Introduction: Appendiceal Mucocele is a rare medical condition, sometimes it is discovered incidentally but occasionally it could mimic acute appendicitis. Laparoscopic resection of appendiceal mucocele recently has been reported, but the safety and efficacy are still controversial.
Presentation of cases: We will present four cases of laparoscopic resection of appediceal mucocele. The First, second, and fourth cases were treated by laparoscopic appendectomy only; While the third case was treated by laparoscopic right hemicolectomy.
Discussion: We elected to do our cases using a Laparoscopic approach. Laparoscopic resection is achievable with expert surgeons, despite the risk of malignancy, but necessary precautions should be taken. The four cases' final histopathology reports showed the same result: Low-Grade Appendiceal Mucinous Neoplasm (LAMN).
Conclusion: A Laparoscopic resection of appendiceal mucocele can be done by expert surgeons if the necessary precautions were taken to prevent spillage.
Mucocele, Appendix, Laparoscopy, Appendectomy, Right hemicolectomy, Minimally invasive, Low Grade Appendiceal Mucinous Neoplasm (LAMN)
Appendiceal Mucocele is a condition where luminal distention occurs due to mucin accumulation within the appendiceal lumen. This condition usually results from either benign epithelial proliferation such as; hyperplasia and Lowe-Grade Mucinous Neoplasm or malignant epithelial proliferation such as: Mucinous cystadenocarcinoma [1].
The most common mucinous neoplasm of the appendix is Mucinous cystadenoma the new terminology is Low-Grade Mucinous Neoplasm. The standard therapy is surgical resection due to the difficulty in determining whether
it’s benign or malignant in addition to the risk of rupture that may cause pseudomyxoma peritonei in both conditions. The ideal way for resection is either Appendectomy or Partial Cecectomy of appendiceal mucocele or even ends with right hemicolectomy [2,3].
