The aim was to compare the neonatal and maternal short-term outcome after an emergency caesarean to the outcome after an elective and after a second stage c-section. A possible impact of the weekday and time of the day as well as the incision-to-closure time within the overall collective and the decision-to-delivery time regarding emergency caesareans on neonatal and maternal outcomes was examined.
Retrospective analysis of the performed c-sections between 2004 and 2014 was carried out at a maximum-care- clinic.
Emergency c-sections correlate significantly with low APGAR-scores, pH and a higher rate of the need of oxygen mask, intubation, reanimation and transfer to NICU.
There was a higher rate of blood loss (p = 0.00001), anaemia rate (p = 0.0001) and an increased rate of fever (p = 0.01345) in emergency c-sections. Time and weekday have been influential factors as regards to the maternal and neonatal outcomes.
In 319/320 emergency c-sections, a decision-to-delivery time within 20 minutes was achieved. The postnatal pH- value was lower the longer the decision-to-delivery time was. The decision-to-delivery time was significantly shorter between 08:00 and 16:00 in comparison to other times and at the weekend. The other neonatal and maternal outcome parameters did not show significant differences.
In the majority of cases a decision-to-delivery time of 20 minutes in a clinic with Level I care is feasible. A shorter decision-to-delivery time involves a better pH-value at birth. The maternal complication rate after emergency caesarean is not significantly higher in comparison to the one after an elective or second stage c- section with regard to time and weekdays. The higher rate of blood loss, anaemia and fever in emergency c- section are treatable conditions, but should bare in mind when performing an emergency c-section.
Caesarean, Emergency caesarean, Decision-to-delivery-time, Neonatal outcome, Maternal outcome
Today's obstetrics in Europe is organized in a differentiated way. Risks for mother and child have been reduced significantly. This becomes apparent in the decreased perinatal mortality rate. In 1980 it was 12.4/1,000 live-births. In 2000 it went down again to 4.4 and settled down at a stable level between 3-4% [1] in Germany and Europe.
The maternal mortality has also declined considerably. At the beginning of the 20th century the rate of maternal deaths at live births was 300-350/100,000 in Europe. Maternal deaths in Europe are rare, however, an under - reporting has to be assumed. The maternal deaths in Europe include information of under 3/100,000 births to 10/100,000 [2,3].
An established and regulated pregnancy care, the use of prenatal diagnostics, guidelines for the care of premature infants but also the structural and supply policy aspects implemented in hospitals, have a significant influence on the decreased perinatal and maternal mortality rate. The aim of today's birth clinics is to provide the highest level of safety for mother and child. This includes the ability to react immediately and without delay to emergencies with the complete range of sensible medical and caregiving treatments.
While the amount of births in hospitals has been increasing steadily, a stagnation and an insignificant reduction in the rate of caesarean sections can be registered since 2012. The rate of caesareans in Germany was at 31.1% and 31.8% in the years 2015 and 2014. The caesarean rate in Europe fluctuates from 50% in Cyprus for example, to 30% in many central and southern European countries, and below 20% in countries such as The Netherlands, Finland, Sweden and Norway [1-3].
In a statement, miscellaneous national institutes have agreed on minimum requirements for process-related, structural and organisational requirements regarding obstetric departments. So the standard for the time between indication and c-section, the so-called decision-to-delivery time in an emergency was set at 20 minutes in Germany and 30 minutes internationally [4-7].
Considering the fact that the interval for the performance of an emergency caesarean was determined decades ago, a very limited amount of studies exist which investigate the neonatal and maternal outcome after an emergency caesarean in comparison with the outcome after an elective or second stage c-section. This is indeed surprising, as this set interval plays a decisive role in court cases [8,9].
Previous studies focussed on the evaluation of neonatal and maternal outcomes with regards to the decision-to- delivery time. Yet, the results are quite controversial. Some studies report no difference in the neonatal and maternal outcome, or a reduced morbidity, in decision-to-delivery times which exceed the 30 minutes [10-12].
