Osteomas are benign tumors that can originate and grow in the paranasal sinuses. Many are asymptomatic and only require tomographic control. When they produce symptoms, treatment is surgical. Different surgical approaches have been proposed, with a trend in the last decade to perform endonasal surgery with endoscopes using simple, extended or combined transnasal approaches.
To determine the efficacy of surgery to resect symptomatic frontoethmoidal osteomas, and to establish the factors that could facilitate an endonasal approach with endoscopes.
All patients who were surgically treated for osteomas located in the ethmoid and frontal sinuses between August 2007 and June 2021 were included. The characteristics of the osteomas (location, size, implantation) were retrospectively analyzed.
Seven patients were surgically treated for symptomatic frontoethmoidal osteomas. Four were located in the frontal sinus, two in the anterior ethmoid and one in the anterior and posterior ethmoid and sphenoid. Five were treated by endonasal approach with endoscopes and two with osteoplastic technique without frontal sinus obliteration. Symptoms improved in all patients.
Surgery was a very effective treatment to resolve the symptoms caused by frontoethmoid osteomas.
The endonasal approach with endoscopes is of choice to treat ethmoidal osteomas. In frontal osteomas, the total occupation of the sinus, the lateral location, and the extensive implantation are factors to consider in the choice of external approaches, although they do not exclude the indication of an extended endonasal approach with the cavitation technique or a combined approach.
Osteoma, Frontal, Ethmoid, Endoscopic surgery, Lothrop modified
Osteomas are benign, slow-growing tumors that originate in the paranasal sinuses, mainly in the frontal and ethmoid sinuses. Most are asymptomatic and are diagnosed based on imaging findings. When they produce symptoms, treatment is surgical and the approach depends mainly on the location and size of the tumor. The surgical approach can be external, endonasal with endoscopes or combined.
To determine the efficacy of surgery to resect symptomatic frontoethmoidal osteomas, and to establish the factors that could facilitate an endonasal approach with endoscopes.
Descriptive and retrospective study.
All patients who were surgically treated for osteomas located in the ethmoid and frontal sinuses between August 2007 and June 2021 in the Rhinosinusology section of the Otorhinolaryngology service of the Hospital Italiano de Buenos Aires were included.
All the operated patients had symptoms caused by the bone neoplasm. Those who suffered from craniofacial pain consulted neurology prior to surgery to rule out other types of headaches.
They were evaluated by nasal endoscopy and computed tomography without contrast (CT). A measurement of the size of the osteoma was performed on the tomography and the extension and its possible implantation (Chiu classification) were analyzed (Table 1).
Table 1: Classification of frontal osteomas according to extension and implantation. View Table 1
The surgical technique varied according to the paranasal sinus involved, the location within the sinus, and the size of the tumor. In ethmoid osteomas, an endonasal approach was performed with endoscopes. An anterior ethmoidectomy was performed and the osteomas were resected and in another the osteoma was drilled to reduce its size. In frontal osteomas, an endonasal approach was performed with endoscopes (Draf II-a, and Lothrop modified technique) and osteoplastic surgery without obliteration. All patients were hospitalized for 24 hours and there were no complications. Controls were performed by nasal endoscopy and computed tomography.
Seven patients were surgically treated for symptomatic frontoethmoidal osteomas. Five were women and two men, the average age was 48 years. Two were located in the ethmoids and had an approximate size of 0.8 × 0.9 mm, and another involved the ethmoid and sphenoid (Figure 1 and Figure 2). The symptoms they produced were headache (2/3) and unilateral nasal obstruction (1/3).
