Appendiceal Mucocele is a rare disease. Sometimes, it is discovered accidentally and sometimes mimic acute appendicitis. Correct diagnosis before surgery is very crucial for the selection of adequate surgical treatment to avoid Intraoperative and Postoperative complication. Ultrasonography and particularly, computed Tomography should be used extensively for this purpose. If mucocele of the appendix is treated incorrectly Pseudomyxoma peritonei which is characterized by malignant process may develop.
We present a case, which was discovered accidentally while evaluating the patient for another condition. She is a 47-year-old woman, who presented at the surgical out-patient department with clinical features suggestive of chronic cholecystitis, had abdominal ultrasonographic scan which showed Cholelithiasis and a cystic tubular swelling in the right lower abdomen, which was reported as a right adnexal cyst. Open surgery was performed. At the time of surgery, multiple stones (3) in the gall bladder and a cystic mass of the appendix with dimensions 13.0 × 3.5 cm, with thinned walls without perforation were discovered. No discharge was found in the peritoneal cavity. Diagnosis of mucocele of the appendix was suspected. Only appendectomy was performed because no pathologic process was found in the base of the appendix and lymph nodes were not increased in size.
Also had cholecystectomy. Histopathologic diagnosis was retention cyst (Simple appendiceal mucocele). After 4 months, the patient is doing well.
Mucocele, Appendix, Gallbladder, Cholelithiasis, Retention cyst (simple appendiceal mucocele)
Appendiceal mucocele is an obstructive dilatation of the appendiceal lumen caused by intraluminal accumulation of mucoid material. It is a rare disease. The incidence is 0.2% to 0.7% of all appendectomy specimens [1-3]. This transformation is caused by one of four patterns of epithelial proliferation: Retention cyst, mucosal hyperplasia, mucinous cystadenoma and mucinous cystadenocarcinoma [4,5].
This disease does not have a typical clinical picture. Sometimes the patient has pain in the lower right quadrant of the abdomen; therefore a surgeon may mistake it for acute appendicitis. Sometimes it is discovered incidentally while evaluating a patient for another condition as in this case. Acute appendicitis is one of the most common surgical diseases [3,6,7].
It is important to differentiate between these two pathologies before surgery and select adequate surgical tactics. If treated improperly, the mucocele may progress, epithelial cells may escape into the peritoneal cavity and Pseudomyxoma peritonei may develop which has a high mortality [7]. We present the case which was discovered intraoperative.
A 47-year-old woman was referred to the Surgical Outpatient Department. Her complain was pain in the right hypochondrial region, worsen by fatty meal. The pain has been on and off for the past 9 months. No pain in the right lower abdomen. No anorexia. Examination of the abdomen showed mild tenderness in the right hypochondrium. No palpable mass or swelling in the right iliac fossa. Ultrasonography showed multiple stones (3) in the gallbladder and right adnexal cystic swelling. The working diagnosis was symptomatic Cholelithiasis and right ovarian cyst. Open surgery (Laparotomy) was performed. At the time of surgery, thickened gallbladder with multiple stones (3) within it and a cystic mass of the appendix, 13.5 × 3.5 cm, thinned wall, without perforation were discovered Figure 1, Figure 2 and Figure 3.