This study investigates to what extent the neonatal and maternal short-term outcome after an emergency caesarean differs from the outcome after an elective primary c-section as well as after a second stage c-section.
Additionally it also evaluates to what extent the time and weekday influence the neonatal and maternal outcomes. Furthermore, it analyses to what extent the incision-to-closure time within the overall collective as well as the decision-to-delivery time influences the neonatal and maternal short-term outcome.
For this retrospective data analysis, births performed by emergency caesareans in the years 2004 to 2014 were selected from the obstetric database of the Hannover Medical School. Missing data were obtained from medical records. The data used for evaluation purposes were inserted in Excel and anonymised.
All single pregnancies from 24+0 gestational weeks delivered by caesarean section in the period from January 2004 to December 2014.
Multiple pregnancies, gestational week < 24+0, all spontaneous and vaginal operative deliveries. Known foetal abnormalities in elective c-sections. Intrauterine death.
The following parameters were collected for the descriptive analysis: maternal age, gestational age at c-section, BMI, indication of c-section, maternal underlying disease.
Furthermore, the incision-to-closure time for all c-sections and additionally the decision-to-delivery time for emergency caesareans were noted.
Primary, neonatal outcome parameters are:
-APGAR scores after 1, 5 and 10 minutes
-pH value of arterial umbilical cord
-necessity for mask oxygenation
-necessity for intubation
-necessity for reanimation
-necessity for transfer to NICU
Primary maternal outcome parameters are:
-blood loss
-postoperative anaemia
-impairment of wound healing
-necessity for hysterectomy
-necessity for (re-) laparotomy
-fever for longer than 2 days after surgery
-sepsis
-maternal death.
The birth clinic is a so-called Level I centre (corresponding to Level III in USA and UK). The labour ward is fully equipped with all facilities of foetal and maternal monitoring. Residents, consultant, midwives, anaesthetists and anaesthetic caregivers, surgical caregivers as well as paediatricians and paediatric caregivers are present at all times. There is an operating theater in the labour ward, in which not only the elective caesareans but also the emergency interventions such as emergency caesareans are carried out. Moreover, the instrumental requirements for carrying out emergency caesareans are available in each cubicle of the delivery room. If possible the emergency caesareans are carried out in the operating theater.
The decision and indication for a caesarean is always made by a consultant.
All planned procedures have been defined as elective, primary c-sections.
The necessity for carrying out a caesarean within the next 30-60 minutes while the delivery process is defined as a second stage c-section.
Emergency c-section is defined as the need of an immediate delivery in order to minimise the maternal or neonatal risk.
The study was approved by the Ethics Committee of Hannover Medical School (no:2588-2015).
The statistical analysis was carried out in cooperation with the Institute of Statistics at the Leibniz University Hanover. All evaluations were made with the statistics programme R (http://www.cran.r-project.org).
Mean comparisons and regression analysis were performed. The calculation was done for the whole sample and filtered by time and weekday and compared with each other afterwards. The time of the day was divided in 0800-1600, 1600-2400 and 2400-0800. The weekdays were structured in working days and weekends. In case of metric parameters a two sample t- test (Welch Test) and in case of 0-1 scale variables a two sample binominal test was used. Significance was achieved if p < 0.05.
The analysis included 3,045 pregnancies, which were delivered by caesarean section during the period of the study. Among those were 320 emergency caesareans, 1,528 elective c-sections and 1,197 second stage c- sections.
Table 1 displays the demographic details of the collective. Maternal, underlying diseases and indication of c- section are shown in Table 2.
Table 1: Maternal and neonatal demographic details. View Table 1
Table 2: Maternal characteristics and indication for caesarean section. View Table 2
Table 3 shows the births' modi, which are allocated to the different times of day and weekdays (divided into working days and weekends).
