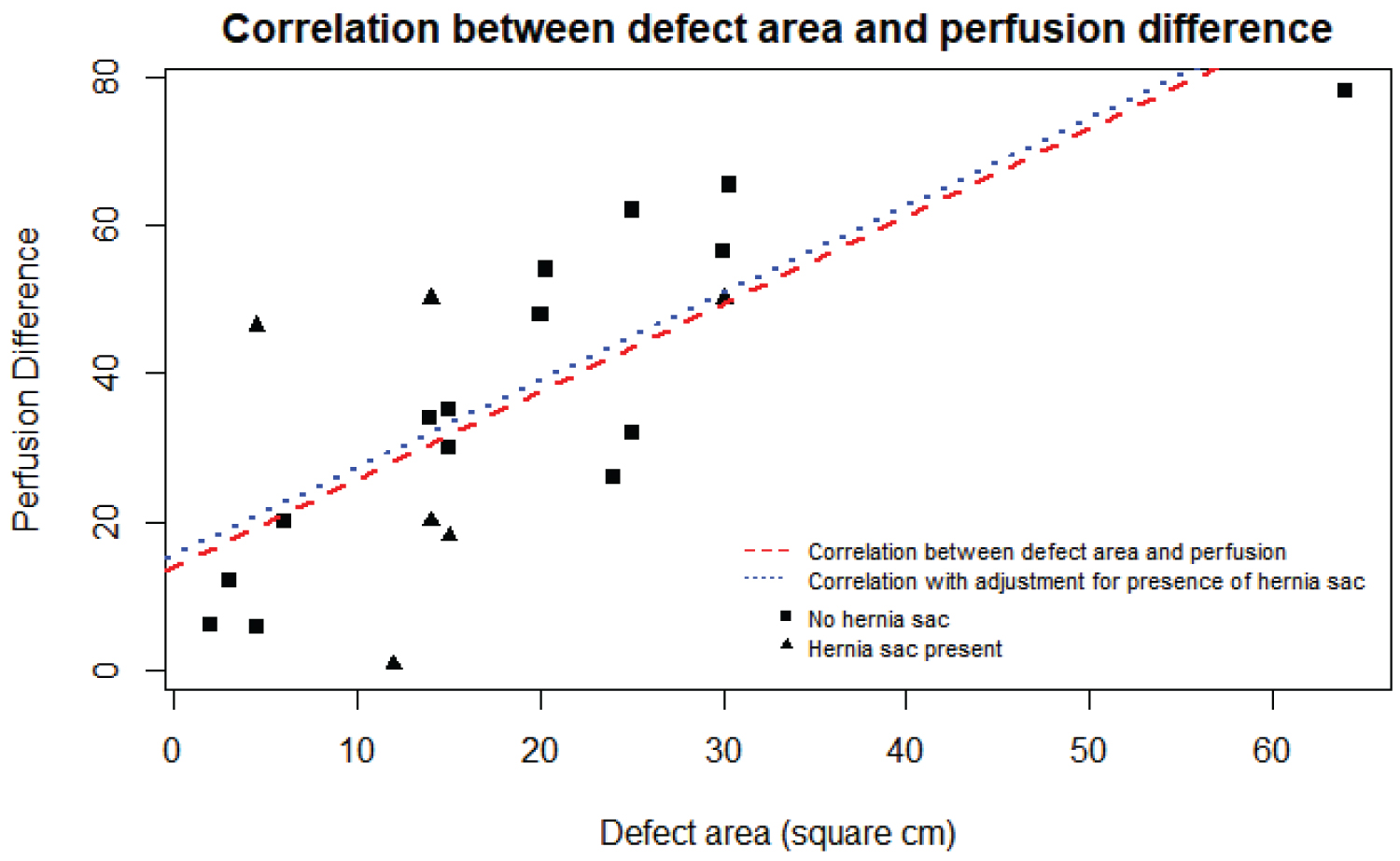 Figure 1: Correlation between defect area and perfusion difference.
View Figure 1
Figure 1: Correlation between defect area and perfusion difference.
