The number of adult cases of rhinolith is uncommon. Rhinoliths are hard stony mass that are found in the nose that can progress over a long period of time leading to nasal symptoms and sometimes ear symptoms. This is a case report of a 40-year-old lady that came with unilateral tinnitus and blood stained rhinorrhea, but on further investigation was found to have rhinolith mimicking symptoms of nasopharyngeal carcinoma due to the position of the rhinolith in the fossa of Rosenmuller.
Nasopharyngeal rhinolith, Rhinolith, Nasopharyngeal carcinoma, Unilateral tinnitus, Middle ear effusion
Rhinoliths are not common and are calcareous concretions formed by salt deposition namely calcium and magnesium on a foreign body in the nasal cavity [1-4]. They are normally found unilaterally, but can also be found in both the nasal cavities [5]. Most of them are found on the floor of the nose, but rhinolith found in the fossa of Rosenmuller are rarely seen [5-7]. Patients can come with symptoms like nasal blockage, unilateral nasal discharge, some can be foul smelling and blood stained [8]. If rhinoliths are arising from the fossa of Rosenmuller, patientscan have ear pain, bad breath and globus sensation [7]. Nasal endoscopy and CT scan are the modalities used for proper diagnosis of this condition [9,10]. Complete removal of rhinolith, debridement with administration of antibiotics are the treatment of choice [11,12]. Early detection and complete surgical removal of rhinolith help in the resolution of the symptoms and for the prevention of complications [12]. We reviewed a case of a rhinolith in the fossa of Rosenmuller mimicking symptoms of nasopharyngeal carcinoma.