Traditionally, resection is recommended for mucoceles, as imaging cannot predict the malignancy rate of mucoceles. However, resection must be done with caution, as the rupture can lead to pseudomyxoma peritonei or deposition of mucin within the peritoneal cavity. These conditions can result in significant morbidity due to mucinous ascites and bowel obstruction. Laparoscopic surgery for appendiceal tumors is still controversial, as inadvertent rupture of the lesion could happen due to improper handling, which will cause pseudomyxoma peritonei [3].
In our cases, we will present our center experience in Laparoscopic approach for resection of Appendicular Mucocele.
A 51-years-old female is known to have Hypertension, hypothyroidism, and asthma. Presented to the clinic with lower abdominal pain and right flank pain for 20 days. Physical examination was significant only for diffuse abdominal tenderness without peritoneal signs. Laboratory tests including complete blood count, and biochemical analysis of the biliary and urinary systems were all normal. Abdominal CT-Scan with IV contrast showed: Distended fluid containing appendix with no significant inflammatory change and few small local nodes with a Highly Possibility of mucocele (Figure 1). We did a full colonoscopy and CEA to rule out the underlying appendiceal mucocele and other concomitant malignancies. Colonoscopy revealed: No caecum pathology, CEA test was within normal range. After a discussion with the patient, we took her for a diagnostic laparoscopy and according to the intraperitoneal findings, we did an appendectomy instead of ileocecal resection.
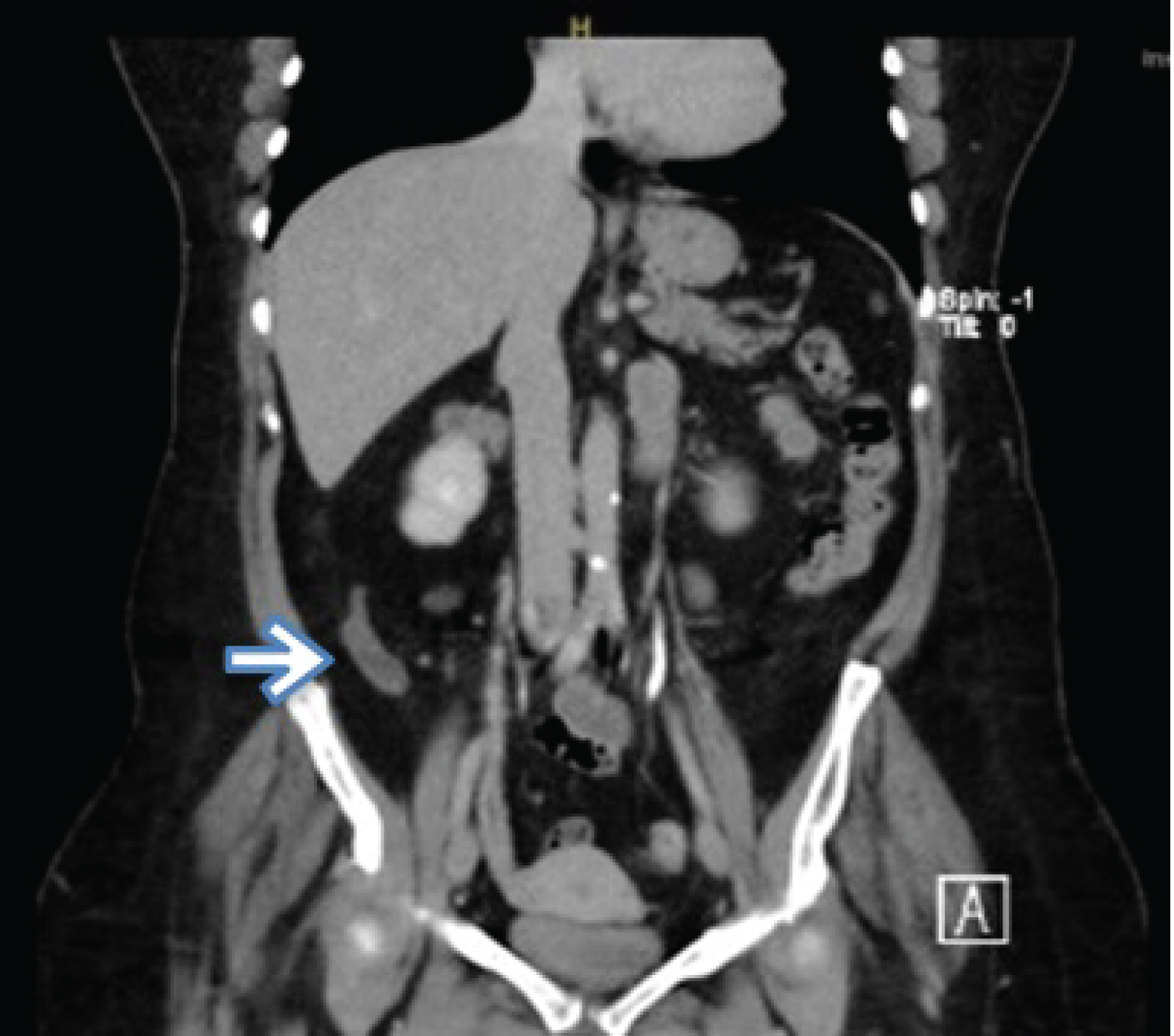 Figure 1: Coronal CT appearance of mucocele of the appendix.
View Figure 1