Table 3: Absolute und relative (%) distribution of birth modi depending on time and weekday. View Table 3
75% of the elective caesareans are carried out between 0800 to 1600. Nearly 7.5% of the elective c-sections are carried out between 2400 and 0800, whereas 23.13% of all emergency caesareans are carried out in this time span. Nearly half of the emergency caesareans and of the second stage c-sections occurred between 0800 and 1600.
In total, approximately 16% of the caesareans were carried out at the weekend. Around 10% of the elective c- sections took place at the weekend, whereas nearly 23% and 22% of the emergency and second stage c-sections were carried out.
The type of delivery is significantly correlated with the time of day (K*0.3455, p < 0.0001) and the weekday (K*0.2392, p < 0.001).
Table 4 shows in summary the means of each neonatal outcome parameter of the emergency c-sections, elective and second stage c-sections for the APGAR-scores and pH values.
Table 4: APGAR-score and pH-outcome value for emergency, elective and second stage c-section with regards on the whole collective and considering time and weekday. View Table 4
In the emergency caesarean group APGAR-scores are higher between 1600 and 2400 than at any other time. Here week-days barely differ from the weekend. There are no differences in regard to the pH values.
The necessity for intubation seems to be less frequent between 1600 and 2400 as well as at the weekend. The necessity for reanimation and transfer to NICU occurs at a similar level. However, these differences are not significant.
Regarding the elective c-sections, APGAR-scores are significantly higher between 0800 and 1600 in comparison to other times and also on weekdays in comparison to weekends. The pH value does not differ within these time periods, but is higher in elective c-sections than in emergency caesareans.
The oxygen mask is used significantly more often between 1600 and 2400 (p = 0.002) in comparison to other times and more often at the weekend than during the week (p = 0.0081). The reanimation rate (p = 0.0026) and the transfer to NICU (p = 0.0001) is significantly higher between 1600 and 2400.
As regards second stage c-sections, the values for the APGAR 1' and 5' after 1600 and at the weekend are lower but not significantly. No significant differences are portrayed for all other outcome parameters.
An emergency caesarean correlates significantly more frequently with lower values for APGAR 1 (r = -1.7587, p = 0.00001), APGAR 5 (r = -1.2233, p = 0.00001), APGAR 10 (r = -0.7295, p = 0.00001), pH (-0.1141, p = 0.00001) and an increased rate for the use of oxygen mask (r = 1.5595, p = 0.00001), intubation (r = 2.1404, p = 0.00001), reanimation (r = 1.6451, p = 0.0001). as well as transfer to NICU (r = 0.8812, p = 0.00001) in comparison to elective and second stage c-sections.
Taking into account the variables of time and weekday, significantly higher values for APGAR 1 (r = 0.1737, p = 0.0373) and a lower rate in reanimation (r = 0.5237, p = 0.0064) are found between 0800 and 1600 in comparison to the other c-sections. In the time from 1600 to 2400 the NICU transfer rate was significantly higher (r = 0.2979, p = 0.0432) in emergency caesareans than at any other time intervals. The other neonatal outcome parameters do not show significant (all p-values > 0.5) differences between emergency caesarean and elective and second stage c-sections. Between working days and the weekend no significant differences were found between type of births.
Sub analysis regarding pH values < 7.20 and < 7.15 revealed that the pH value was always significantly lower (pH < 7.20, r = -0.0800, p = 00001; pH < 7.15, r-0.0719, p = 0.00001) in those babies who were delivered by emergency caesarean than in those by elective or second stage c-sections, regardless of the variables of time and weekday (all p-values > 0.05).
Concerning the rate of anaemia (p > 0.05) and the rate of blood loss (p > 0.05), no significant differences depending on time of day and weekdays were found between the respective type of births.