A 40-year-old lady with an underlying hypertension presented with reduced hearing over the right ear for the past one month. It was associated with tinnitus. She complained of daily clear foul smelling rhinorrhoea with occasional blood stains and right sided nose block for the past one year. Otherwise, she had no ear discharge, ear pain, vertigo, facial asymmetry, facial pain, blurring of vision, loss of weight or loss of appetite. She could not remember inserting any foreign body into her nostrils when she was younger. She also has no history of any psychiatric illness. Her mother has a history lymphoma.
Rigid nasal endoscopy showed bilateral inferior turbinate hypertrophy. There was a mass seen arising from the nasopharynx obliterating the right fossa of Rosenmuller encroaching the right nasal cavity (Figure 1). It was friable and bleeds upon contact. Left fossa of Rosenmuller was not obliterated. On otoscopy, a dull tympanic membrane was seen with air fluid level over the right ear whereas the left ear was normal. There were no palpable neck nodes. Tympanometry showed type B on the right ear and type A on the left ear. Pure tone audiometry showed right ear had mild conductive hearing loss with normal hearing over the left ear.
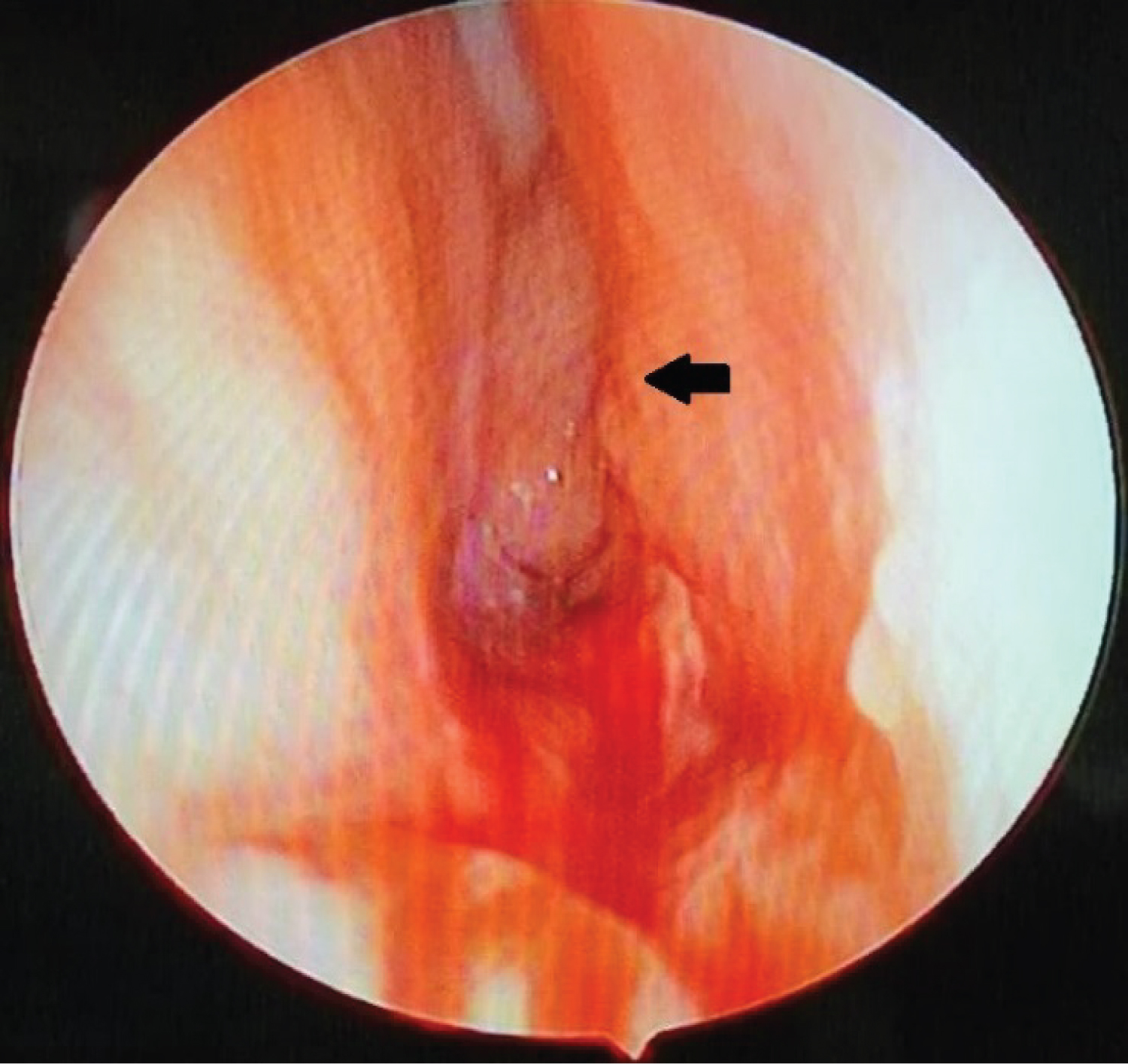 Figure 1: Black arrow shows mass in the right nasal cavity that bled on contact seen on rigid nasal endoscopy.
View Figure 1
Figure 1: Black arrow shows mass in the right nasal cavity that bled on contact seen on rigid nasal endoscopy.
View Figure 1
Biopsy of the nasopharyngeal mass was taken. It was reported as acute and chronic inflammation. We proceeded with contrast enhanced CT scan of the paranasal sinuses which showed enhancing lesion of right fossa of Rosenmuller with coarse calcification (Figure 2 and Figure 3). There was also presence of chronic paranasal sinusitis with remodelling of bilateral maxillary and right sphenoid sinuses walls.