View Figure 1
Table 1: Hernia sac presence and perfusion. View Table 1
Table 2: CDH study group classifications, defect size in square centimeters, abnormal results of perfusion scintigraphy, or mean difference in perfusion between the two lungs across groups defined by presence of a hernia sac. View Table 2
We sought to evaluate the relationship between presence of a diaphragmatic hernia sac and pulmonary perfusion scintigraphy results for patients with CDH. As expected, perfusion scan results were abnormal in a majority of patients, perfusion was decreased in the ipsilateral lung, and there was a correlation between CDH defect size and lung perfusion. Patients with a hernia sac were less likely to have pulmonary hypertension at discharge. However, presence of a hernia sac did not influence need for ECMO, need for a patch repair, need for oxygen at discharge, or ipsilateral perfusion defect.
Approximately 30% of our study population had a hernia sac, consistent with large studies reporting the frequency of this finding in CDH patients. Our results are different from prior evaluations of the influence of a hernia sac on pulmonary outcomes. A 2013 study from Zamora, et al. and a 2019 study from Oliver, et al. showed that presence of a hernia sac is associated with decreased need for patch repair, ECMO, and supplemental oxygen at 30 days of life. These same studies showed decreased duration of intubation and decreased proportion of patients with pulmonary hypertension [5,8]. Levesque, et al. showed that presence of a hernia sac is associated with decreased need for inhaled nitric oxide and decreased duration of ventilation [9]. Finally, a 2018 study from Bouchghoul, et al. found an association between a hernia sac and increased survival at 28 days and 6 months post-natally [7].
To our knowledge this is the first study to assess for an association between presence of a hernia sac and results of perfusion scintigraphy. Other groups have evaluated perfusion scan results to stratify patient groups, including changes in lung perfusion over time, and as related to defect size [14]. Multiple studies have demonstrated that perfusion follows a developmental trajectory, with increasing perfusion of the ipsilateral lung over the first year and a half post-natally, after which time perfusion plateaus [10-12,14]. A recent study from Dao, et al. evaluated the longitudinal relationship between V/Q ratio and CDH defect size and found that baseline V/Q ratios were similar between patients with smaller defects and patients with larger defects. However, V/Q mismatch increased with age in those patients with larger defects, and the authors postulate this was driven by worsening perfusion defect relative to increasing ventilation in the ipsilateral lung [14]. This is thought to be associated with an improved environment for post-natal lung development, though the presence of inadequate perfusion growth may explain some differences in long-term pulmonary function of these children compared to similar age cohorts without CDH [14].
This study has several limitations. First, the limited sample size may prevent us from detecting an association between the presence of a hernia sac and future perfusion scan results. This study also has the potential for selection bias. At our institution perfusion is evaluated at the discretion of the providers in our longitudinal follow-up clinic, and requires parental consent. Children with less severe disease are less likely to undergo perfusion imaging, so a subset of patients with less severe disease are missing from this study population. Finally, perfusion scans measure distribution of the radiotracer in the ipsilateral and contralateral lungs as a proportion of total tracer administered. Patients with CDH, however, are considered to have a global perfusion abnormality, with decreased perfusion to both the ipsilateral and contralateral lung. The true perfusion defects are likely larger than what was observed in this study. This would attenuate the observe relationship between defect area and perfusion defect [2]. The study does however make a first attempt to evaluate the relationship between hernia sacs and future lung perfusion. Additionally, our regression analysis provides some insight into the magnitude and direction of the relationship between hernia defect area and differential perfusion of the two lungs, although this relationship should be further explored with larger sample sizes.
This study suggests evidence of a potential mechanism of impaired pulmonary perfusion observed in CDH patients with larger defects. While no relationship between hernia sacs and pulmonary perfusion was identified, repeating this study with a larger sample may allow for detection of such a relationship. Future research projects include continued enrollment to increase sample size and longitudinal assessment of lung function using perfusion and spirometric indices. Continued investigation of protective and deleterious factors influencing the long term outcomes of CDH is needed in order to allow for better discussions with parents regarding the long term effects of their child's diagnosis, as well as identify modifiable factors that may improve patient outcomes.