Figure 1: Coronal CT appearance of mucocele of the appendix.
View Figure 1
Intra-operative approach and findings: A 12-mm trocar was placed through the supra-umbilical incision to approach the intraperitoneal cavity using the open Hasson technique. A pneumoperitoneum was made by the insufflation of carbon dioxide. The table was kept in Trendelenburg position with a 15° left tilt. A 30° telescope was introduced through the umbilical port for diagnostic laparoscopy, and complete abdominal examinations were done. Diagnostic laparoscopy revealed approximately 2 cm large mucocele of the appendix with omental adhesions. The ovary, fallopian tube, and uterus were all normal looking.
Two 5-mm ports were placed in the right upper quadrant and the left lower quadrant (Figure 2). The appendiceal mucocele was isolated after separating the mesoappendix with the help of bipolar cautery (ligasure). Following this, the base of the appendix was ligated at the ileocecal junction and divided by using an endoscopic stapling device (Multifire Endo GIA, 60 mm) which was used to perform the partial resection of cecum. Mucocele of the appendix was retrieved in a plastic bag through the umbilical port after careful minimal handling. Hemostasis was obtained. The umbilicalport site wound was closed with 1.0 Vicryl endoclose. The Patient tolerated the procedure, she started oral feeding 6 hours post-operation and solid food on the next day. She was discharged on the third postoperative day without active complaint. Pathology showed a Low-Grade Appendiceal Mucinous Neoplasm (LAMN), negative margins, and no invasive component. The patient was refered to the oncology clinic for surveillance, One year follow-up with CT showed normal CT.
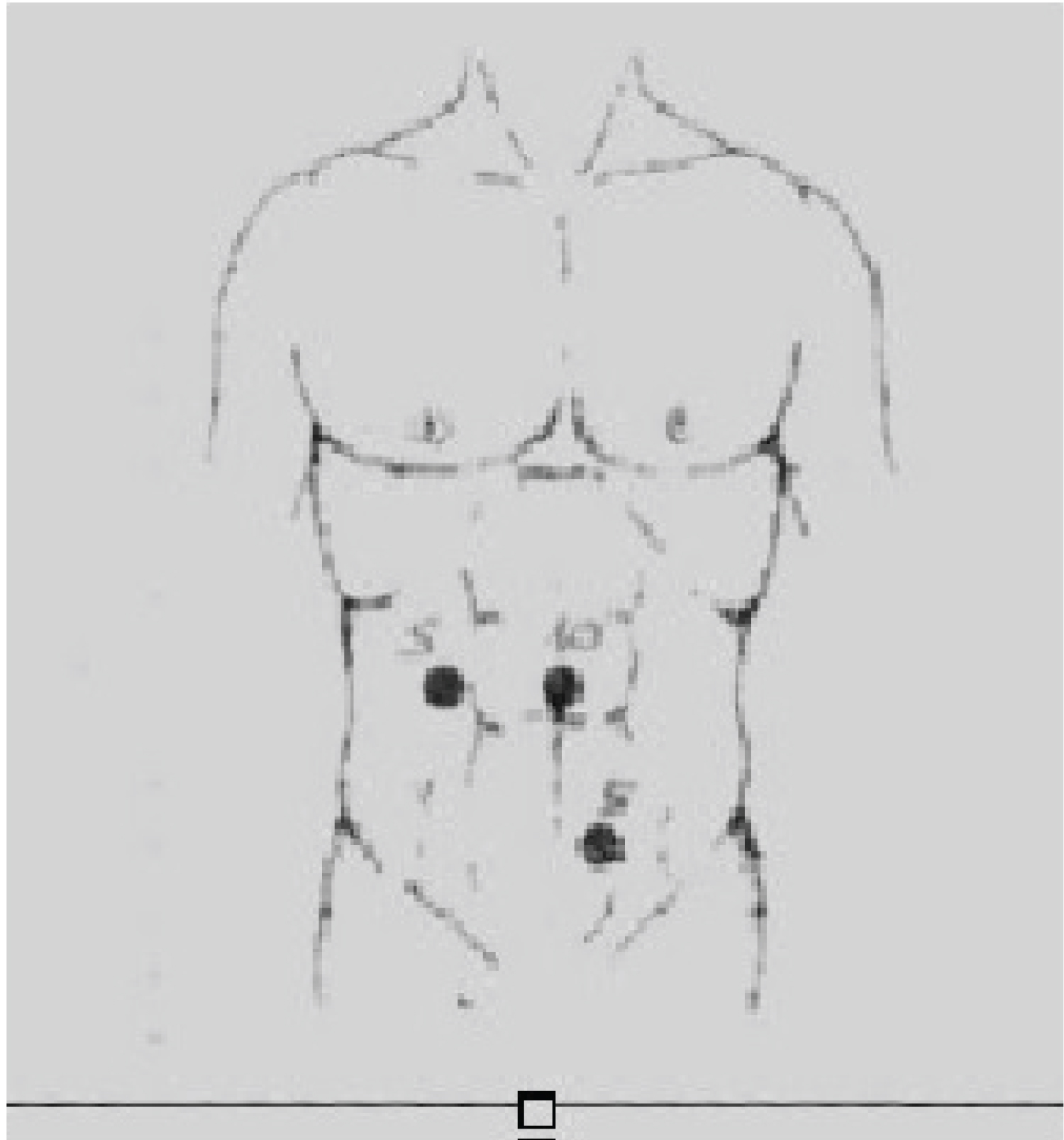 Figure 2: Trocars sites for laparoscopic resection of an appendiceal mucocele.
View Figure 2
