Background: Treatment for patients with pulmonary nontuberculous mycobacterial (NTM) disease includes long, multi-drug, and toxic medication regimens. Surgical resection is an alternative treatment for patients with localized or refractory NTM infection. Robot-assisted operations have not been performed routinely in this population.
Methods: A retrospective review was performed on patients with NTM disease that underwent robotic anatomic pulmonary resection at NYU Langone Medical Center between August 2017 and May 2021.
Results: A total of 12 patients underwent 13 operations. The majority of patients were female (92%) and white (83%). Mean age at time of surgery was 61 years. The most common indication for surgery was cavitary disease, followed by failure of medical therapy, and hemoptysis. All patients had pre-operative sputum cultures positive for Mycobacterium avium intracellulare.
67% of patients were on IV antibiotics prior to surgery. Lobectomy was the most common operation performed. There were no post-operative deaths. Three patients had a prolonged air leak (> 5 days). There were no post-operative bleeds requiring transfusion, pneumonias, pneumothoraces, or bronchopleural fistulas. None of the patients required an ICU stay and the median length of hospital stay was 1 day. Ten patients were followed for a median follow-up period of 21 months (range 6-48 months). Seven patients have been followed for over a year and are no longer on antibiotic therapy. The remaining three patients had recent surgeries and have de-escalated their medical regimen and are off IV therapy.
Interpretation: Surgical resection for patients with complex NTM disease can be performed using minimally invasive, robotic techniques safely and without the need for conversion to open thoracotomy, blood transfusions, or ICU stay. In this small cohort of patients, robotic surgery had a high rate of cure, few post-operative complications, and a short length of hospital stay.
Bronchiectasis, Nontuberculous mycobacteria (NTM), Mycobacterium avium intracellulare (MAI), Robotic pulmonary resection, Robotic lobectomy
MAI: Mycobacteria Avium Intracellulare; NTM: Nontuberculous Mycobacteria; NTM-LD: Nontuberculous Mycobacteria Lung Disease; VATS: Video-assisted Thoracoscopic Surgery
The prevalence of nontuberculous mycobacterial disease is increasing in the United States, especially among women and the elderly [1]. There are more than 190 species of nontuberculous mycobacteria (NTM), with the most common being Mycobacterium avium complex [2]. Pulmonary disease occurs in patients with chronic lung disease, such as those with non-cystic fibrosis bronchiectasis or emphysema. Nontuberculous mycobacterial lung disease (NTM-LD) is associated with significant morbidity and mortality, especially in patients with cavitary disease [3].
Current guidelines recommend a multi-drug macrolide-based regimen for a minimum of 12 months after sputum culture conversion [2]. Treatment is challenging due to the long duration of administration, multiple toxicities, and emerging resistance. Despite medical therapy, many patients do not achieve sputum culture conversion and the rate of relapse is high. Sputum culture conversion is often lower in patients with the cavitary form of the disease with a reported rate of 52% compared to 100% in those with nodular disease [4]. The high failure rate may be explained by poor penetration of antibiotics into the diseased lung and resistance due to biofilm formation [5].
It has been suggested that patients with poor response to standard medical therapy may benefit from a combination of anti-mycobacterial drugs and surgical resection. Several single-center retrospective studies that have shown a favorable treatment outcome for patients who have undergone surgery [6-10]. Sputum culture conversion rates have been reported to be as high as 87.5% in patients that underwent surgical resection compared to 45.8% in matched controls [11]. Though the data has been promising, there are no consensus guidelines for which patients should be considered for surgery.
Mitchell, et al. reported on the largest cohort to date with a total of 236 patients who had surgical intervention for NTM disease. This group included patients that underwent open thoracotomy or video-assisted thoracoscopic surgery (VATS) for pulmonary resection. The average length of stay was 6.5 days, morbidity rate was 18.5%, and the overall mortality rate was 2.6% [7]. Data on sputum culture conversion was not included. Overall, it showed positive results with an acceptable, though not insignificant, rate of morbidity. Kang and colleagues evaluated the surgical outcomes of 70 patients with NTM-LD, they reported one post-operative mortality and a complication rate of 21% [12]. Though the complication rate was relatively high, 81% of patients achieved sputum culture conversion.