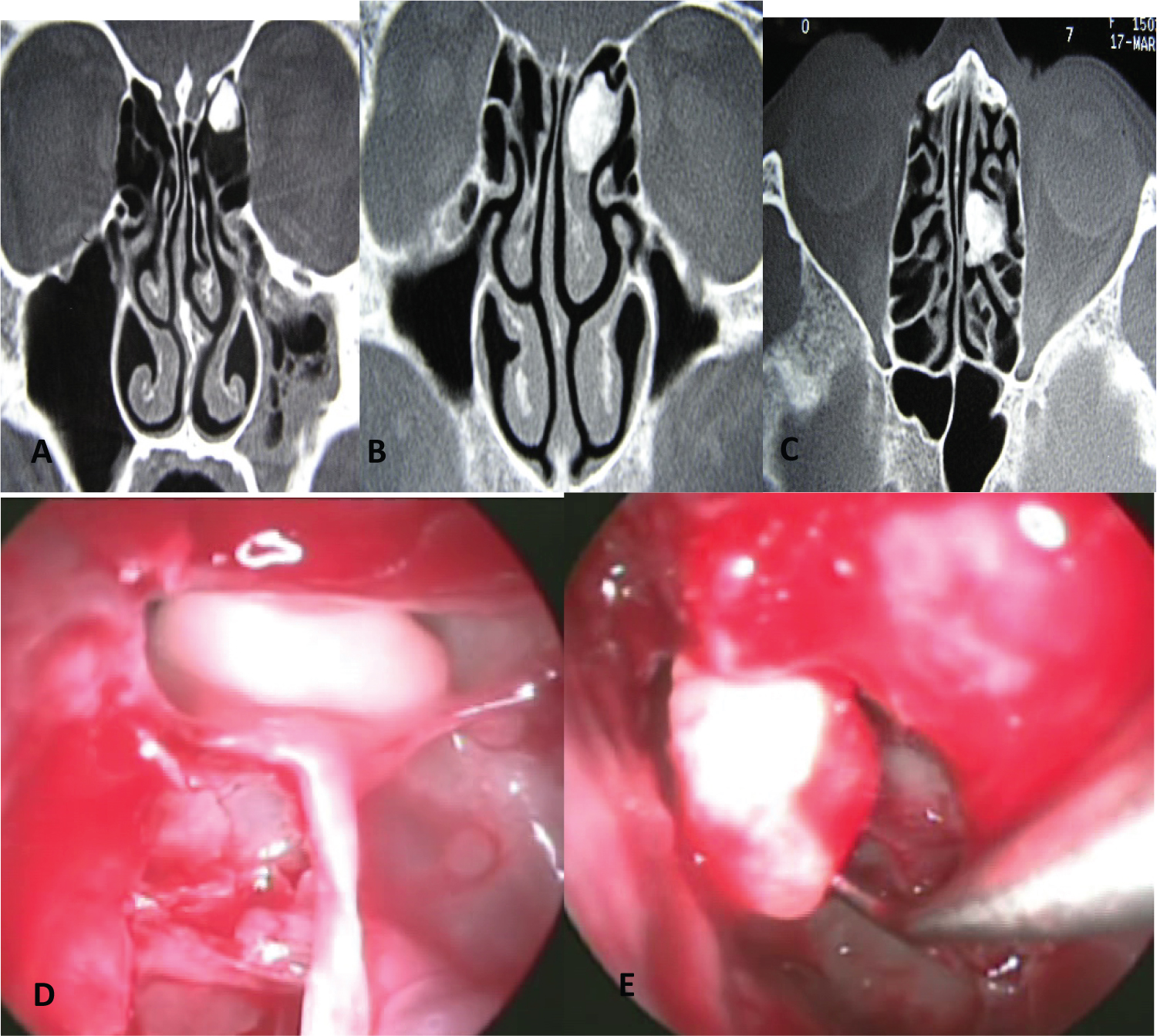 Figure 1: Ethmoid Osteoma: (A, B, C) Computed tomography; (D, E) Endoscopic vision: Anterior ethmoidectomy and resección of osteoma.
View Figure 1
Figure 1: Ethmoid Osteoma: (A, B, C) Computed tomography; (D, E) Endoscopic vision: Anterior ethmoidectomy and resección of osteoma.