Figure 2: Trocars sites for laparoscopic resection of an appendiceal mucocele.
View Figure 2
A 37-years-old Male medically free, presented to ED complaining of lower abdominal pain associated with nausea and vomiting for 1 Day, Abdominal CT scan was done and showed dilated appendix that is reaching 1.6 cm in maximal diameter and contained multiple calcifications with mild surrounding fatty stranding. Impression of acute non-complicated appendicitis with the possibility of coexistent appendiceal mucocele (Figure 3). After a discussion with the patient, we took him for a diagnostic laparoscopy and according to the intraperitoneal findings, we did an appendectomy instead of ileocecal resection.
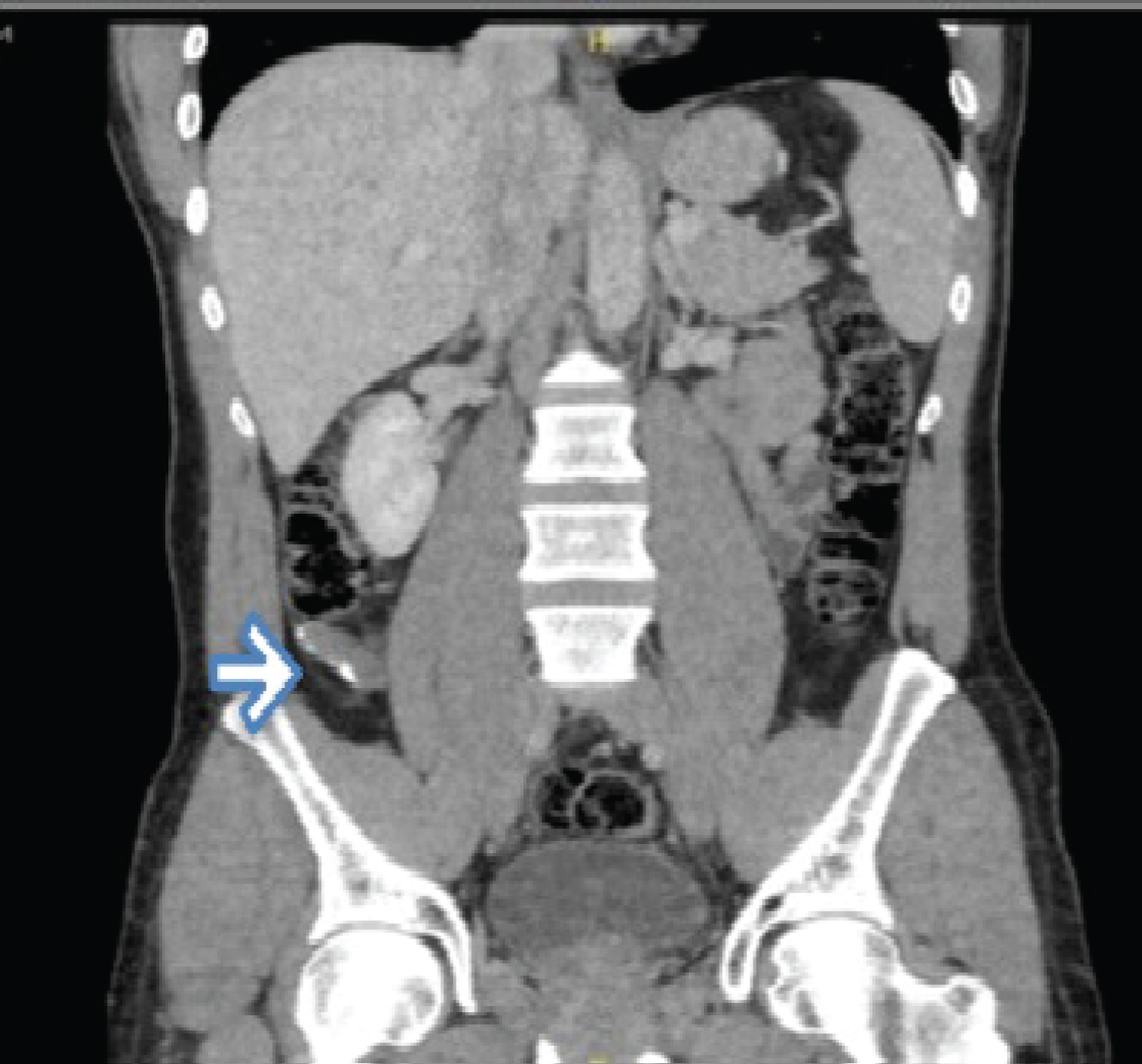 Figure 3: Coronal CT appearance of appendiceal mucocele with calcification.
View Figure 3
Figure 3: Coronal CT appearance of appendiceal mucocele with calcification.
View Figure 3
Intra-operative approach and findings: Because of the similarity in the laparoscopic procedure for the both first and second cases, only the first case was presented in detail. Intraoperative findings showed no evidence of intraperitoneal mucin deposition. The Laparoscopic approach allowed the meticulous dissection of the Appendix and clear identification of the base of the appendix without manipulating the appendiceal mucocele itself; also, the appendix was secured at the base. The specimen was intact with no spillage of mucin during the operation. The patient has discharged two days post-operation in a good condition without active complaint. Histopathological evaluation of the appendiceal mucocele was reported as a Low-Grade Appendiceal Mucinous Neoplasm (LAMN) (Figure 4A and Figure 4B). After that, the patient was referred to the oncology clinic and planned for surveillance follow-up after 6 months.