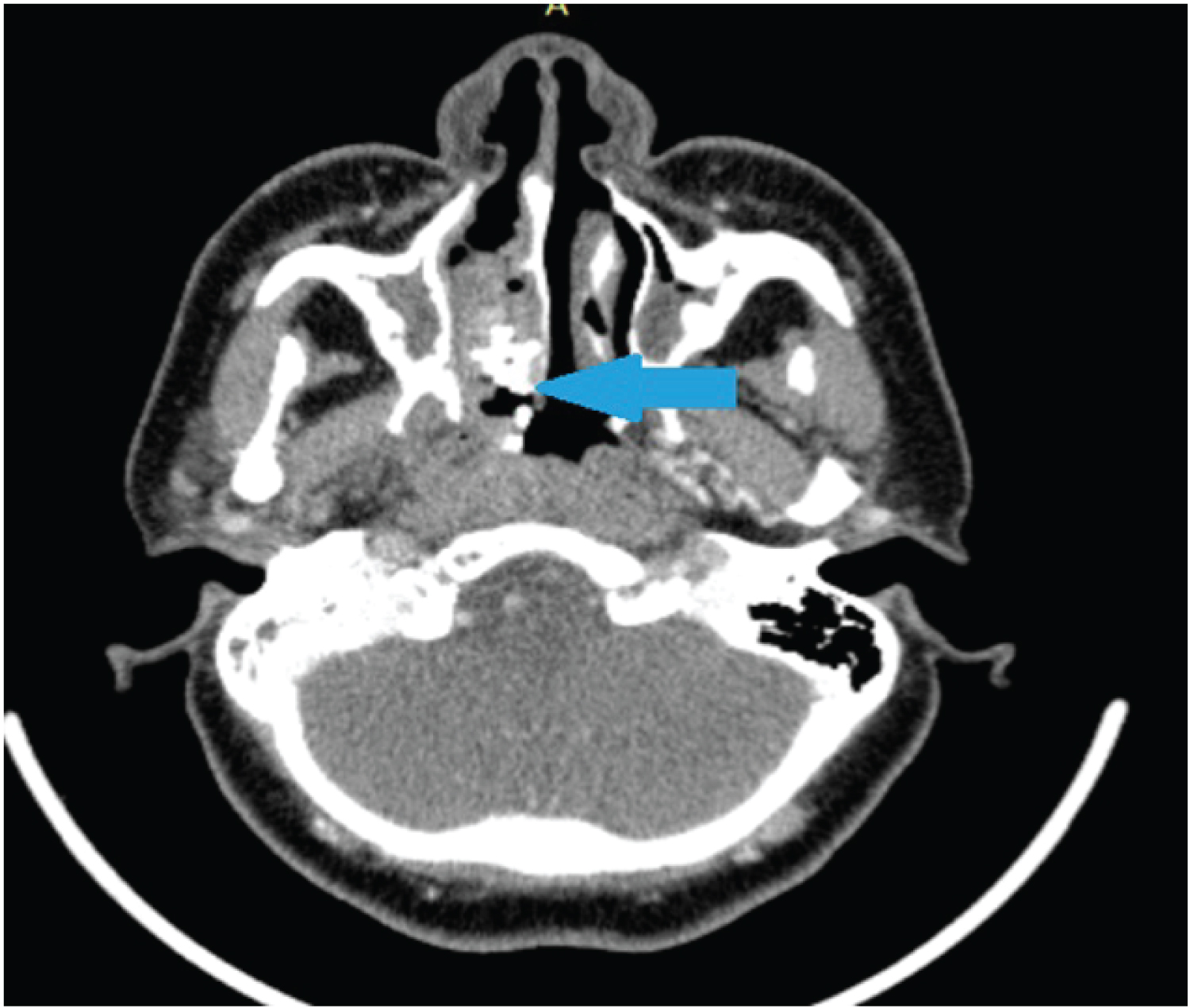 Figure 2: Axial cut of Contrast enhanced CT scan. Blue arrow showing rhinolith in the nasal cavity with soft tissue surrounding it.
View Figure 2
Figure 2: Axial cut of Contrast enhanced CT scan. Blue arrow showing rhinolith in the nasal cavity with soft tissue surrounding it.