View Figure 1
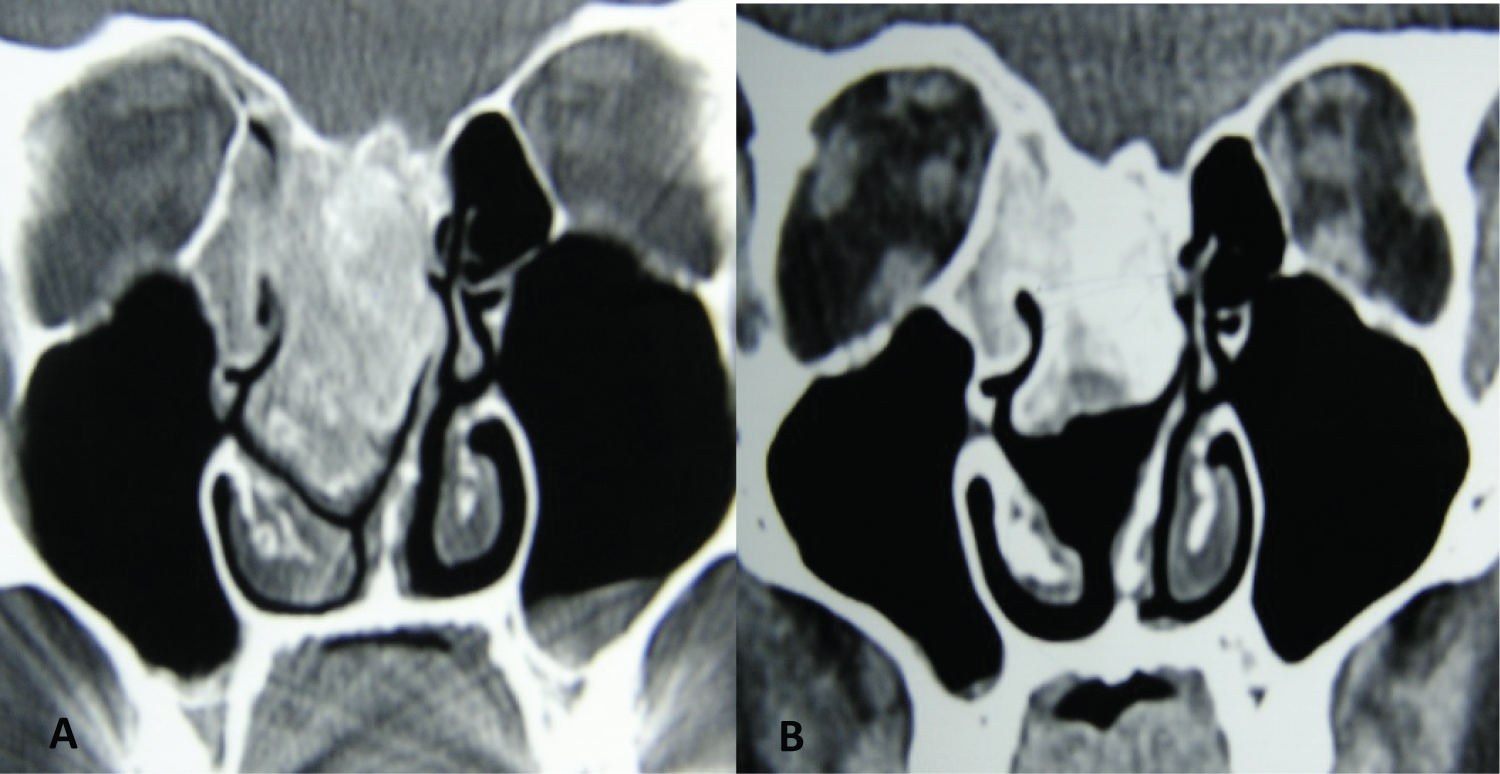 Figure 2: Ethmoid-sphenoid osteoma that produced right nasal obstruction as the only symptom. A) Computed tomography; B) Postoperative computed tomography showing a reduction in the size after drilling the osteoma.
View Figure 2
Figure 2: Ethmoid-sphenoid osteoma that produced right nasal obstruction as the only symptom. A) Computed tomography; B) Postoperative computed tomography showing a reduction in the size after drilling the osteoma.
View Figure 2
Four were located in the frontal sinus. One in the recess blocking the drainage ostium, another in the medial sector of the frontal sinus reaching the superior wall, and two compromised a frontal hemisinus (from the medial to the lateral wall).
The size of the tumors was: 10 mm (height) × 10 mm (width), 39.28 mm (height) × 25.68 mm (width), 29 mm × 43 mm and 31 mm × 37 mm.
According to the extension (Chiu classification: Table 1), there was one grade I and three grade III osteomas (Figure 3 and Figure 4).
