There is an alarming rise of chronic kidney disease (CKD) prevalence globally, which is associated with significant morbidity and mortality necessitating special attention as a major public health problem. Data on the burden of CKD on the African continent are sparse for rural population. Hypertension related kidney disease accounts for a large percentage of the population requiring renal replacement therapy worldwide. Therefore, we determined the burden of CKD in patients with hypertension attending a tertiary hospital located in a rural community.
This cross-sectional study included patients of a medical outpatient clinic in Federal Teaching Hospital Ido Ekiti, Ekiti State, Nigeria. Study patients were consecutively recruited from Cardiac clinic and baseline data were obtained from the patients' files which include the blood pressure, plasma creatinine, age, gender, ethnicity, and other necessary data. Glomerular filtration rate (GFR) was calculated using estimated GFR by Modification of diet in renal disease (MDRD) equation. The estimated minimum sample size was 179 with probability of type 1 error, assumption of α = 0.05 and power of 95%. A total of 204 patients with the minimum number of investigation results were included.
A total of 204 hypertensive patients were studied. The patients were aged between 29 and 90 years with a mean age of 62.9 ± 12.9 years. The study population was made up of 93 males and 111 females. Overall, about 50% of the patients at presentation have CKD (GFR below 60 ml/min/1.73 m2), p < 0.05. Majority of the patients belonged to the low socioeconomic class presenting with stage 2 hypertension.
The burden of CKD in this report among hypertensive patients suggest a significant public-health problem on the basis of the tremendous burden of CKD among the poor, its distribution among the patients, and the existence of effective treatments that are not affordable and available to a large proportion of these groups of people.
Chronic kidney diseases, Hypertension, Prevalence, Outpatients, Poverty, Blood pressure
Chronic kidney disease (CKD) is a leading cause of morbidity and mortality in both developed and developing countries, with an estimated 10% of the population worldwide having CKD [1,2].
The number of patients with CKD worldwide is rising markedly [3]. The European average around 135/1000000 and that of the United States 336/1000000 [4]. The overall prevalence of CKD in adult populations living in Africa was 15.8% for CKD stages 1-5 and 4.6% for CKD stages 3-5 in the general population. Equivalent figures were greater at 32.3% and 13.3% in high-risk populations (people with hypertension, diabetes, HIV) [5].
Hypertension is a chronic disease that is increasing in prevalence worldwide and spans race and gender lines. An estimated 1.13 billion people worldwide have hypertension, most (two-thirds) living in low- and middle-income countries [6].
Despite widespread awareness of the complications associated with hypertension, especially in those with CKD, the rates of hypertension, the rates of end stage renal disease (ESRD) attributable to hypertension and the rates of CKD continue to rise in the worldwide [7].
Perry, et al. [8] demonstrated the intimate connection between blood pressure (BP), cardiovascular disease risk and risk of CKD in their 15-year follow-up study of approximately 12,000 hypertensive individuals at multiple Veterans Affairs centers in the USA.
Hypertension is the driver of the cardiovascular disease (CVD) epidemic in Africa where it is a major, independent risk factor for heart failure, stroke and kidney failure [9-11]. In Africa, pooled prevalence of CKD is 24.7% in hypertensive [12]. Hypertension remains a very important cause of kidney related morbidity and mortality in sub- Saharan Africa [9].
The prevalence of CKD in Nigeria is 11.4-26% [13]. Hypertension is a major cause of CKD and chronic renal failure (CRF) in Nigeria. In Enugu (South East) and Benin City (South South), hypertension is the commonest cause of CKD and CRF [14,15]. It is only second to chronic glomerulonephritis in the South West [16-18]. Virtually all these reports are from urban settings.
The finding of impaired renal function in a hypertensive patient is frequent and constitutes a very potent predictor of future cardiovascular events and death even in treated patients [19-21].
Individuals with estimated GFR (eGFR) < 60 mL/min have an approximate 16 percent increase in CVD mortality, and individuals with eGFR < 30 mL/min have a 30 percent increase [22].
Despite global declines in hypertension, hypertension of adults in sub-saharan africa (SSA) continue to rise [23,24] and the age-adjusted prevalence of hypertension in SSA is estimated to be the highest of any region in the world [25].
In view of the scarce data on burden of CKD in hypertensive patients in the rural setting of Nigeria, this study was purposely conducted to determine the burden of CKD in hypertensive patients referred to the cardiology unit in a rural setting which is rarely reported.