 Figure 4a: Hematoxylin and eosin stain (100x) The appendix lumen was distended by mucin (asterisks), fibrin and scattered calcified material.
View Figure 4a
Figure 4a: Hematoxylin and eosin stain (100x) The appendix lumen was distended by mucin (asterisks), fibrin and scattered calcified material.
View Figure 4a
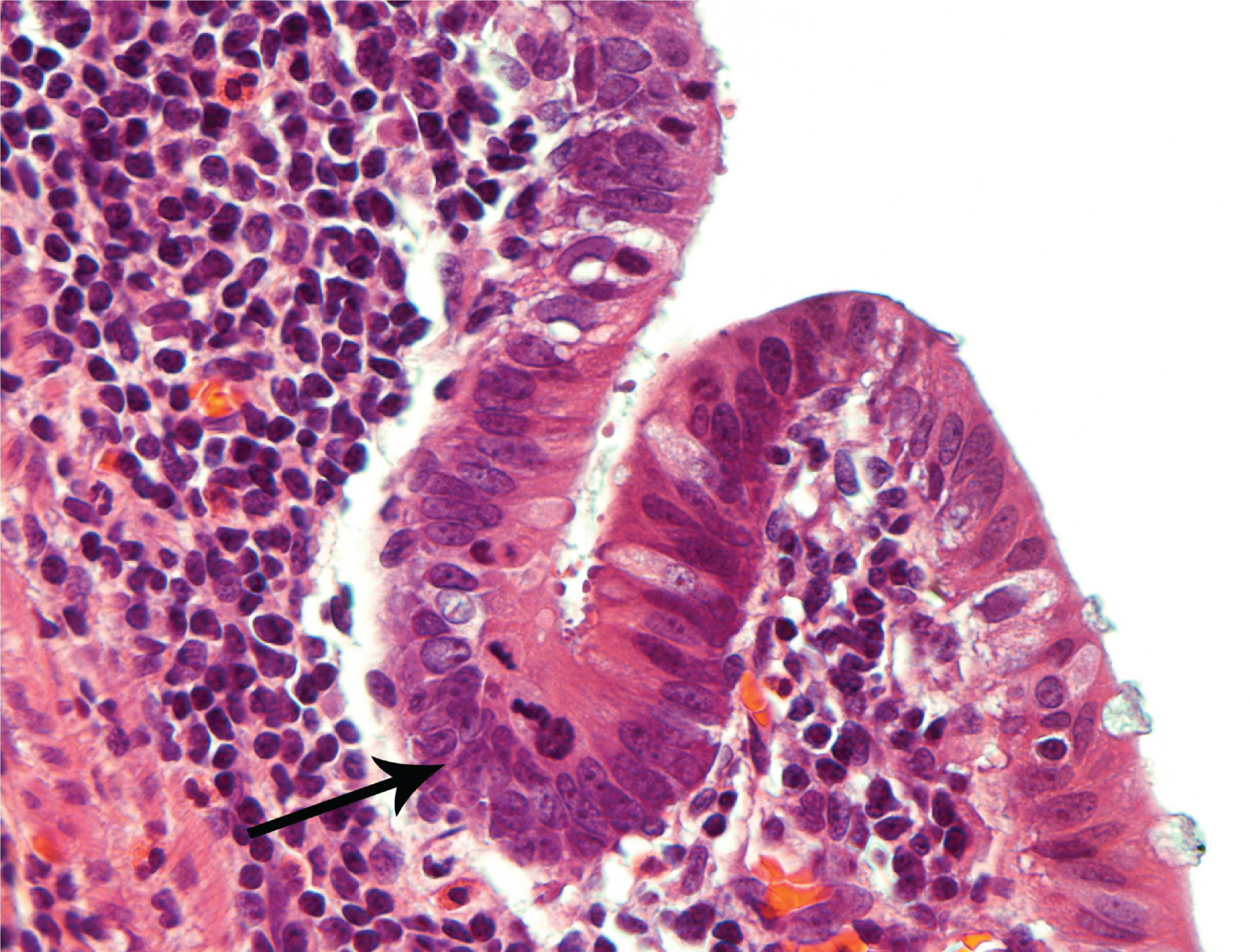 Figure 4b: Hematoxylin and eosin stain (400x) High power view showing an intact dysplastic epithelial lining (arrow). The cells nuclei appear elongated and crowded with adjacent mitoses at the apical border.
View Figure 4b
Figure 4b: Hematoxylin and eosin stain (400x) High power view showing an intact dysplastic epithelial lining (arrow). The cells nuclei appear elongated and crowded with adjacent mitoses at the apical border.
View Figure 4b
A 38-years-old male medically free, presented to the general surgery clinic complaining of vague abdominal pain, bilateral inguinal swelling, and pain. Moreover, the patient had a history of open left inguinal hernia repair with mesh placement 2 years prior to presentation. An abdominal CT scan with contrast was done which revealed an incidental finding of a large fluid-distended tubular lesion approximately measuring 13.2 cm in length, that extended from the right iliac fossa to retro cecal paracolic region. It is having flecks of calcification in the inferior aspect with mild thickening of the wall (Figure 5). We did a full colonoscopy, CEA to rule out the underlying concomitant disease or malignancies. Colonoscopy revealed: no caecum pathology, CEA test was within normal range. A Chest CT scan was done to rule out any metastasis, which was unremarkable. We took the patient for a diagnostic laparoscopy and proceeded with a right hemicolectomy based on the intraperitoneal findings.
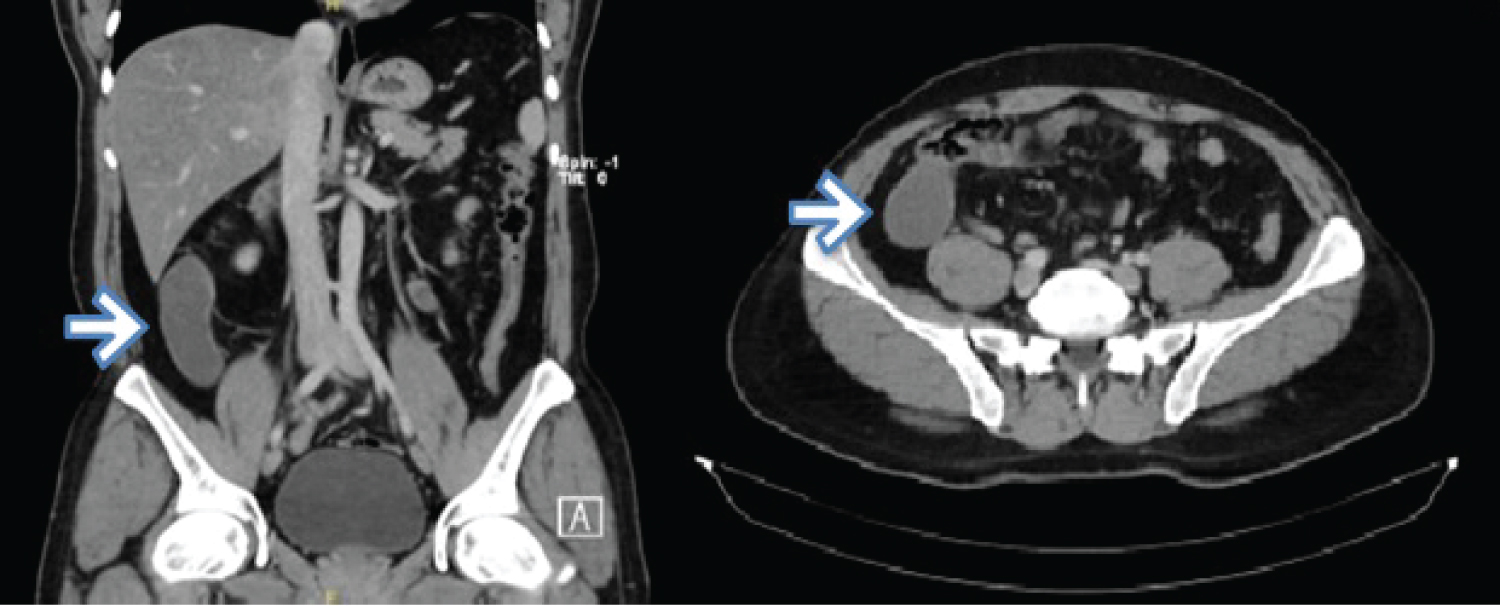 Figure 5: Axial, coronal CT appearance of mucocele of the appendix.