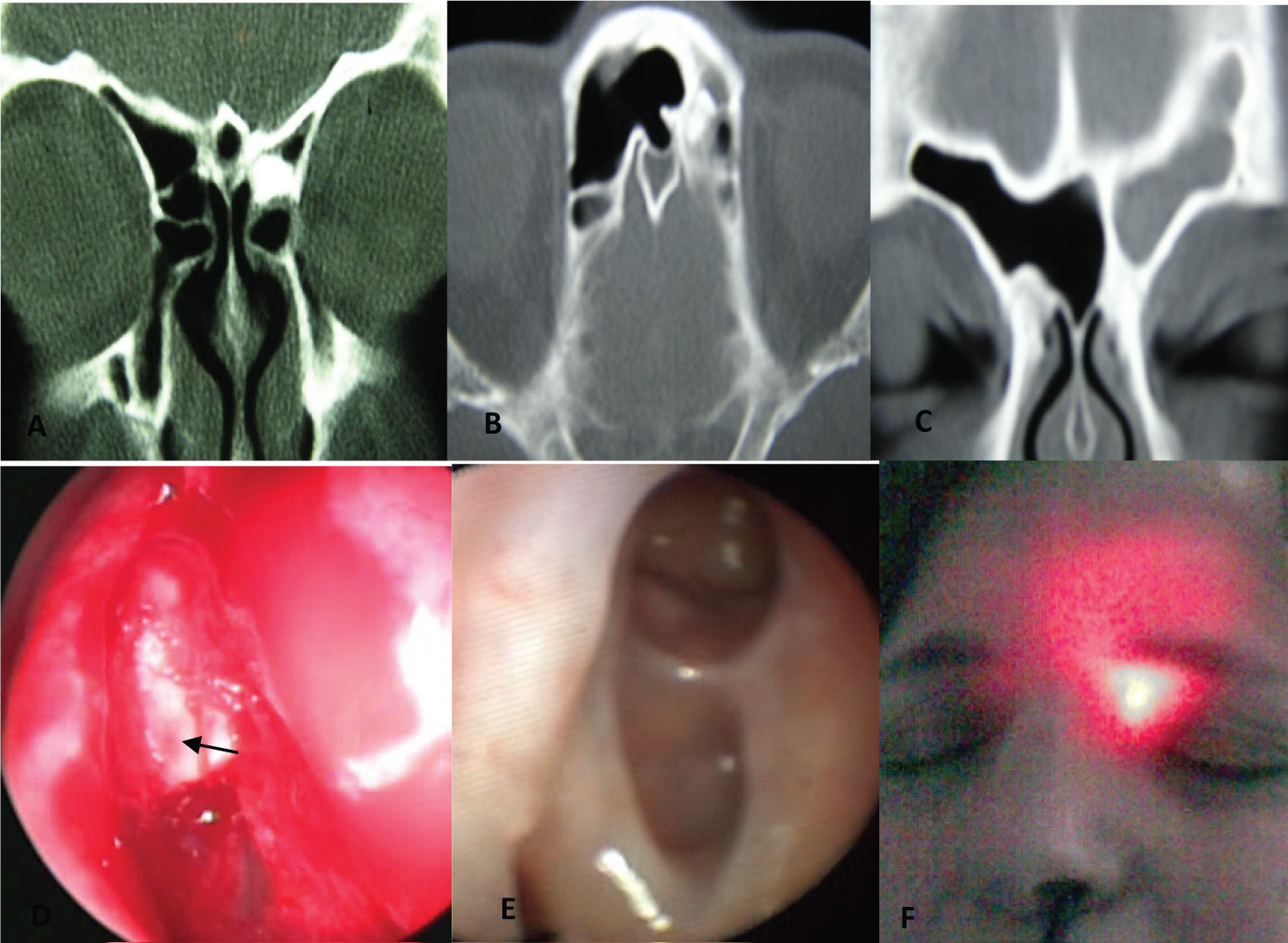 Figure 3: A, B, C) Osteoma located in the frontal recess causing sinusitis; D) Endoscopic view of osteoma (arrow); E) Postoperative endoscopic vision of frontal drainage; F) Postoperative frontal sinus transillumination.
View Figure 3
Figure 3: A, B, C) Osteoma located in the frontal recess causing sinusitis; D) Endoscopic view of osteoma (arrow); E) Postoperative endoscopic vision of frontal drainage; F) Postoperative frontal sinus transillumination.