In total, there were only a few complications. These are listed as follows for the groups emergency caesareans, elective and second stage c-sections: Bleeding above 1,000ml in 5 (1.6%), 8 (0.5%) and 5 (0.4%) cases, 4 (1.3%), 8 (0.5%) and 8 (0.6%) impairments of wound healing in need of revision, 3 (0.9%), 7 (0.5%) and 4 (0.3%) hysterectomies, 5 (1.6%), 10 (0.7%) and 8 (0.7%) (re-) laparotomies, 7 (2.2%), 9 (0.6%) and 7 (0.6%) cases of fever > 2 days p.p., 1 (0.31%), 3 (0.2%) and 2 (0.2%) cases of sepsis. One woman, who received an emergency caesarean after a poly-trauma, died from her severe injuries.
A further analysis of the maternal complication rate divided into time and weekday, has not been carried out due to the low case numbers and consequently their limited validity.
The regression analysis shows that there is higher blood loss (r = -0.7365, p = 0.00001), an increased anaemia rate (r = 0.8481, p = 0.0001) and an increased rate of fever (r = 1.3355, p = 0.01345) in emergency c-sections than in elective or second stage c-sections.
The blood loss during elective c-section is also significantly increased (r = 0.1486, p = 0.0002) in comparison to second stage c-section but lower than during emergency caesareans.
As expected, the incision-to-closure time did not show a significant influence on the neonatal outcome (p-value was always > 0.05) because logically the duration of the surgery has no influence on the neonatal outcome.
In respect of the maternal outcomes the following results are shown for the overall collective: A positive correlation between the duration of the surgery and the complication rate was noted. The longer the incision-to-closure time, the higher the blood loss was (r = 0.0046, p = 0.00001), the higher the postoperative anaemia rate (r = 0.0152, p = 0.00001), the higher the amount of hysterectomies (r = 0.0377, p = 0.00001) and of (re-) laparotomies (r = 0.0192, p = 0.0001) and the rate of the postnatal occurrence of fever (r = 0.0132, p = 0.0462). However, the rate of for impairment of wound healing (p = 0.7569) and sepsis (p = 0.3811) differed not significantly.
The decision-to-delivery time had no significant influence on the maternal outcome parameter (all p-values > 0.05).
Figure 1 demonstrates that the longer the decision-to-delivery time, the lower the pH value at birth (r = -0.6413, p = 0.0208) is. No significant difference could be proven for the remaining parameters: APGAR 1' (p = 0.8387), APGAR 5' (p = 0.9974), APGAR 10' (p = 0.6618), interventions with oxygen mask (p = 0.6122), intubation (p = 0.7351), reanimation (p = 0.2263), transfer to NICU (p = 0.5118).
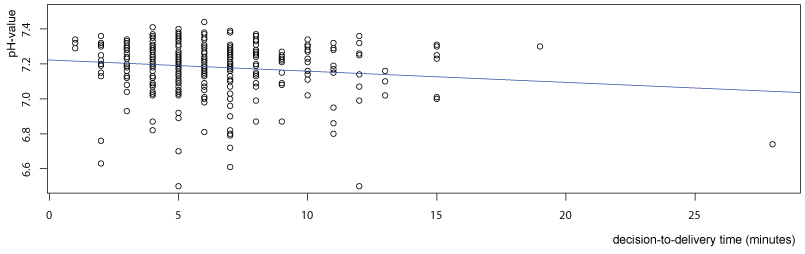 Figure 1: Correlation of pH-value and decision-to-delivery time. View Figure 1
Figure 1: Correlation of pH-value and decision-to-delivery time. View Figure 1
Subsequently, the analysis in dependency to weekdays and the weekend as well as the time showed the following result: The delivery-to-decision time was significantly shorter (r = -1.480, p = 0.000302) on weekdays than at the weekend (Figure 2).