This study was a cross-sectional study on patients with hypertension attending the Cardiology clinic in a Federal Teaching Hospital Ido Ekiti, Ekiti State, Nigeria. This is a tertiary hospital located in a rural community of Ekiti state in Nigeria. It is the only hospital located in a rural community in the entire southwest zone of Nigeria and only very few of such exist in other regions of Nigeria. Many patients attend the hospital as referrals from primary and secondary care clinicians within and outside the state; many choose to make the hospital their first point of call when they need medical care.
Patients attending the clinic consist of referred cases from within the hospital or other secondary health centers in the state or neighboring states. Eligible patients were consecutively recruited in the study.
The inclusion criterion for enrolment includes all patients attending the clinic for hypertension treatment with no identifiable secondary cause. Patients attending the clinic during the period of study were considered based on this criterion. Patients with incomplete (needed) data were excluded and 204 patients were included in the final analysis.
Information were obtained from the patients' files by the senior resident physicians between year 2017 and 2018 which included demographic characteristics, BP, fasting blood glucose (FBG), serum creatinine, smoking and alcohol status, duration of hypertension, history of diabetes mellitus (DM), anthropometric measurement and other relevant information. Documented data in the case files were obtained in our clinic by standardized methods. Weights (kg) were measured by standardized techniques and equipment [26]. The BP was measured with a mercury sphygmomanometer at least twice in each participant with at least five minutes of rest in between, with the subject seated in a chair and relaxed, the back supported, and the arm at heart level. During the initial screening, BP of both arms was measured with mercury sphygmomanometer and the arm with higher BP used subsequently. The FBG and fasting lipid profile were determined using venous blood by conventional laboratory devices after an overnight fast.
Plasmacreatinine assay was performed at the Chemical Pathology Laboratory of the hospital. This was performed using modified Jaffe's reaction method with creatinine kits from Agape following standard protocol provided in the leaflet. Assay results were read on a manual microplate reader (MR-96A) manufactured by Mindray (Schenzen Mindray Biomedical Electronics Co, Ltd). This method removes bilirubin which causes positive interference in the measurement of creatinine by the known kinetic enzymatic jaffe's reaction by reducing bilirubin in the sample to biliverdin using potassium ferricyanide prior to the known jaffe's reaction producing results which agree closely with isotope dilution mass spectrometry (IDMS).
Re-expressed MDRD 4-variable version (MDRD 4-variable GFR equation) using serum creatinine values that were standardized to reference methods were adopted [27,28]. Hence, the eGFR was calculated by the abbreviated MDRD equation: 175 × (plasma Creatinine)-1.154 × (Age)-0.203 × (0.742 if female) × (1.212 if black). On this basis, the eGFR were categorized simply as < 60 or ≥ 60 mL/min/1.73 m2 according to the recommendation of national institute of diabetes and digestive and kidney diseases (NIDDK) [29] in reporting eGFR ≥ 60 mL/min/1.73 m2.
The following definitions were adopted for this study. Hypertension: Persistently elevated BP of ≥ 140 mmHg for systolic or 90 mmHg for diastolic or both, based on at least two readings on separate occasions after the initial screening or those receiving treatment for hypertension [30]. The choice of 140/90 mmHg as a cut-off point is based on the Seventh Report of the Joint National Committee on prevention, detection, evaluation and treatment of high blood pressure (JNC 7) criteria [30]. DM: Diagnosed according to the World Health Organization diagnostic criteria [31]. Dyslipidaemia: National Cholesterol Education Programme Adult Treatment Panel III (NCEP ATP III) cut-off points were used to identify participants with desirable, borderline high and high levels of lipoprotein risk factors [32]. Smoking and alcohol: Considered present if reported up to the day of the interview. Metabolic syndrome was defined according to WHO definition [33].
The overall estimated population-based data on prevalence of hypertension among Nigerian is 28.9% [34]. Therefore, we estimated the sample size based on this prevalence. The estimated minimum sample size was 179 with probability of type 1 error, assumption of α = 0.05 and power of 95%.
Data were analysed using the SPSS software package for windows version 16 (SPSS Inc. Chicago, Illinois, USA) and presented the result as descriptive statistics of the hypertensive adult patients. The groups were compared using the Chi-square test for categorical variables represented as number (percentage). Continuous variables were represented as the mean ± standard deviation in case of normal distribution, otherwise presented as medians. A p-value less than 0.05 was considered as statistically significant.