View Figure 3
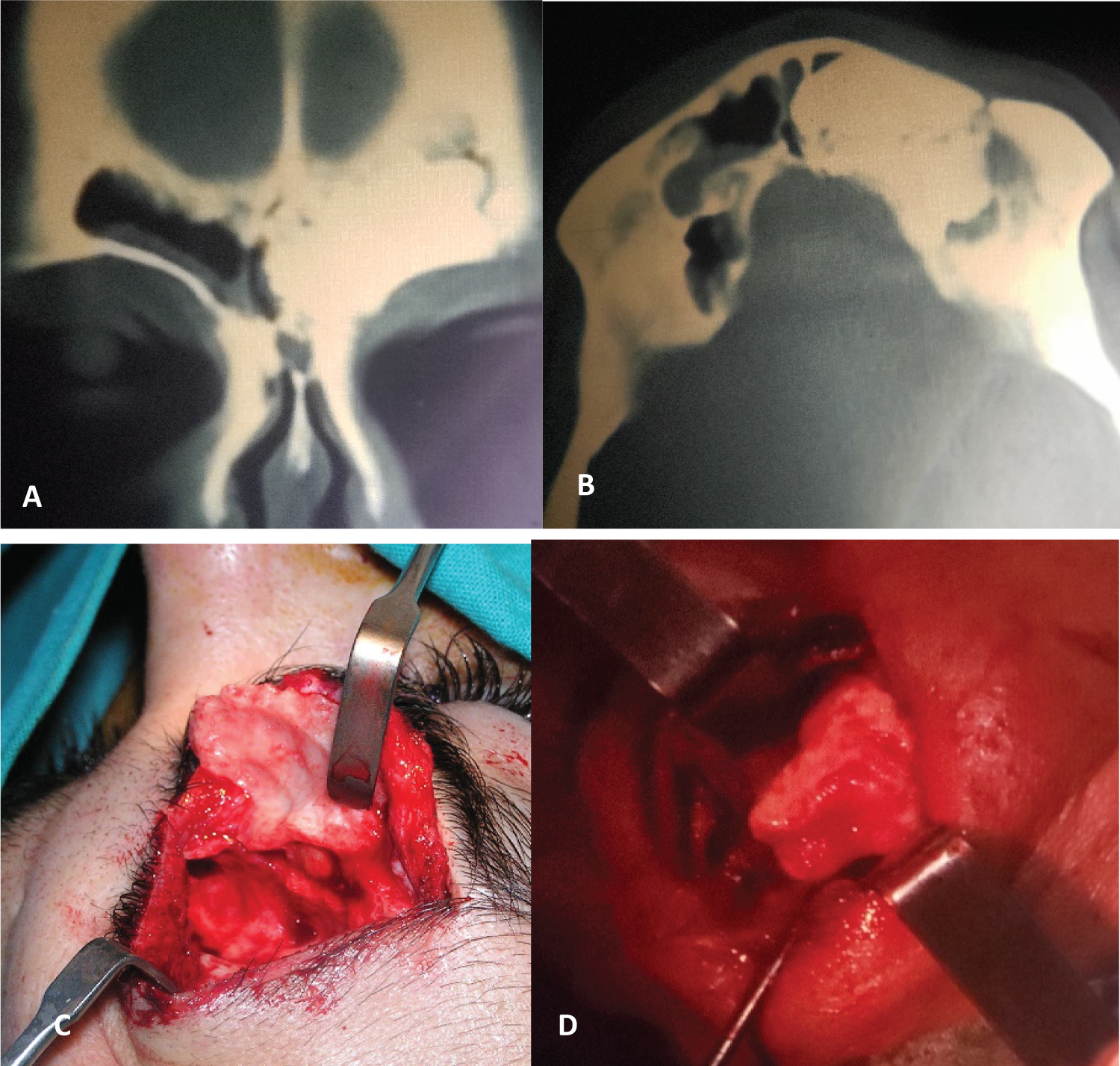 Figure 4: A, B) Computed tomography showing extensive left frontal osteoma; C) Osteoplastic surgery without obliteration; D) Osteoma resection.
View Figure 4
Figure 4: A, B) Computed tomography showing extensive left frontal osteoma; C) Osteoplastic surgery without obliteration; D) Osteoma resection.
View Figure 4
The symptoms they caused were: Recurrent sinusitis due to blockage of the ostium (1/4) and headache (3/4). In two osteomas that compromised the anterior ethmoid, a complete resection was performed.In another osteoma that compromised the anterior and posterior ethmoid and sphenoid, affecting the base of the skull, the tumor was reduced through an endonasal approach to improve the nasal obstruction.
The frontal osteomas were completely resected in three patients and in another in whom a modified Lothrop was performed, the exeresis was subtotal, leaving a residual lesion of approximately 15% of the original size of the tumor (Figure 5).
