The use of waterpipe tobacco among young person's has become a social norm, in spite of awareness of its potential toxic effects on health [1,2]. A single session of waterpipe smoke delivers as much tar as one pack of cigarettes, while it contains nicotine and other carcinogens [3-5].
Waterpipe tobacco smoking (WTS) behavior has been reported among students in several regions, with prevalence between 20-80% [6,7]. The behavior historically existed under various names, (shisha, hookah and narghile) and is considered native to Eastern Mediterranean region [8], where health-promotion specific research is understudied [1,9-11].
WTS has been used for ceremonial activities characterized by strict rules for preparing, lighting and smoking the waterpipe and over time was integrated into traditional EMR culture [12]. Since the early 1990s WTS became more commercialized with the introduction of various flavors, sophisticated marketing campaigns, and transnational distribution networks, which promote smoking behavior throughout the EMR and many Western countries, particularly among youth [1,13-15]. The media associates WTS with lavishness, while some brands market their product specifically to women and youth, resulting in increasing popularity and familiarity with this type of smoking behavior [14]. In this region, parents commonly engage in WTS while in the company of their sons and daughters [16]. The sharing of waterpipes among family members is often how young adults initiate WTS since this type of behavior is more acceptable for their age group than the use of cigarette [16,17]. This familial factor may contribute to the early age of initiation for WTS compared to cigarettes.
The EMR has a high prevalence of WTS and rates are increasing. A longitudinal study among youth in Jordan revealed a 42% increase in WTS prevalence over the 2-year study period [18]. Results of the BREATHE study indicate that WTS prevalence rates among adults over 40 years of age are around 3.5% and even higher in EMR countries compared to Northern Africa [19]. In most EMR countries, the proportion of males who smoke waterpipes is higher than females [19,20]. Yet the male-female difference is much smaller compared to cigarette smoking because girls smoking waterpipes is more socially acceptable compared to smoking cigarettes in some parts of the EMR [21]. A few studies have even shown that, waterpipes have replaced cigarettes as the most common form of tobacco use for the youth population [22]. For many of them, WTS is their first tobacco experience, and facilitates subsequent use of cigarettes, encouraged by the optional flavors and access to social settings for use [18,23,24,].
The World Health Organization (WHO) has released a scientific advisory note to address the growing concerns about the increasing prevalence and potential health effects of WTS, especially in EMR countries [25]. A lack of awareness and persistent belief of the reduced risk in the use of WTS exists, particularly among youth. Some persons may not be aware of the harm involved in the use of waterpipes, and believe it is safer than cigarette use, because the process of WTS uses water as a filter [16,17]. Negative health outcomes associated with tobacco use are well-documented, yet few people are convinced that WTS behavior is harmful [16,26,27].
We aimed to describe the behavior and perspective towards WTS among female Emirati college students and apply qualitative analysis to identify thematic influences that promote initiation and use. This study also explores attitudes towards the use of health-warning labels on tobacco products.
Participants recruited for this study were female full-time college students, and self-reported waterpipe users (N = 10) currently enrolled in an undergraduate program at a government university in Abu Dhabi, the largest Emirate in the UAE. Abu Dhabi is the capital and the seat of government [29]. It has a population of approximately 3.15 million residents, occupying 87% of the geographical land mass. Most recent statistics indicate that 68% of the Emirati population in Abu Dhabi is younger than 30 years of age with a median age of 19 [29]. Recruitment efforts were carried out by faculty who visited classes randomly, to introduce the study, describe its purpose, design, confidentiality, and location for anonymous individual interviews. A total of 155 female students were approached, with a final sample of 10 students who presented themselves for participation. All participants were bilingual (Arabic/English) Emirati nationals and enrolled in full-time tertiary education within an academic institution using English as the language of study.
The study was approved by the research ethics committee of (Name of institution). All participants provided consent to record their answers and include content from the interviews for the purpose of this study and reporting.