View Figure 5
Figure 5: Axial, coronal CT appearance of mucocele of the appendix.
View Figure 5
Intra-operative approach and findings: A 12-mm trocar was placed through the umbilical incision to approach the intraperitoneal cavity using the open Hasson technique. A pneumoperitoneum was made by the insufflation of carbon dioxide. The table was kept in Trendelenburg position with a 15° left tilt. A 30° telescope was introduced through the umbilical port for diagnostic laparoscopy which revealed an approximately 13 cm large mucocele of the appendix. Due to the large size of the mucocele and to prevent any spillage, we decided to proceed with a right hemicolectomy. Three 5-mm ports were placed in the right upper quadrant, left lower quadrant, and subxiphoid area. Lateral to medial approach for mobilization of ascending colon was done by using ligasure. The right ureter was identified and protected then medial to lateral mobilization was done, the duodenum was identified and protected, and the ileocolic vessel was isolated and taken using a Tan load of GIA 60 mm. The hepatic flexure was mobilized as well. Making a midline incision as an extension to the previous umbilical incision, the specimen was carefully extracted through the umbilical incision using the wound protector device, and the ileum and transverse colon were transected using purple load (Multifire Endo GIA, 60 mm) and rest of the mesentery was taken with ligasure, a specimen was taken out and sent for pathology (Figure 6A and Figure 6B). A side-to-side anastomosis using 2 loads of (Multifire Endo GIA, 60 mm) was done. The anastomosis was wide and tension free, the midline incision was closed using 2-loop PDS, and hemostasis was obtained.
 Figure 6a: Hemicolectomy specimens showing the appendix communicating with caecum and ascending colon.
View Figure 6a
Figure 6a: Hemicolectomy specimens showing the appendix communicating with caecum and ascending colon.
View Figure 6a
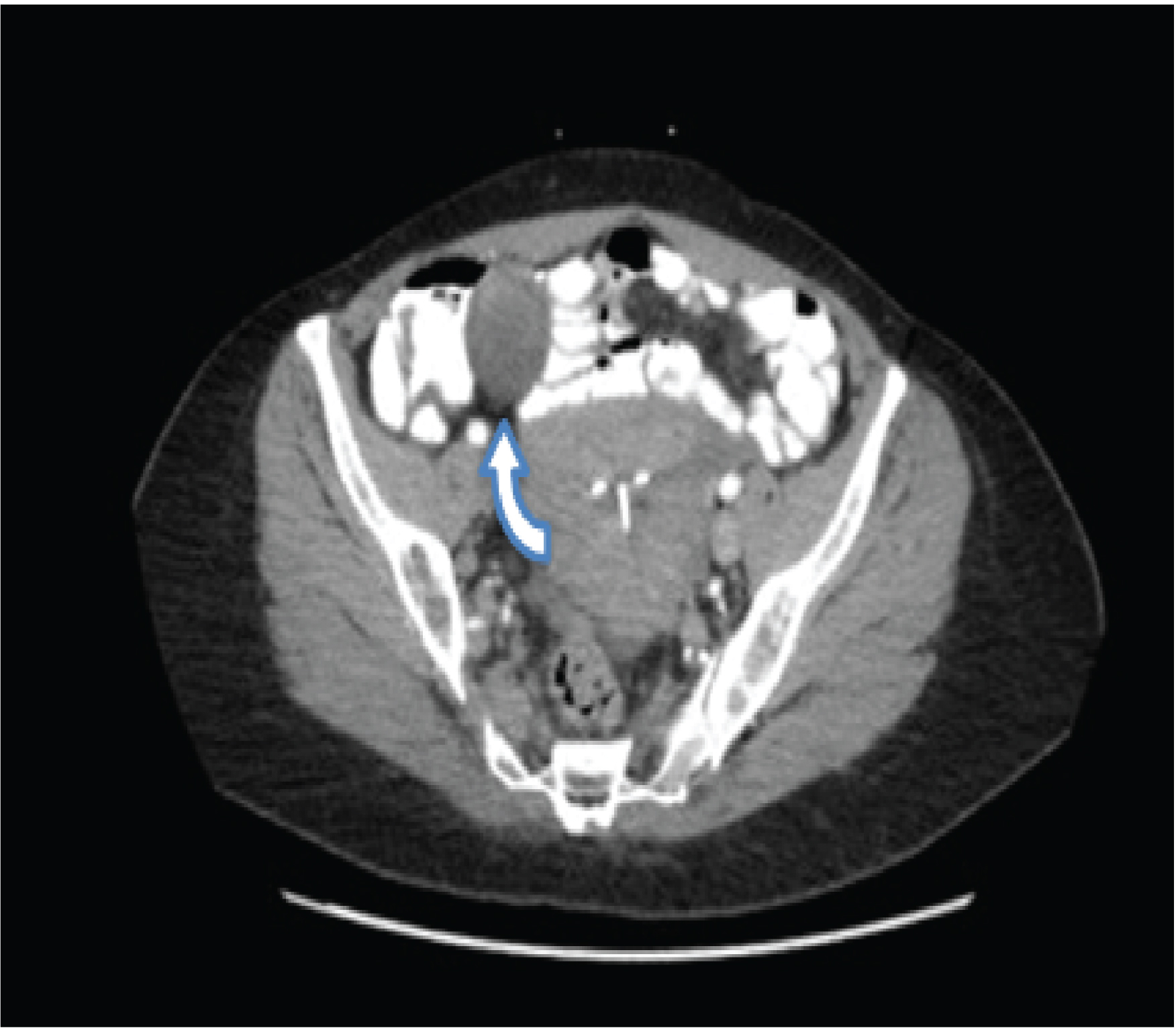 Figure 6b: Axial CT appearance of mucocele of the appendix.