View Figure 2
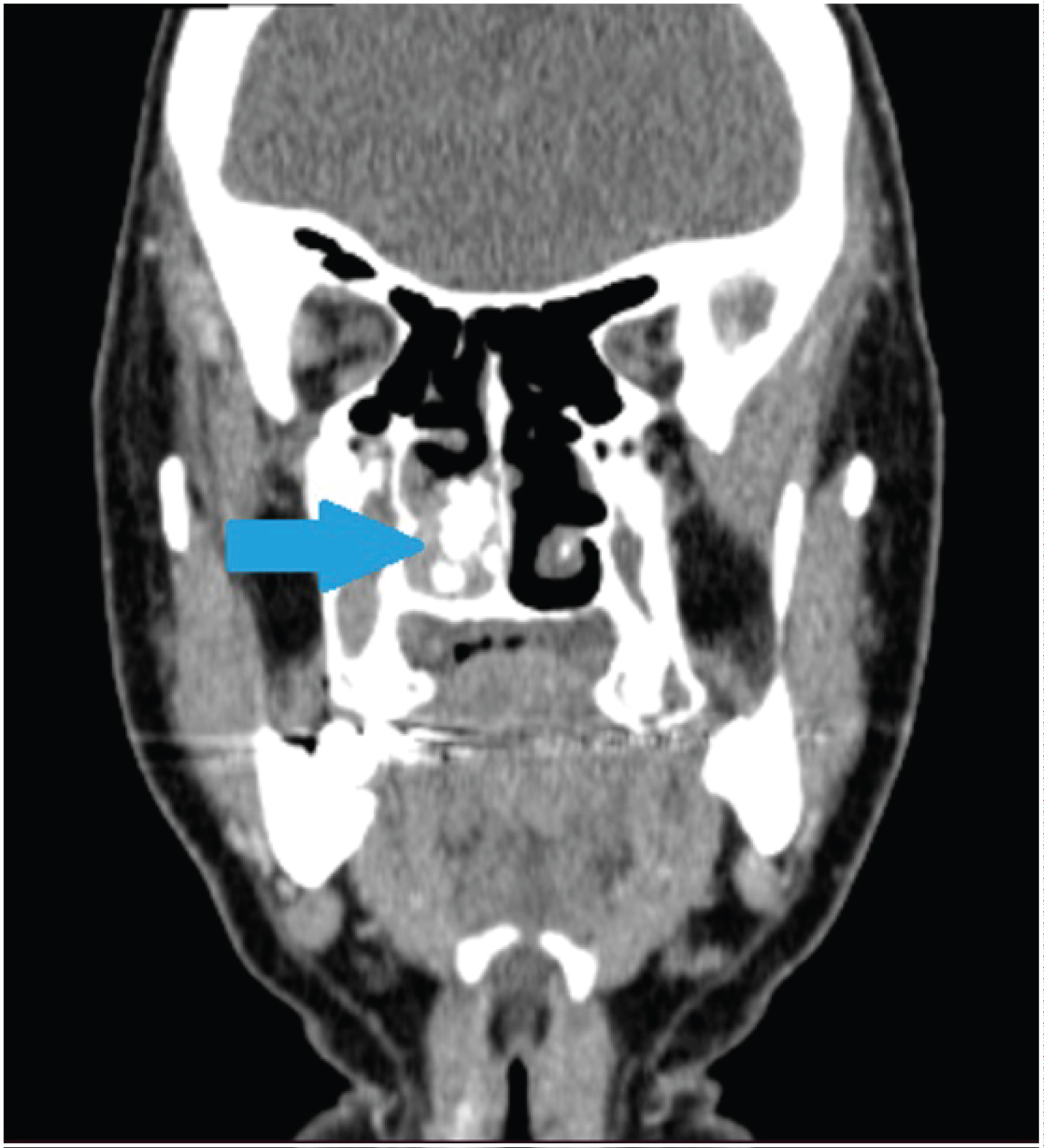 Figure 3: Coronal cut of Contrast enhanced CT scan. Blue arrow showing rhinolith occupying the right nasal cavity with resorption of right inferior turbinate.
View Figure 3
Figure 3: Coronal cut of Contrast enhanced CT scan. Blue arrow showing rhinolith occupying the right nasal cavity with resorption of right inferior turbinate.
View Figure 3
Examination under anaesthesia, biopsy and partial right inferior turbinectomy was done. Intraoperatively, there was an irregular, friable, granulation tissue surrounding the rhinolith which bled on touch. Posterior end of inferior turbinate was resorbed. Granulation tissue was seen at the nasopharynx occluding the right eustachian tube opening. Biopsy of the right nasopharyngeal mass showed inflammed granulation tissue with bacterial colonies. The histopathological report of the rhinolith came back as calcified material. She was discharged after two days of nasal packing with oral antibiotics and nasal douching.