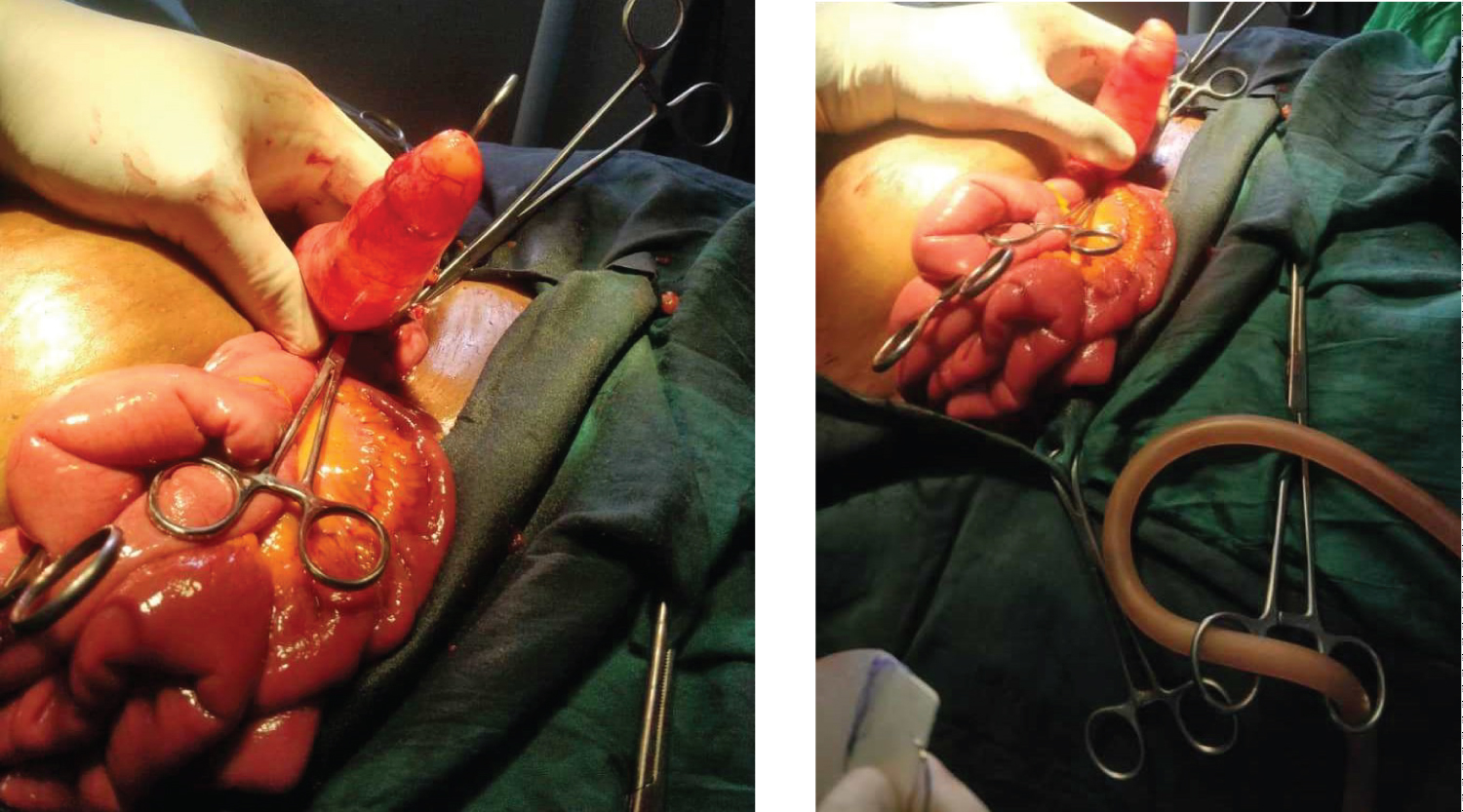 Figure 1 and Figure 2: Intraoperative finding of appendiceal mucocele with normal appendix base.
View Figure 1&2
Figure 1 and Figure 2: Intraoperative finding of appendiceal mucocele with normal appendix base.