A total of 204 hypertensive patients were studied. The patients were aged between 29 and 90 years with a mean age of 62.9 ± 12.9 years. The study population was made up of 93 males and 111 females. There was statistical significance difference in the mean age of patients with GFR of equal or more than 60 ml/min/1.73 m2 and that of less than 60 ml/min/1.73 m2 (Table 1). The two groups show no statistically significant differences in gender, smoking history, alcohol consumption, duration of hypertension, FBG, and lipid profile. In contrast, there was statistically significant difference in body weight, body mass index (BMI), systolic BP, diastolic BP, and eGFR between the two groups.
Table 1: Baseline characteristics of patients stratified by eGFR group. View Table 1
Table 2 shows the proportion of hypertensive patients in different stages of CKD with majority in stage 3 (35.2%). Overall, about 50% of the patients at presentation have CKD (GFR below 60 ml/min/1.73 m2), p < 0.05.
Table 2: Proportion of hypertensive patients in different stages of chronic kidney disease. View Table 2
In Table 3, majority (52.9%) of the referred patients presented with stage 2 hypertension. The burdens of CKD were in increasing order of BP categories with majority found in stage 2 (47.1%)), p = 0.000. Isolated systolic hypertension (ISH) accounted for 7.4% of total patients out of which 4.9% of the patients have CKD, p = 0.049.
Table 3: JNC 7 and isolated hypertension stratified by eGFR, ml/min/1.73 m2. View Table 3
In Table 4, majority of the patients belonged to the low socioeconomic class such as petty trading, peasant farming, patients who had retire, and others (unemployed, job loss, nonspecific job). Only 22.1% of patients were civil servants.
Table 4: Distribution of CKD categories by occupation among hypertensive patients. View Table 4
Figure 1 shows the graphical representation of the patients with majority of the patients clustering in stage 2 and 3 CKD; thereafter, showing a major decline. Presence of any of the hypertensive patients in CKD < 30 ml/min/1.73 m2 decline precipitously to only one of the occupational groups at GFR < 15 ml/min/1.73 m2.
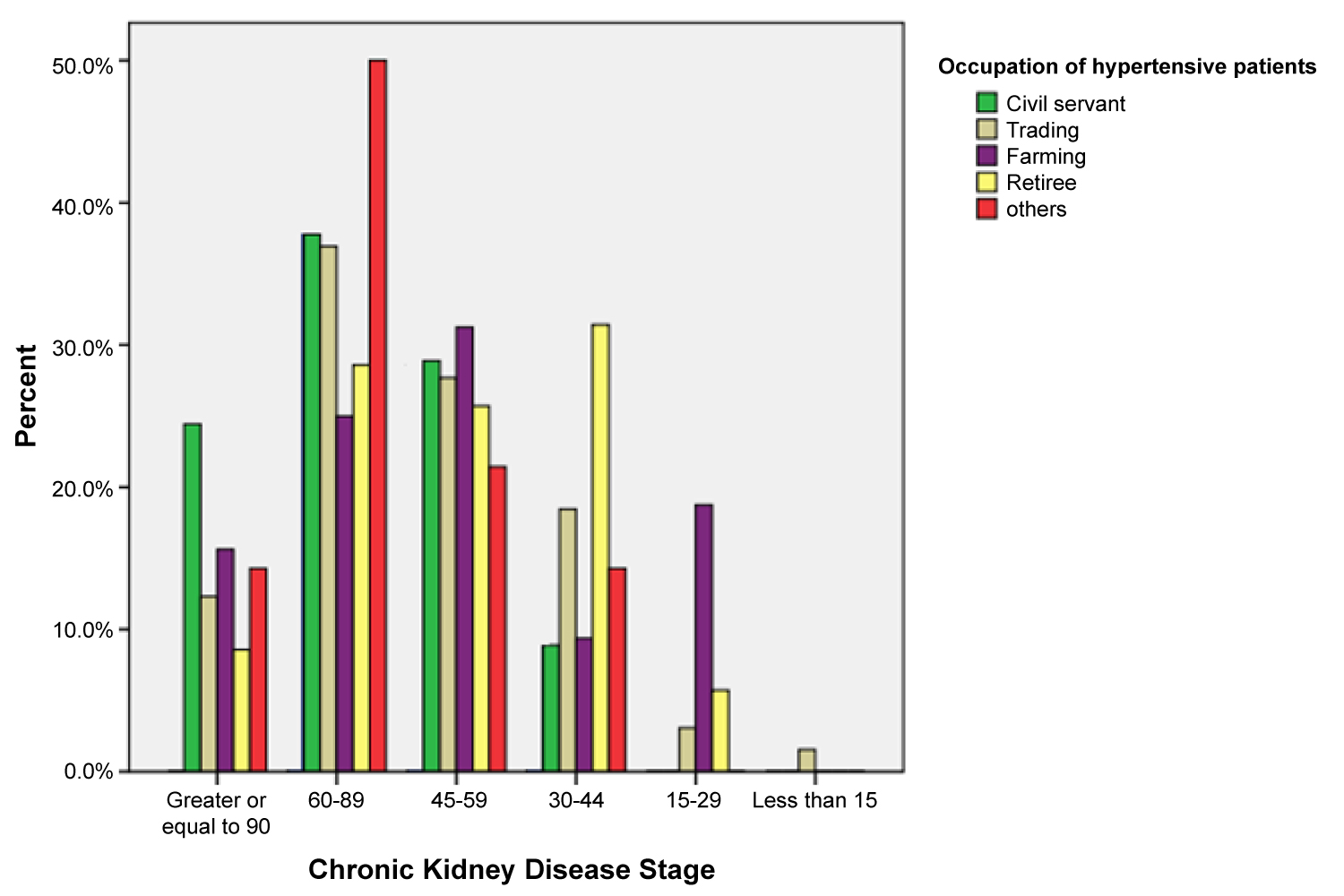 Figure 1: Distribution of Chronic kidney disease stages by occupation of the hypertensive patients.