On subsequent follow up, the patient no longer complained of nasal blockage, tinnitus and reduced hearing. Rigid nasal endoscopy showed evidence of turbinectomy, posterior choanae and bilateral fossa of Rosenmuller were clear. Otoscopy showed resolved middle ear fluid on the right ear with repeated tympanometry of type A. She was now well and discharged from our care.
Rhinolith is very uncommon with incidence of 1:10000 in a study of outpatients in ENT [1,2]. Rhinoliths or calculi of the nasal cavity are calcareous concretions which are formed by salt deposition namely calcium and magnesium on a foreign body intranasally [3,4]. Rhinoliths are mostly seen in the thirties and are rare in children with a female preponderance [13]. They are usually seen in one nasal cavity, but some are seen on both the nasal cavities [5]. Rhinoliths are commonly seen on the floor of the nose, however, there are some literature showing rhinolith in the fossa of Rosenmuller [5-7].
The pathogenesis of rhinolith are unclear. It is said to arise from the foreign body acting as a nidus causing chronic inflammation and deposition of mineral salt over a long period of time [3,11,14,15]. The nidus can usually be exogenous or less commonly endogenous [9,10]. It enters into the nasal cavity anteriorly or posteriorly through the nasopharynx by means of vomiting, coughing or even sneezing [12]. The rhinolith in our patient was in the Fossa of Rosenmuller which may suggest a retrograde manner.
Symptoms of patients vary and are based on the location and size of the rhinolith [12]. They usually come with nasal symptoms like one sided nasal discharge, nasal block, some associated with a foul smell and blood stained [8]. But in our case, she came mainly because of her ear symptoms namely tinnitus and unilateral reduced hearing despite having nasal symptoms as well as due to the rhinolith being in close proximity to the Fossa of Rosenmuller. Upon further questioning, she admitted having nasal symptoms like blood stained rhinorrhea and nasal blockage. Initial diagnosis of nasopharyngeal carcinoma was made in view of the mass that was present from the fossa of Rosenmuller that obstructed the opening of the eustachian tube.
Nasal endoscopy is the modality of choice to diagnose this condition [9]. CT scan can also be done as it is able to determine the size of the rhinolith, location and any associated abnormalities [10]. CT scan was performed in our case to look for the extension of the right nasal mass as we had nasopharyngeal carcinoma as the provisional diagnosis. Benign tumors like ossifying fibroma, osteoma, hemangioma and enchondroma as well as malignant tumors for example osteosarcoma and chondrosarcoma can be differential diagnoses that can be thought of for this case [6]. However, for this patient an incidental finding of a rhinolith with features of sinusitis was seen on CT scan.
The treatment of choice for this condition is complete removal of the rhinolith from the nasal cavity, debridement of granulation tissue and administration of suitable antibiotics. Depending on the location and size, it can be performed under general anaesthesia or local anaesthesia. Due to the advancement of technology, patients can now be treated endoscopically [11,12]. Our patient underwent the procedure under general anaesthesia and the removal of the rhinolith was done endoscopically. Partial turbinectomy was performed as the posterior end of inferior turbinate was shrunken and resorbed. Biopsy was taken and it confirmed the diagnosis of rhinolith in the fossa of Rosenmuller and had ruled out nasopharyngeal carcinoma.
Complications like nasal mucosa destruction, recurrent sinusitis, septal perforation and deviation, oroantral and oronasal fistulas, perforation of the palate are usually associated with rhinoliths. Complications as such can be avoided if cases are detected early [16].
Rhinoliths in the fossa of Rosenmuller are rare. Like most rhinolith, in this patient it was found incidentally. Proper and full clinical examination should be conducted with a high index of suspicion when dealing with patients having foul smelling rhinorrhea, worsening unilateral nasal obstruction with unilateral nasal bleeding. Endoscopic nasal examination and CT scan should be done to confirm the diagnosis as it can detect rhinolith in rare places. Early detection and complete surgical removal of the rhinolith are needed to prevent recurrence and complications.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.