With advances in surgical techniques, less invasive approaches are now preferred over the traditional open thoracotomy. In a recent report, VATS accounted for 65% of operations and was associated with a lower rate of adverse events [6]. Robotic surgery has gained popularity in recent years, especially in patients that undergo surgical resection for lung cancer. Recent data shows robotic-assisted lobectomies may have shorter operating times and a decreased hospital length of stay compared to VATS in selected centers. Additionally, the robotic surgery cohort had less post-operative complications compared to open-thoracotomy group [13]. Robotic surgery has not been used routinely for patients with NTM-LD. To date there have been no published studies on the safety or efficacy of robotic surgery for this population. This report presents our single surgeon, single center experience with robot-assisted pulmonary resection in patients with NTM-LD.
A retrospective chart review was performed on the medical records of 13 patients who underwent anatomical lung resection for NTM at New York University Langone Health between August 2017 and May 2021. All operations were performed by a single, experienced surgeon. This study was approved by the Institutional Review Board of NYU Langone Health. Patient consent was waived as patient identification was not required for the present study.
Demographic data including patient age, sex, BMI, smoking status, and medical co-morbidities were included. Information on pre-operative antibiotic therapy, microbiologic data, surgical characteristics, and major and minor surgical complications was collected.
Patients were included if they had robotic surgery for NTM and met the criteria for NTM-LD based on the 2020 American Thoracic Society (ATS)/Infectious Disease Society of America (IDSA) guidelines [2]. Patients were considered for surgical intervention if they had failure of medical therapy, massive or recurrent hemoptysis, or cavitary disease. Failure of medical therapy was defined as persistently positive sputum cultures after 6 months of therapy, progression of disease despite appropriate antibiotics, or inability to tolerate medications. All patients had evidence of irreversible lung destruction amenable to surgical resection, such as focal bronchiectasis or cavitary disease (Figure 1 and Figure 2). A consensus decision was made between the patient's primary pulmonologist and the thoracic surgeon. Standard pre-operative work-up included high-resolution chest computed tomography, baseline pulmonary function testing, and evaluation of sputum cultures with sensitivity testing.