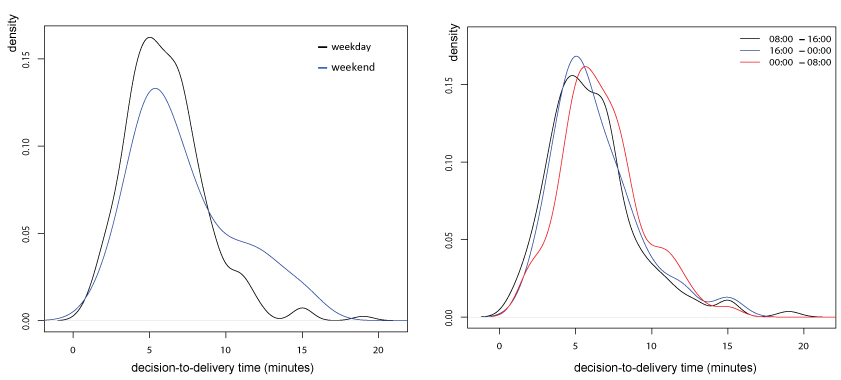 Figure 2: Decision-to-delivery time depending on weekday and time. View Figure 2
Figure 2: Decision-to-delivery time depending on weekday and time. View Figure 2
On weekdays, the pH-value was significantly lower, the longer the decision-to-delivery time (r = -0.9122, p = 0.0151) took. At the weekend no significance could be established (p = 0.5019), which, however, could be due to the low case numbers.
In respect to the variable time, the following results were noted:
Between 0800 and 1600 (r = -0.9214, p = 0.036) shorter decision-to-delivery times were established in comparison to 1600 to 2400. The decision-to-delivery time between 2400 and 0800 (r = 0.8265, p = 0.0441) was significantly longer than between 0800 and 1600 as well as between 1600 and 2400 (Figure 2).
Taking into account the variable time, no significant differences could be determined with regard to the neonatal and maternal outcomes (all p-values > 0.05).
In their guidelines various national and international professional associations recommend that an emergency caesarean should be carried out within 20 to 30 minutes [4-7].
In the meantime, several studies have evaluated both the feasibility of the time limit and the complication rate during emergency caesareans in comparison to the planned caesarean sections [13-19]. A review analysis [13] resulted in the fact that 82% of the emergency caesareans could be carried out within 30 minutes. Yet, the 5' APGAR score and the birth pH value were worse in deliveries within 30 minutes. Various studies [9,20,21] also came to the conclusion that the neonatal outcome was worse if delivery was within 30 minutes after indication and that the outcome does not necessarily have to be worse if the decision-to-delivery time is longer than 30 minutes [9,13,21,22]. Other studies [10,11,23,24] were not able to prove a correlation between umbilical cord-outcome- pH values, APGAR values and decision-to-delivery time.
The contradictory data situation is highlighted again by additional study results [14,16,17,25,26], which prove that newborns with short decision-to-delivery time had a better outcome and that despite a short preparation time, the maternal risks and complications do not increase. The results of this study also demonstrated that the birth-pH was significantly lower with extended decision-to-delivery time.
It certainly has to be taken into account in the analysis of the emergency caesareans and the interpretation of the study results that the indication for an emergency caesarean is based on a real foetal stress situation, which in turn means that the rate of depressed newborns is expected to be high. This is also reflected by the results of this study. The average 1' APGAR score was 6.62, 5' APGAR score 8.21 and the birth pH values at 7,18 (Table 4). A correlation between the decision-to-delivery time and the APGAR outcome values could not be proven. Yet, this may be due to the overall relatively short decision-to-delivery time within our collective. Overall, our study results were able to demonstrate that the neonatal morbidity and mortality rate was significantly lower when the decision-to-delivery time was lower.
The comparison of the studies is sometimes difficult. Although there is a consensus regard on the definition 'emergency caesarean', its use varies in everyday practice. Additionally, not all studies are from clinics with maximum care (Level I in Germany, Level III in USA and UK) so that there are not only differences in the organisational process but also in the collective of expectant mothers. This is due to the fact that one can expect a higher percent of high risk pregnancies in a clinic with maximum care.