View Figure 1
Figure 1: Distribution of Chronic kidney disease stages by occupation of the hypertensive patients.
View Figure 1
Our study found a CKD burden of 50.5% for CKD stages 3-5 (moderate to severe decrease in kidney function) in the hypertensive outpatient clinic of adults attending a tertiary hospital located in a rural community. Among the 50.5%, majority (89.3%) are in CKD stage 3. This heavy burden is possibly due to the fact that majority of the patients referred to the specialist clinic are in stage 2 hypertension (52.9%). Poorly controlled BP is a known risk factor for the development of CKD and cardiovascular complications and lowering of BP was associated with a reduced risk of developing CKD [8]. Our finding of CKD burden was double that of similar work done in an urban situated tertiary hospital of a neighboring state which reported 23.3% [35]. Similarly, multicenter screening study done in city center, Accra in Ghana, reported a prevalence of 27.8% of CKD stages 3-5 [36]. However, in the former study only about one-third (32.2%) compared to over half (52.9%) of the patients were in stage 2 hypertension; while the latter study was conducted in polyclinic as against specialist clinic in our study where complicated cases are referred.
Additionally, the burden of CKD is higher in women than in men in our findings as previously reported [37] although without statistical significance. We discovered low smoking history (5.4%) and alcohol consumption (11.8%) that were not significant, and lack of significant lipid profile which are all similar to the community-based study conducted by Ogunmola, et al. in the community where the hospital is located [10]. Hypertension duration and FBG do not significantly show difference in the two categories of CKD possibly due to possible variation in treatment compliance as a confounder and greater population of diabetic patients with a comorbidity of hypertension being referred to the endocrinology clinic respectively. Findings in the two categories of CKD show significant differences in age, weight, BMI, DBP, and SBP in consistent with available knowledge [38].
There was a progressive increase in the burden of CKD from normal through stage 2 hypertension with the highest proportion in stage 2. This shows statistical significance findings in patients at stages 1 and 2; and Isolated Systolic Hypertension. This is similar to previous work [39] except the trend from normal to prehypertension which the small sample size for the two groups may be responsible. Previous workers as shown that control of hypertension is the single most effective determinant of CKD burden [40]. Pooled analyses of many of these studies have consistently shown that the lower the BP, the slower the progression of CKD [40].
Similar to CKD, awareness of hypertension is low. Previous data has reported this, showing that more than half of US adults with hypertension were aware of their disease in 1999-2004; less than half were treated for their hypertension with medications; and less than two-thirds of those achieved good control [41,42]. This problem is worse in developing countries and worst in less urban communities compounded by illiteracy and poverty [43,44]. As a consequence of late detection and referral for treatment, damage to the end organs in the form of CKD expectedly higher in our study population than in places where better healthcare systems exist and hypertension is detected and treated optimally.
Our findings showed that over 78% of the patients are below poverty line (petty traders, peasant farmers, retirees, and other groups without stable or specific job). We found substantial percentage of all the patients in subgroup analyses to fall in CKD stages 3-5. It is noteworthy that the civil servants who expectedly have regular income revealed lesser proportion of patients in CKD stages 3-5 compared to others. Low socioeconomic status (poverty) with the consequent limited access to healthcare, poor nutrition, and housing have been reported to contribute to the incidence and prevalence of hypertension and CKD [45]. Poverty has several pathways through which it can be associated with kidney disease and hypertension. For example, there is strong evidence that intrauterine events linked to poor nutrition alter prenatal programming and lead to low nephron number, which represents a substantial risk factor for CKD in later life [46]. This is relevant to global health given the emerging food crises worldwide in the face of COVID-19 pandemic devastating effects on the world economy.