This study was a qualitative design, using face-to-face interviews with individual participants. The lead research team member conducted semi-structured interviews in English in person, and in an anonymous office setting located on the college campus. Interviews were framed around constructs of the Social Cognitive Theory (SCT) [30] and included questions that focused on personal, environmental and behavior influences of WTS. Additional questions were aimed to assess the WTS users' perceptions of WTS related health-warning labels. The interview included questions about experience of smoking behavior, types and choice, efficacy of warning labels and other feedback (Table 1). Interviews were conducted in individual sessions of approximately 45 minutes for each participant. Participants were encouraged to draw on their own WTS experiences and to discuss any issues of personal importance.
Table 1: Participant guide questions for semi-structured WTS interview. View Table 1
The recordings of participants, were transcribed by a trained research assistant and cross-checked by a member of the research team. An initial transcript was coded around the main interview topics, and then applied to all data. Following careful line-by-line scrutiny of emergent themes and analysis to identify thematic issues resulted in a preliminary coding-index. The remaining transcripts were coded line-by-line using this index, and emergent themes were then used to refine and extend the index. A member of the research team coded the transcripts using the finalized index. Discussions were held to resolve inter-analyst disagreements in interpretation, and a consensus was reached through clarification or amendment.
The final element of the interview, included a request for the participant to discuss and rank eight health-warning labels, presented in English and Arabic (Figure 1) based on their perceptions of each label's efficacy. These labels were first developed as possible health warning labels for waterpipe tobacco packages and related accessories based on preliminary research [31]. Health warning labels on waterpipe tobacco products vary across the EMR and are not always in Arabic. Furthermore, qualitative descriptors for waterpipe accessories have been known to contain misleading information. Nonetheless, evidence exists that health warning labels on cigarette packages increase awareness of health risks among smokers and non-smokers and decreases tobacco consumption [32].
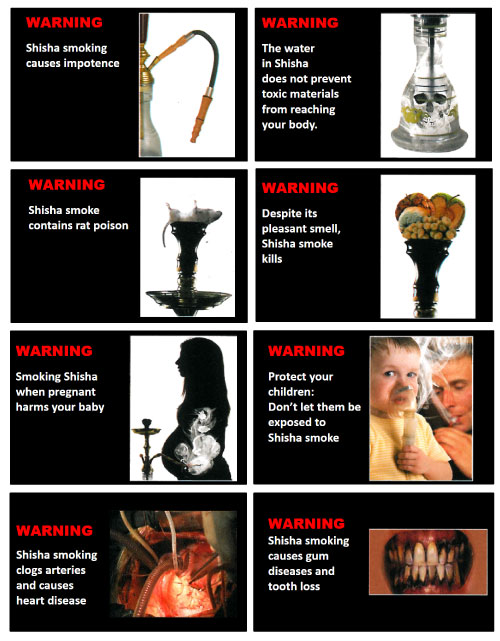 Figure 1: Health warning labels reviewed by self-reported WTS users.
View Figure 1
Figure 1: Health warning labels reviewed by self-reported WTS users.
View Figure 1
A total of 10 female undergraduate students participated in one-on-one face-to-face interviews. All participants identified as Emirati, which is consistent with the demographics of the government institution, targeted primarily at UAE citizens. The mean age of participants was 21.7 (SD = 2.81). One participant self-identified as both WTS and cigarette smoker, and another reportedly used WTS and medwakh. All other participants exclusively engaged in WTS.
The qualitative analysis of student interview transcripts identified four perceived influencing factors broadly summarized as: secrecy and norms, exclusivity, family influence, and olfactory/gustatory attraction (Table 2). Additional data describes students' response to the effectiveness of health warning labels to reduce WTS among youth (Table 3).