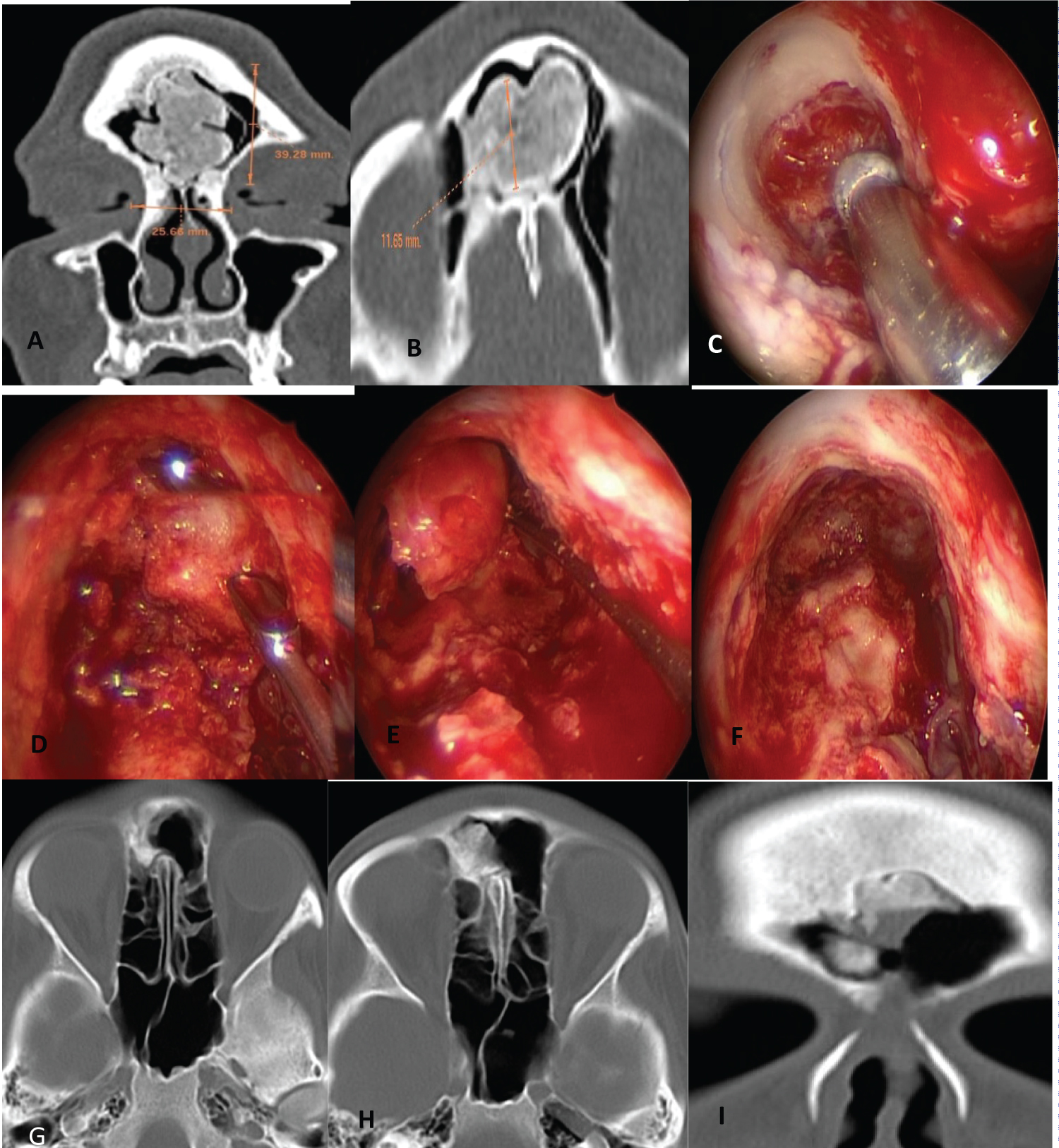 Figure 5: (A, B) Computed tomography showing extensive frontal osteoma; (C) Lothrop modified and osteoma milling; (D, E) Fragmentation and resection of the osteoma; (F) Modified Lothrop: Endoscopic vision after resecting the osteoma; (G, H) Postoperative axial computed tomography; (I) Postoperative coronal computed tomography where residual lesion is observed.
View Figure 5
Figure 5: (A, B) Computed tomography showing extensive frontal osteoma; (C) Lothrop modified and osteoma milling; (D, E) Fragmentation and resection of the osteoma; (F) Modified Lothrop: Endoscopic vision after resecting the osteoma; (G, H) Postoperative axial computed tomography; (I) Postoperative coronal computed tomography where residual lesion is observed.