Therefore, lack of affordable health care service in our area of study can contribute to the high prevalence of renal impairment among our hypertensive population who will only present for treatment at the onset of complications of hypertension.
Overall evidence of clustering of patients in stages 2 and 3 suggest significant proportion waiting to cross from stage 2 to 3 and 3 to 4. Importantly, the resources to implement effective early detection and prevention programs for CKD, like all non-communicable diseases (NCD), must ultimately come from government health programs to improve public health, to decrease the costs of managing CKD, and CVD; and to respond to public demand.
It is already known that (even in developed nations) only a small minority of people with CKD will develop kidney failure, partly because of the competing risk of cardiovascular mortality [47]. Data from the US show that for every patient with ESRD, there are more than 200 with overt CKD (stage 3 or 4) and about 5000 with covert disease (stage 1 or 2) [47]. In stage 3, representing almost 40% of the CKD population (similar to our study), the number that will progress to ESRD is estimated at only about 0.15-0.2% per year over 10-25 years [48-50]. A much greater problem is the now well-documented eight- to ten-fold increase in CVD mortality in CKD populations, thus strongly linking CKD to CVD, one of the four major NCDs prioritized in the Global NCD Action Plan [48,49,51].
In this report, CKD owing to hypertension is likely an overestimate because of alternative diseases that are likely undiagnosed or overlooked due to lack of biopsy and histological study on the patients. This is a general challenge in estimating the precise prevalence of CKD secondary to hypertension alone.
The burden of CKD associated with hypertension depends largely on the definition of CKD used. The kidney dialysis outcomes quality initiative (KDOQI) classification provides a step-wise progressive definition of CKD ranging from albuminuria with preserved GFR (stage 1) to ESRD with GFR < 15 ml/ min/1.73 m2 (stage 5). Early (stage 1 and stage 2) CKDs were included in the KDOQI classification to incorporate individuals with obvious renal parenchymal damage (for example, proliferative lupus nephritis) but preserved GFR. Without further clinical information, it is impossible to identify which individuals classified as having stage 1 and 2 CKD. Thus, use of the KDOQI classification of CKD and, specifically, use of a single measurement of kidney function such as micro-albuminuria, might not be the best method for identifying CKD prevalence. Thus, stage 1 and 2 were excluded in this study because firstly, the presence of a single measurement of micro-albuminuria does not confirm the presence of glomerular disease or parenchymal kidney injury. So, it was not feasible in our setting of poor patients. Estimates of CKD are probably overestimated even by the measurement of persistent microalbuminuria [52]. A 2010 debate questioned the relevance of microalbuminuria measurements in the diagnosis of kidney disease and controversy regarding its use as a marker of CKD still exists [53-55]. The results of the Avoiding Cardiovascular Events through Combination Therapy in Patients Living with Systolic Hypertension (ACCOMPLISH) study highlights the limitations of using microalbuminuria as a marker of kidney disease and predictor of CKD progression [56].
The findings of Crews, et al. [57] also highlight the limitations of using criteria that have been established for the classification of disease severity for establishing a diagnosis.
To date, the available literature exploring the epidemiology of CKD overall has not classified individuals according to the underlying etiology. However, in the absence of overt glomerular disease, such as in hypertensive nephrosclerosis or early diabetic nephropathy, evidence of early kidney injury remains elusive.
The burden of CKD in this report among hypertensive patients suggest a significant public-health problem on the basis of the tremendous burden of CKD among the poor, its distribution among the patients, and the existence of effective treatments that are not affordable and available to a large proportion of these groups of people. Therefore, the rationale for the need to consider prevention of CKD through focus on modification of CVD risk factors for hypertension and early detection and treatment of hypertension and CKD.A combination of population-wide and individual health-care interventions is required to make control of hypertension affordable and equitable in these lower income settings [58-62].
Olarinde Jeffrey Oluwademilade: Study design, Data collection, Statistical analysis, Data interpretation, Manuscript preparation and Literature Search.
Gbadebo Oladimeji Ajani, Fasanmi Tolulope Kolawole, Omotola Olawale Obajolowo, Eunice Oluremi Olabinri and Segun Matthew Agboola: Manuscript preparation.