Table 2: Personal, Environmental, and Behavioral Influences of WTS among female Emirati college students. View Table 2
Table 3: Influence of health warning labels on WTS among female Emirati college students. View Table 3
Secrecy within the family and in public, emerged as a key factor for engaging in WTS behavior. Females reported specific strategies for maintaining secrecy in order to maintain family norms that dictate who is allowed to engage in smoking behaviors. All of the participants reported that they hide their WTS behavior from family members, particularly males. The participants described several strategies they use to keep their WTS behavior a secret, at venues that provide space for shisha and other tobacco smoking and even in their home, among family members. When asked to elaborate on the concept of secrecy in the home, a participant described how she sometimes smokes waterpipe in a garden outhouse, after one of the families' domestic workers prepares the waterpipe for her:
In our home, we have this outside kitchen thing, and the maid already has the shisha set up. When nobody is home, I'm like 'make it for me. She does, and I'm under the table [breathes in mimicking deep inhalation], and I keep doing it and seeing if anyone is coming. And then I'm like 'don't tell anyone, I'm going to get really upset. She's my friend. I have a friend in the maid (Participant 1).
Second hand smoking was perceived as another way of engaging in WTS behavior without being identified. This was done by intentionally sitting amid family members who are smoking, and inhaling, which is perceived as a stronger effect.
At the last family gathering, I sat between my grandma and my mom. My grandma was smoking a cigarette, and my mom was smoking shisha. They were telling me 'go sit there, but I wanted to sit beside them (Participant 9).
Although it is more acceptable for males to engage in smoking behaviors than females, some parents supported their daughter's tobacco use, if the behavior occurred in the home, and not in public. One participant reported that her mother allowed her to smoke cigarettes only in her room but forbid her to do so in public. The idea of engaging in any smoking behavior in public goes against family norms and impedes on the family reputation.
When participants described their WTS behavior in public and the importance of secrecy, they described several strategies for hiding their behavior that worked for them. Some participants will target venues where shisha is offered (shisha cafés or beach bars), and where Emiratis are not frequent customers to minimize the risk of being recognized by someone known to their family. Since opportunity is key, it was not surprising that participants reported only engaging in WTS behavior between 2-10 times in the past six months, and timing was of importance. Since Shisha cafés open most days of the week, participants described they chose weekdays and daytime hours in order to minimize recognition by a person known to the family. Even inside the shisha cafés or similar venues, participants went through great length to sit in strategic locations that they perceive make it harder to be seen even when someone enters the venue. Although some venues charge a fee for the request to be concealed, this did not seem to deter participants from engaging in WTS behavior.
The shisha industry offers alternatives for WTS behavior without familial recognition Home delivery services now exist, which deliver all the tools needed to smoke shisha, to include the waterpipes and the fresh coals. Other venues include a drive-in service to accommodate clients, which works well for the participants who need to keep their behavior a secret. Emiratis traditionally use cars with heavy tinted windows, and it is the norm that females have a private chauffeur, who is perceived as a trustworthy source. Although smoking is the norm in most households, the fear of being recognized by family members exists, and participants agreed that the consequences would be severe, if their secret was uncovered.
WTS is more common among females and a more acceptable form of tobacco use, in spite of the aforementioned secrecy. Only 8 of the 10 participants reported that they exclusively use shisha, while one participant also uses cigarettes and another reported medwakh as her second option. Participants self-identified as occasional smokers or opportunistic smokers and suggested that WTS behavior was a social activity engaged in with other female friends and or family members. The exclusive use of WTS is sometimes perceived as a socially enhancing activity that reduces feelings of stress.
I come up with brilliant ideas whenever I'm smoking while writing with my right hand, smoking with my left hand. My brain doesn't stop functioning, and I get the missing word or the time or the structure or the idea…or the inspiration (Participant 1).
Although smoking was perceived as a less acceptable norm among families, participants still felt they initiated WTS because of family practices. Every household reportedly engages in tobacco smoking and being around family members influenced their ability to arrange WTS within the household. When asked how early participants initiated WTS behavior, most reported they started as early as high school.