View Figure 1&2
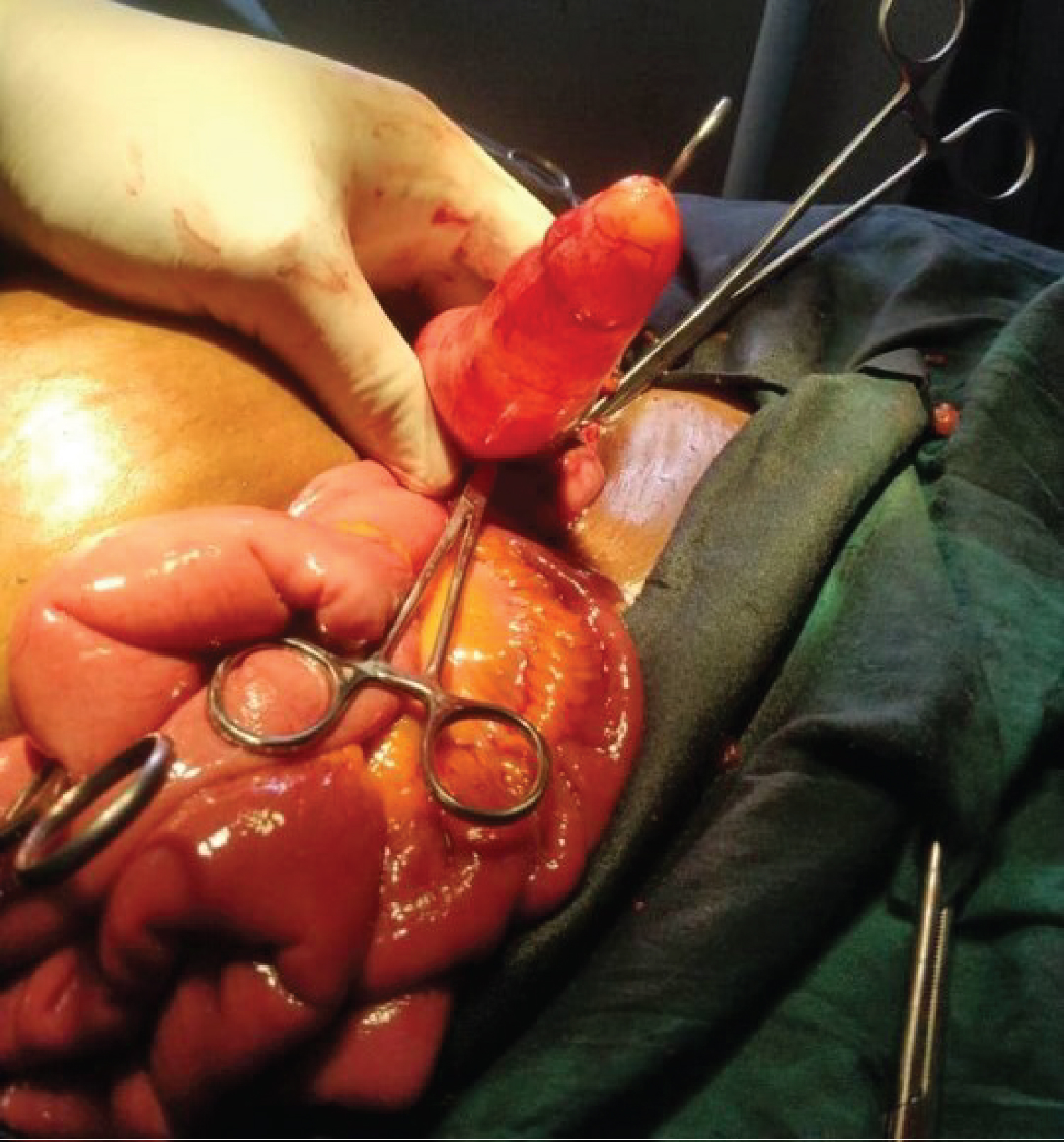 Figure 3: Intraoperative distended appendix with mucin without perforation.
View Figure 3
Figure 3: Intraoperative distended appendix with mucin without perforation.
View Figure 3
The ovaries were normal. No discharge was found in the peritoneal cavity. A mucocele of the appendix was suspected only appendectomy was performed because no pathologic process was found in the base of the appendix. The patient also had cholecystectomy. Histopathologic diagnosis was retention cyst (simple appendiceal mucocele) and chronic cholecystitis. There was no complication in the postoperative period. Four months after Surgery the patient is feeling well.
Mucocele of the appendix was first described by Rokitansky [8]. It is a descriptive and unspecific term to define the cystic dilation of the appendix caused by the accumulation of mucus secretion. This process is slow and gradual, with no signs of infection inside the organ. It results from lumen obstruction in the appendix, which is secondary to the inflammatory or neoplastic proliferation of the appendix mucosa or lesion in the caecum, adjacent to the appendiceal ostium. While some article, confirm its prevalence among women [9,10] other demonstrate a higher incidence among men [11].