View Figure 6b
Figure 6b: Axial CT appearance of mucocele of the appendix.
View Figure 6b
The patient tolerated the procedure, the patient was discharged on the third postoperative day with- out active complaint. Pathology showed a Low-Grade Appendiceal Mucinous Neoplasm (LAMN) with negative margins and no invasive component. The patient was referred to the oncology clinic for surveillance and Planned for CT scan surveillance after 6 months.
A 41-years-old female known to have Iron deficiency anemia, presented to the Emergency department with recurrent lower abdominal pain. Physical examination was significant only for right lower quadrant tenderness without peritoneal signs. Laboratory tests including complete blood count and urinary system were all within normal ranges. Abdominal CT scan with IV contrast revealed a large elongated fluid-filled tubular structure in the right iliac fossa measuring about 7 cm and arising from the inferior-medial aspect of the cecum with focal calcification, the appearance was highly suggestive of appendiceal mucocele no other masses were seen (Figure 6A and Figure 6B). We did a full colonoscopy, and CEA to rule out underlying appendiceal mucocele, and other concomitant malignancies. Colonoscopy revealed: No cecum pathology, CEA test was within normal range. After a discussion with the patient, we took her for a diagnostic laparoscopy and according to the intraperitoneal findings, we did an appendectomy instead of ileocecal resection.
Intra-operative approach and findings: A 12-mm trocar was placed through the supra-umbilical incision to approach the intraperitoneal cavity using the open Hasson technique. A pneumoperitoneum was made by the insufflation of carbon dioxide. The table was kept in the Trendelenburg position with a 15° left tilt. A 30° telescope was introduced through the umbilical port for diagnostic laparoscopy, and a complete abdominal examination was done. Diagnostic laparoscopy revealed approximately 8 cm large appendiceal mucocele. Two 5-mm ports were placed in the suprapubic and left lower quadrant areas. The appendiceal mucocele was isolated after separating the mesoappendix by Bovie, following this, the base of the appendix was ligated at the ileocecal junction and divided by using an endoscopic stapling device (Multifire Endo GIA, 60 mm) which was used to perform the partial resection of the cecum. Mucocele of the appendix was retrieved in a plastic bag through the umbilical port after careful minimal handling, hemostasis was obtained and the umbilical port site wound was closed.
The patient tolerated the procedure very well, she started oral feeding 6 hours post-operation. She was discharged on the second postoperative day without any active complaint. Pathology showed a Low-Grade Appendiceal Mucinous Neoplasm (LAMN), negative margins, and no invasive component. The patient was referred to the oncology clinic for surveillance, and a two-year follow-up with CT showed normal CT.
There are few reports of Laparoscopic resection of an appendiceal mucocele, none have been published in Saudi Arabia as a case series. In this report, we present four patients with appendiceal mucoceles, two of them were identified incidentally while the other two presented as lower abdominal pain. The four presented cases are different in both presentation and treatment. The first, second, and fourth cases were treated by laparoscopic appendectomy only; while the third case was treated by laparoscopic right hemicolectomy instead of ileocecal resection according to the intra-operative finding of large mucocele which is difficult to resect and obtain negative margins; also, to prevent the spillage. The four cases’ final histopathology reports showed the same result: Low-Grade Appendiceal mucinous neoplasm (LAMN). Appendiceal mucocele does not have a typical clinical picture, more than two-thirds of the patients have their appendiceal mucocele removed based on incidental findings [4]. Clinically, it can remain asymptomatic or manifest with chronic abdominal pain which is the most common clinical feature, as in our first and third cases. Undoubtedly, this condition is less likely to occur in young patients, but always malignancy should be considered as a differential diagnosis. Preoperative diagnostic methods should be done to avoid inappropriate treatment. US abdomen, computed tomography (CT), and colonoscopy are used for diagnostics. US is the first-line diagnostic method for patients with acute abdominal pain. Ultrasound can be used to differentiate between mucocele and acute appendicitis. However, CT abdomen is regarded as the most accurate method of diagnostics. CT can be used to discover the signs specific to mucocele with high accuracy and sensitivity [5,6].