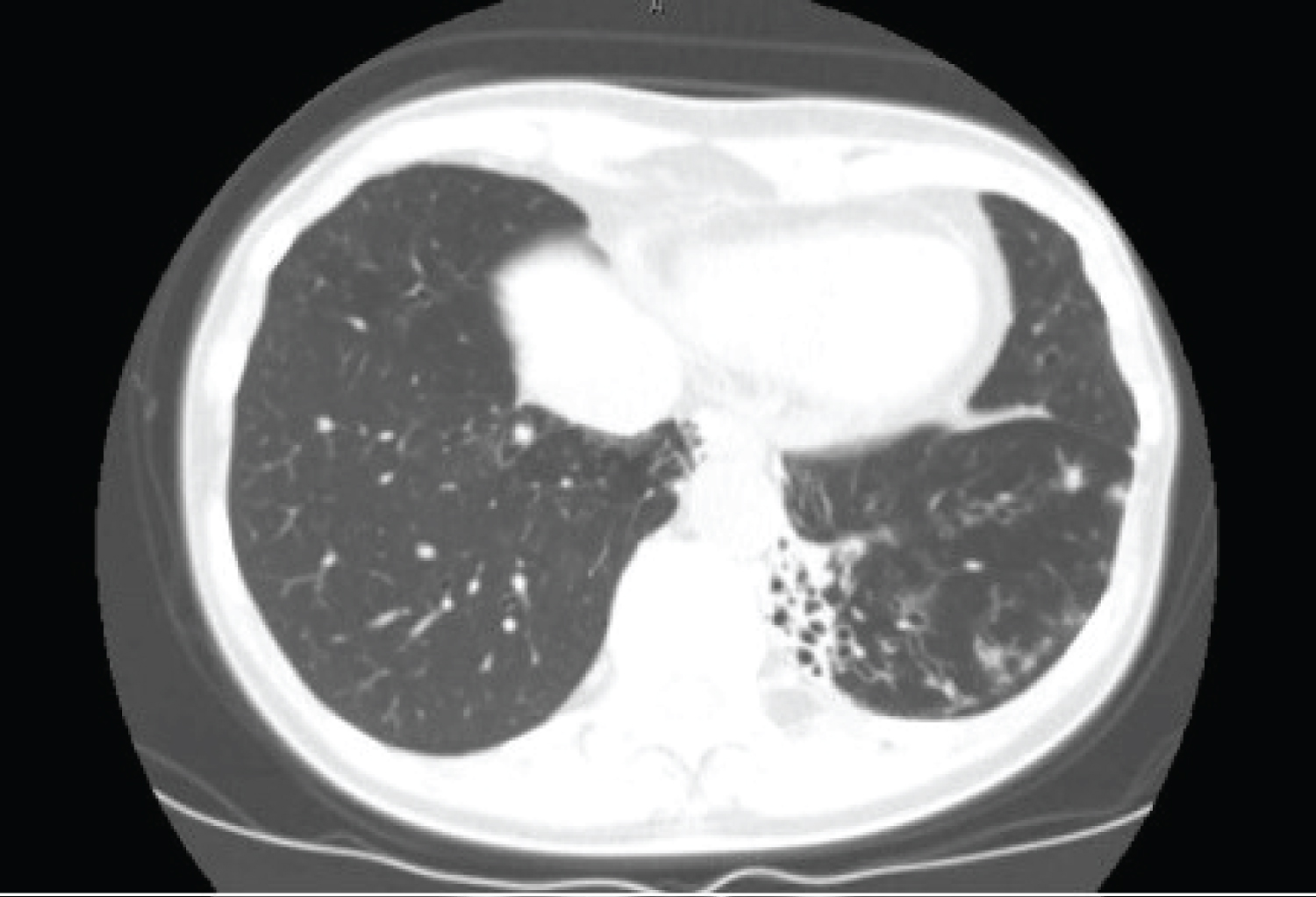 Figure 1: Computed tomography scan of the chest showing focal bronchiectasis in the left lower lobe in a patient with Mycobacterium avium intracellulare. View Figure 1
Figure 1: Computed tomography scan of the chest showing focal bronchiectasis in the left lower lobe in a patient with Mycobacterium avium intracellulare. View Figure 1
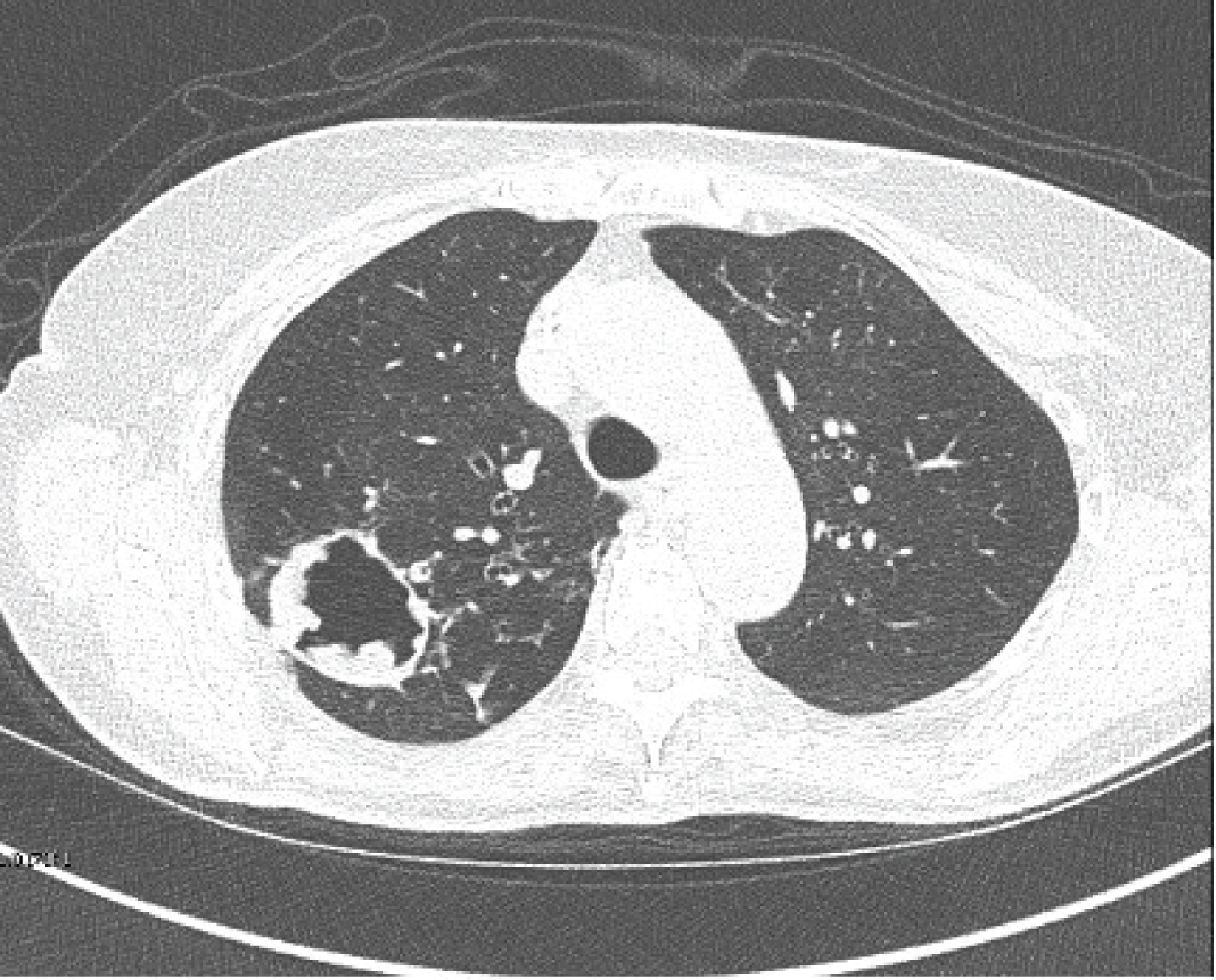 Figure 2: Computed tomography scan of the chest demonstrating a large cavity in the right upper lobe in a patient with Mycobacterium avium intracellulare. View Figure 2
Figure 2: Computed tomography scan of the chest demonstrating a large cavity in the right upper lobe in a patient with Mycobacterium avium intracellulare. View Figure 2
All patients were continued on their multi-drug antibiotic regimen after surgery. Patients that were on intravenous (IV) antibiotics remained on IV antibiotics for at least one month after the operation. Routine post-operative care including early mobilization, pain control, and pulmonary toilet was completed. All patients had chest tubes placed at the time of surgery. Chest tubes were removed prior to hospital discharge or at a follow-up telemedicine visit with the surgeon.
A total of 13 operations were performed in 12 patients from August 2017 to May 2021 (Table 1). The mean age at time of surgery was 61.6 years (range 43 to 74 years). The majority of patients were female (92%) and white (83%). The mean BMI was 21.6 kg/m2. Only one patient had prior thoracic surgery. The patients were mostly non-smokers (83%) and the most common co-morbidity reported was gastroesophageal reflux disease (58%). One patient was on immunosuppression for history of rheumatoid arthritis.
Table 1: Demographics. View Table 1
All the patients had sputum positive for macrolide sensitive Mycobacterium avium-intracellulare (MAI). The most common indication for surgical resection was cavitary disease (58%), followed by failure of medical therapy (25%), and recurrent hemoptysis (16%). All patients were treated with standard guideline-based therapy for MAI unless they developed a toxicity to standard drugs [2]. 67% of patients were on IV antibiotics prior to surgery. The duration of anti-mycobacterial prior treatment ranged from 1 month-4 years. The pre-operative anti- mycobacterial regimen at the time of surgery is listed in Table 2.