Mucocele of the appendix is divided into four pathological subgroups based on the epithelial characteristic [12,13].
The first group consist of a simple retention cyst secondary to occlusion of the appendix by faceolith, scar tissue from previous inflammation or in rare cases due to endometriosis [14]. It has a normal or flattened epithelium, moderate luminal dilation up to 2 cm and it constitutes about 20% of all appendiceal mucocele [14]. The case presented falls under this group. However, it was much larger than expected for this pathologic type. The second group with hyperplastic epithelium and moderate luminal dilatation: This constitutes about 20% of all mucocele of the appendix [14].
The third group is benign mucinous cystadenoma: This is characterized by tubular adenomatous epithelium with varying degree of epithelial atypia. It produces large amount of mucin with prominent luminal dilatation of up to 6 cm. it is the most common form, constituting about 50% cases and with associated 20% risk of perforation [13,14]. The fourth group encompasses the malignant mucinous cystadenocarcinoma; characterized by glandular stromal invasion and/or tumour cells in peritoneal implants i.e. Pseudomyxoma peritonei. It sometimes resembles mucinous carcinoma of the colon. It constitutes about 11-20% of all cases with 6% risk of spontaneous rupture [13,14]. Cystadenoma and cystadenocarcinoma are neoplastic appendiceal mucocele, constituting about 35% of all primary neoplasm of the appendix [11,14].
The clinical presentation of the disease does not have a specific picture. It often flows asymptomatically as in this case. In about 50% of cases it is discovered accidentally during radiologic and endoscopic examination or at surgery. However, a patient's clinical symptoms may include pain, palpable abdominal mass, nausea, vomiting, weight loss, gastrointestinal bleeding, and signs of intussusceptions of the intestine [9,13,14].
Pre-operative diagnosis of appendiceal mucocele is very important for the selection of an adequate surgical method to prevent peritoneal dissemination to prevent intraoperative and postoperative complication and repeated surgery [13].
Sonographic examination is considered the first line diagnostic modality that can probably differentiate benign and malignant mucocele [15]. An appendicular diameter of 15 mm or more has been determined the threshold for diagnosis of mucocele with a sensitivity of 83% and a specificity of 92%. Computerized tomography (CT) scan is important to confirm the diagnosis and to evaluate the extent of the disease.
Fine needle aspiration cytology (FNAC) is not usually recommended as it increases the risk of perforation and dissemination in to peritoneal cavity [16]. Colonoscopy usually reveals an elevation of the appendicular orifice. In addition, a yellow mucous discharge would be visible as well. Colonoscopy is also important for the diagnosis of synchronous or metachronous cancers when present.
Conventional surgery is generally preferred to laparoscopic approach as the latter increases the risk of rupture, but laparoscopic appendectomy is performed for selected patients which confer the advantages of minimal-access surgery, including the avoidance of a large incision, a better cosmetic outcome and a short convalescent period [17-20]. Simple appendectomy is the choice for patients with benign mucocele as suggested by the presence of a normal caecum and appendicular base and no evidence of perforation as in our patient. As in our case presented, the patient had open appendectomy as the pathology was incidentally found intraoperative while performing open cholecystectomy. In our centre, there is little or no laparoscopic setting and minimal laparoscopic skill, being a semi-urban to rural setting in a low income region. Right hemicolectomy is recommended when malignant mucocele is suspected by the presence of a perforated mucocele, enlarged mesenteric lymph node or a positive cytology. An accurate exploration of the abdomen is advised due to the well-known association between the appendiceal mucocele and other mucin-secreting cells such as colon and ovarian cancers [21].
Mucocele of the appendix is a rare disease with vague symptoms. Abdominal ultrasonographic scan important diagnostic tool, but histopathology is needed for definitive diagnosis. Surgery for benign appendiceal mucocele has an excellent long-term prognosis.
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for images and other clinical information to be reported in the journal. The patient understand that her name will not be published and due efforts will be mode to conceal her identity.
Nil.
There are no conflicts of interest.