You know they smoke in front of us then wonder where we got the idea from. It doesn't matter if you're a man or a woman, we've been taught to do this (Participant 8).
Another factor that influenced WTS behavior was the attractive aromas and variety of flavors available. The idea of choosing from many different flavors, was exciting and apriority when ordering WTS at any venue away from home, with apple, double apple, grape and mint as the most popular flavors.
…I don't know what it is exactly. It's like blueberries if I'm not mistaken… Blue mist is light and tastes cold—like when you brush your teeth and get a cool breeze (Participant 4).
Most participants agreed that health warning labels would do little to stop students from engaging in WTS and did not seem to express concern about the potential adverse effects to their health. Some participants drew parallels between health-warning labels and people trying to encourage them to wear the hijab (headscarf):
Like we already know that! It's like people coming up to me like, 'you should wear a scarf because… and I say listen, Islam has existed 1400 years now. I know about this. It's not like I'm an ignorant, waiting for you to tell me this. I know. I just don't want to do it (Participants 3 and 8).
Another participant felt disgusted looking at the labels and suggested they might work in the short-term but wasn't sure the effect would last. None of the participants had previously seen any health warning labels on waterpipes, at venues that offer WTS. One participant reported she had seen such a warning during a visit to Germany. When asked what type of message on warning labels would have the greatest impact on WTS behavior, participants ranked gum disease (Figure 1) with the caption "Shisha smoking causes gum diseases and tooth loss" as number 1.
Secrecy related to social norms was an essential characteristic of WTS behavior among female Emirati college students in our study. All of the participants engaged in WTS and two also engaged in cigarette smoking. The findings of this study are supported by previous research on the influence of familial factors on smoking behavior among young populations [16]. Few participants believe that current efforts such as health warning labels are effective, and most agree that contradicting messages are not effective to convince students and reduce initiation or reduce the use of WTS. Social stigma and the belief that smoking in public may be damaging to one's personal or family reputation was an overarching theme of concern among participants. This social stigma is reminiscent of smoking-related gender-types prevalent in Europe and North America, dating back to the 17th century, when paintings of female smokers were depicted in erotic photography [33]. Young populations with access to the internet and a barrage of unfiltered information, are more vulnerable than ever, and easily convinced that a health warning may not be a serious matter. This study did not explore sources of information to describe students' support for or against WTS behavior.
The desire to keep WTS behavior a secret has implications for health promotions and cessation programs. Perceived behavior control and intention to quit, without the fear of being socially stigmatized, may be an important influencer of help-seeking behavior. However, anticipated stress, may influence a person's ability to change their behavior. Social stigma related to gender, may unintentionally increase smoking behavior, and achieve the opposite of health promotions programs to reduce initiation and use of tobacco products [34].
This study had some limitations. The random selection of participants who are WTS users did not allow us to describe factors that deter non-users from similar factors such as familial influencers or health warning labels that influence WTS behavior. The focus on WTS did not adequately represent multiple tobacco produce use, although at least 1 participant reportedly used WTS and cigarettes. Behavioral constructs were only partially explored and may have revealed additional information to describe the WTS use among this population.
This study is the first of its kind and provides an opportunity for expanding research designs to better describe WTS behavior among the target population.
Almost all WTS users agreed that familial factors and olfactory factors promoted rather than discouraged the initiation and use of WTS. However very few believed that the use of health warning labels was an effective strategy to reduce the long-term use of this form of tobacco among females. Social stigmas further influence familial factors towards initiation, but other factors such as education and awareness of health risks may be the basis for future research. While this study addresses influencers of initiation and use, ongoing research in this area is needed to address barriers to change. Policymakers may need to consider mandatory use of health warning labels to encourage tobacco cessation and reduce WTS behavior, rather than sustain or possibly increase initiation and use among youth and implement health education programs to address the early initiation of tobacco use in the UAE.