Table 2: Pre-operative antibiotics. View Table 2
All surgeries were performed robotically by the same surgeon and lobectomy was the most common operation performed. One patient had a bilateral, staged procedure. The type of resection performed is listed in Table 3. None of the operations had to be converted to open thoracotomy. The median operative time was 98 minutes (range 45 to 221 minutes) and the median intraoperative blood loss was 10 mL (range 7 to 50 mL). The median hospital length of stay was 1 day (range 1 to 5 days).
Table 3: Type of surgical resection. View Table 3
The surgical outcomes are detailed in Table 4. There were no intraoperative or post-operative mortalities. Three patients had a prolonged air leak, defined as air leak greater than 5 days. All patients that developed a prolonged air leak had cavitary disease. These patients were all discharged from the hospital with chest tubes in place attached to a digital air leak system and had daily telemedicine visits with the surgeon. Two of these patients had their chest tubes removed on post-operative day 8 and day 14 and had a small fixed pleural space deficit that did not require intervention. One patient had a chest tube removed on post-operative day 8 and had no further sequelae. There was no operative morbidity, 30 or 90-day operative mortality, or re- admissions. There were no post-operative pneumonias or infections requiring antibiotic therapy.
Table 4: Surgical outcomes. View Table 4
Ten patients have followed longitudinally at our institution for a median follow-up period of 21 months (range 6-48 months). Two patients were lost to follow-up. A favorable outcome was defined as sputum culture conversion or de-escalation of the medical regimen. All 10 patients have had a favorable outcome.
Seven patients have been followed more than a year post surgery, six of these patients have been off all antibiotics therapy. Three out of the seven patients had sputum culture conversion, defined as three negative sputum cultures. An additional two had at least two negative sputum cultures. These patients were unable to give an additional sample due to inability to produce sputum even with induction. Bronchoscopy was not felt to be warranted to confirm sputum culture conversion as patients had significant clinical improvement. The patient that remains on antibiotics is on a suppressive three times weekly regimen due to history of immunosuppression.