Mucoceles represent a variety of histopathology, both neoplastic and non-neoplastic can result in appendicular dilatation filled with mucus. Historically, mucoceles were categorized into four different types; Benign types of mucoceles include mucosal hyperplasia or a simple cyst secondary to obstruction by a fecalith or stricture. While, neoplastic types include mucinous low-grade neoplasm, which is noninvasive, and mucinous cystadenocarcinoma, which is malignant [3]. Appendiceal neoplasias are pervasive in approximately only 0.4% to 1% of all the tumors of the gastrointestinal tract [2,7], of all these excised appendiceal specimens, 0.7% to 1.7% is the incidence rate of appendiceal tumors discovered incidentally as a result of the respective histopathological analysis, Neoplastic appendiceal mucinous lesions These lesions include serrated polyps (which are hyperplastic lesions with a unique architecture, with or without dysplasia), hyperplastic polyps, low-grade appendiceal mucinous neoplasms (LAMNs), high-grade appendiceal mucinous neoplasms (HAMNs), and mucinous adenocarcinomas.
In literature, laparoscopy has been considered a relative contraindication for the surgical treatment of appendiceal mucoceles. This is due to reports of patients who underwent a laparoscopic appendectomy for intact mucoceles and later developed peritoneal implants, suggesting that maintaining the integrity of the wall of the mucocele is challenging [8]. In addition, some authors have recommended laparotomy over laparoscopy for better exploration of the abdomen for mucin deposits [9]. However, several case reports and some small case series have done laparoscopy for appendiceal mucoceles without intraoperative rupture of the mucocele [10]. Hence, we elected to do our cases using a Laparoscopic approach. Laparoscopic resection is achievable with expert surgeons, regardless of the risk of malignancy, but necessary precautions should be taken.
Indicators of mucocele, such as an appendix lumen larger than 1.3 cm, calcification of the appendix wall, and cystic dilatation, can be detected on CT scans [11]. Mucoceles that are not ruptured do not constitute a hazard to the patient, which is one of the fundamental concepts of surgical therapy for this condition.
As Pseudomyxoma peritonei can develop if it ruptures in the peritoneal cavity and that filling is dispersed throughout the cavity. Treatment for this condition is extremely difficult, and long-term outcomes are bad, with a high death rate [12]. A few surgeons believe that open surgery must be preferred over laparoscopic surgery in most cases. However, we presented here our center's experience of Minimally Invasive Surgery for the Resection of Appendiceal Mucocele.
The term “pseudomyxoma peritonei” is used for the presence of mucinous deposits in the peritoneal cavity secondary to a mucinous neoplasm and can have low-grade, high-grade, or signet ring cell histological features [9]. The patients may require a variety of surgical procedures from appendectomy to right colectomy, and sometimes heated intraperitoneal chemotherapy, cytoreductive surgery during the operation, and early postoperative intraperitoneal chemotherapy if pseudoyxoma peritonei develops [13]. The authors are also aware of the possibility of rupture during laparoscopic dissection and the subsequent fatal complication of pseudomyxoma peritonei. Nevertheless, if we can handle the tissue with minimal manipulation, and can secure enough safety by using various laparoscopic instruments, laparoscopic resection of an appendiceal mucocele might be an alternative surgical option to open surgery. An appendectomy is used for simple mucoceles or cystadenomas when the appendiceal base is intact. Cecal resection is in- indicated for cystadenomas with a large base, and a right hemicolectomy is recommended for cystadenocarcinomas. The 10-year survival of patients with mucinous cystadenocarcinomas is 65% among patients treated by hemicolectomy, but only 37% among patients treated by appendectomy alone [14]. Hence, we elected to do our cases using a Laparoscopic approach. Laparoscopic resection is achievable with expert surgeons, regardless of the risk of malignancy, but necessary precautions should be taken. Also, There was no peritoneal discharge or deposits in any of our cases with mucocele.
In conclusion, appendiceal mucocele is a nonspecific term that encompasses a range of diagnoses, including neoplastic and non-neoplastic causes of appendiceal dilation and mucin production. Resection is recommended for mucoceles due to their potential risk of malignancy. It is imperative to maintain the integrity of the mucocele wall to prevent the risk of pseudomyxoma peritonei. Although laparoscopy has traditionally been considered a relative contraindication for appendectomy for mucoceles due to the risk of perforation, a Laparoscopic resection of appendiceal mucocele can be done by expert surgeons if the necessary precautions to prevent spillage are taken.
No conflicts of interest.
No funding.
Ethical considerations for this study were reviewed and approved by the Dr. Sulaiman Al Habib Medical Group Institutional Review Board (IRB), with log no. [RC23.04.01]. The study was granted exemption from full IRB review, as it met the criteria for exempt research. The exemption was granted due to the retrospective nature of the study, the use of existing de-identified data, and the absence of direct patient interaction. Nonetheless, all data were handled with strict confidentiality and privacy protections, and the study was conducted in compliance with the principles outlined in the Declaration of Helsinki and Good Clinical Practice guidelines.
Written informed consent was obtained from all patients for this study. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request. The information in this case series are completely de-identified.