An emergency caesarean can also increase complications on the part of the mother through operative complications and the effect of the general anaesthetics [21,26,27]. The complication rate in the present collective was low. The one maternal death was not due to the emergency caesarean itself but due to the underlying problem of the severe poly-trauma. More recent studies [16,17,28] cannot affirm the increased complication rate anymore despite less preparation time. This is comprehensible as structural, organisational and hygienic progress has lowered the complication rates. The peri-operative antibiotic prophylaxis, which, by now, has become part of the standards, was able to decrease the postoperative infection rate drastically [29].
This retrospective analysis demonstrates that the decision-to-delivery time of 20 minutes was feasible in 319 of 320 emergency caesareans. The decision-to-delivery time concerning one emergency caesarean was 28 minutes. A new aspect of this study was the investigation of the outcome in regard to the time of day and weekdays. The results demonstrate that the decision-to-delivery time was significantly shorter during weekdays and in the morning between 0800 and 1600. During this period the staff resources are fully available which guarantees a quick realisation of the required measures.
Recently, studies were able to prove [30,31] that human receptivity, the realisation and implementation of tasks and therefore the efficacy and the resulting safety for the staff are inconsistent and that performance follows a circadian rhythm. Analyses of the medical care [32-34] demonstrate the influence of the physicians' and medical staff's working hours as well as the influence of the shift and night work both on the cognitive performance and the susceptibility to make medical errors as well as on their well-being.
Significant differences concerning the neonatal and maternal outcomes were not shown in our study. Yet, is has to be mentioned that the results are representative for a house with maximum care, in which there is a full team consisting of obstetrical staff, surgery care, the anaesthetics team and the paediatric team present at any time and any weekday.
Skilled staff within a team, present and ready to act within minutes, are certainly significant factors which influence the decision-to-delivery time, as well as the distance between cubicle of the delivery room and the operating theater. Furthermore, studies were able to show that the decision-to-delivery time was significantly shorter with skilled and trained staff [35].
The retrospective data analysis allows the insight into the documented course of birth and the indication emergency caesarean. Yet, it is impossible to analyse and quantify the detailed perception and observation of the Obstetrics. This is certainly also viewed as a limitation in studies which have been carried out previously.
Moreover, these are the study results of data from a university clinic, in which the organisational, interdisciplinary and staff emergency caesarean alarm structure has been established in the obstetric department for years.
On the other hand, prospective, randomised studies are not realisable nor ethically justifiable as pregnant women, who are in an emergency situation due to their condition or due to the foetal situation, cannot be randomised into groups, which deliver either within 20 minutes or after 20 minutes.
Nowadays, the time interval determined within guidelines plays an important role in court cases [8,9], whereby the defined time is supposed to serve as a point of reference and the constellation in each case ought to be evaluated individually [36].
Numerous studies have shown that a delivery within 20 to 30 minutes after recognition of the emergency, is unfortunately not necessarily accompanied by a good neonatal and maternal outcome and therefore there is no guarantee.
Fundamentally, it should be noted that it seems reasonable to carry out an emergency caesarean or a second stage c-section as quickly as possible after the indication.
Nowadays, the adherence to a decision-to-delivery time serves as a quality indicator for the organisational structure within the obstetric department, especially clinics of maximum care. High rates in decision-to-delivery times may indicate relevant organisational problems.
The results of this study, which are representative of a level I clinic in Germany, show that a decision-to-delivery time of 20 minutes is feasible in the majority of cases with well established organisational structures and skilled staff.
The maternal complication rate during emergency caesareans is not significantly higher than the rate during elective and second stage c-sections.
The authors declare no conflict of interest.
The study was approved by the Ethics Committee of Hanover Medical School on 2nd of February 2015 (no:2588- 2015).
There was no funding.
We are grateful for the support for the statistical analysis, which was carried out by Prof. Sibbertsen and Dr Bertram from the Institute of Statistics of the Leibniz University Hanover.