The three patients that had recent resection and have been followed for a median time of 6 months (range 6-11 months). They have all had de-escalation of their medical regimen. One of these patients has had three negative sputum cultures.
All patients that were treated with IV antibiotics prior to surgery discontinued IV antibiotics in the post-operative period. Most patients discontinued IV antibiotics 1 month after surgery, though one patient continued IV Amikacin for 6 months after surgery.
This report describes our experience with robotic resection for patients with complex NTM-LD. Though this cohort is small, our study demonstrates that robotic surgery can be performed safely with few complications and favorable clinical outcomes. To our knowledge, this is the first published report of robot-assisted surgical resection for patients with NTM-LD.
There were no operative or post-operative mortalities in this study and there was a low rate of morbidity. The only significant complication seen was persistent air leak and fixed pleural space deficit. None of these patients required further intervention and have continued to do well clinically. All patients had either a lobectomy, segmentectomy, or wedge resection compared to older studies where many patients had to undergo larger resections or even pneumonectomy. The minimally invasive approach and ability to resect a smaller portion of the lung contributed to our low complication rate.
In this study, the hospital length of stay was much shorter than previously reported. Mitchell, et al. reported an average length of stay of 6.5 days, however, this group also included patients that underwent open thoracotomy and pneumonectomy [7]. Robotic operations have been shown to have a reduced length of stay compared to both open thoracotomies and VATS [14]. We were able to achieve a shorter length of hospital stay by discharging select patients with chest tubes and a digital air flow leak meter. With close follow-up from the surgeon and frequent telemedicine visits, 84% of our patients were able to leave the hospital within 3 days of the operation.
Regarding clinical outcomes, most patients had a favorable result after robotic resection. All patients had de-escalation of their medical regimen and none of the patients in our cohort remain on IV antibiotics. Three patients met criteria for sputum culture conversion and an additional two had two negative sputum cultures and are considered clinically cured. Further investigation is needed regarding longer term follow-up, specifically to assess the rate of relapse and reinfection.
Our patient population is similar to previous studies with majority female patients with cavitary lung disease. It is important to note that our cohort is a primary MAI group. In general, patients with MAI have better outcomes than patients with rapidly growing NTM infections such as Mycobacterium abscessus. Additionally, all patients had macrolide-sensitive MAI. Most patients with macrolide sensitive MAI can be treated with medical therapy alone, however, surgical resection is an important adjunct for patients with persistent smear positivity, medication intolerance, and the fibrocavitary form of the disease.
The optimal time to perform a surgical intervention for a patient with NTM-LD is unknown. Most of our patients were on antibiotics for months to years without improvement in disease. Those that went to surgery early had significant disease related complications such as hemoptysis. The appropriate timing to perform pulmonary resection in NTM should be explored in future studies.
There were several limitations of this study including a small sample size at a single institution, a homogenous patient population, and all operations were performed by a single, experienced surgeon. More data is needed about the use of robotic surgical resection in the more difficult to treat NTM groups, such as those with rapidly growing nontuberculous mycobacterial infections and those with macrolide resistance. Despite these limitations, this preliminary report demonstrates the benefits of surgical resection with a robotic platform for patients with refractory NTM-LD.
In summary, robotic surgical resection for patient with complex NTM disease is safe and highly efficacious in an experienced medical center. Larger studies are needed to assess further applicability.
EM and RC have no conflicts of interest to report. AB has served as a consultant and on the advisory board for Insmed, Hill-Rom, Zambon, Dymedso and Physio Assist. He also is a principal investigator for a clinical trial funded by Hill-Rom and has received a medical education grant from Insmed. DAH is a principal investigator for clinical trials funded by AN2 Therapeutics, Boehringer Ingelheim, Hill-rom, Insmed, Zambon.
EM and RC have no conflicts of interest to report. AB has served as a consultant and on the advisory board for Insmed, Hill-Rom, Zambon, Dymedso and Physio Assist. He also is a principal investigator for a clinical trial funded by Hill-Rom and has received a medical education grant from Insmed. DAH is a principal investigator for clinical trials funded by AN2 Therapeutics, Boehringer Ingelheim, Hill-rom, Insmed, Zambon.
EM had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any adverse events. AB, RC, and DAH contributed to data analysis and interpretation and the writing of the manuscript.