View Figure 5
Symptoms improved in all patients. Postoperative controls for an average of 2 years did not show recurrences and in osteomas that were partially resected no tumor growth was diagnosed (Table 2).
Table 2: Patients treated for fronto-ethmoid osteomas. View Table 2
Most osteomas located in the frontal and ethmoid sinuses are asymptomatic. The appearance of signs and symptoms depends on the location, size and direction of growth of the tumor. Progressive headache and chronic sinusitis caused by blockage of the frontal sinus drainage ostium are the most common symptoms. The incidence of headache varies between 52 to 100% [1].
In our series, six of seven patients had headache, one of them due to recurrent sinusitis due to frontal drainage obstruction.
Complications can occur if the osteoma extends into the orbit, involves the base of the skull, or obstructs the sinus drainage ostium.
Asymptomatic osteomas can be controlled, except when they occupy more than 50% of the size of the sinus, grow rapidly (more than 1 mm per year), have intracranial or orbital involvement, or block the drainage ostia of the frontal or sphenoid sinus. Some of these indications for surgery are controversial [2].
The goal of surgery treatment is to resect the osteoma without damaging adjacent structures, to resolve the symptoms that affect patients.
For some, the main objective of surgery is the complete resection of the osteoma, others affirm that a partial excision leaving a residual peripheral sector of the tumor may be sufficient without significantly increasing of the rate of recurrence [3].
This last concept is based on the fact that the osteoma initially grows from the center and the bone matures progressively towards the periphery, resecting the center of the tumor would stop growth.
In the patient with sphenoid ethmoid osteoma who underwent partial resection to improve nasal obstruction, no residual tumor growth was detected during follow-up.
The choice of surgical approach will depend on the involved sinus, location within the sinus, size of the osteoma, sector or sectors of implantation, extension to the orbit or skull base, histological appearance inferred from CT (compact, spongy or mixed) and the experience of the surgical team.
Chiu, et al. [4] established a surgical algorithm based on the classification of frontal sinus osteomas that takes into consideration the implantation zone, the location in relation to a virtual line that passes through the lamina papyracea, and the size of the osteoma in relation to the anteroposterior diameter of the frontal sinus (Table 1).
According to this classification, they indicate in grade I osteomas an endonasal endoscopic surgery, in grade II an extended or combined approach to the frontal sinus, and in grade III-IV an osteoplastic technique without obliteration or with obliteration if there was an extensivemucosal resection or the patient had multiple surgeries for chronic sinusitis.
Others consider that the size and location of the osteoma is not relevant to indicate the surgical approach, since the possibility of performing a cavitation and/or fragmentation technique would allow endonasal resection [5].
In our study, a small osteoma that occupied the frontal recess could be resected by a Draf II-a endonasal approach without inconvenience.
In two patients with giant osteomas (greater than 30 mm), an osteoplastic approach was performed due to the laterality of the tumors and because they were operated on in the first years of the beginning of this series, when we had less experience in extended endonasal frontal sinusapproaches.
In the last giant frontal osteoma that we treated with surgery (2021), we performed a modified Lothrop technique with cavitation and fragmentation of the tumor.We resect approximately 85% of the size of the tumor and completely improving the headache that was the reason for which the patient consulted.
The use of equipment with piezoelectric systems that generate a vibration transmitted to the tip of the equipment can facilitate the fragmentation of tumors and their resection through the endonasal route [6].
The tomographic characteristics of osteomascan sometimes make it possible to infer the compact or spongy nature of the osteoma, this latter would facilitate the endonasal resection using the cavitation or fragmentation technique.
In our case series, 6 osteomas were compact and one was mixed. The implantation of the osteoma in the frontal sinus detected in the preoperative tomography may be an important factor in determining the degree of difficulty in resecting the tumor endonasally.
In the two osteomas operated through an external approach the implantation site was extensive.One was implanted in the floor, anterior and posterior wall, and the other in the floor of the frontal sinus.
In another treated using an endonasal approach with the modified Lothrop technique, the tumor was implanted in the posterior superior wall.
The external approaches that may be indicated to treat ethmoidal osteomas are the paralateronasal or the Lynch type and in the frontal sinus the subciliary, transpalpebral, bipalpebroglabellar or bicoronal approach (osteomas with involvement of the entire frontal sinus) with an osteoplastic technique without obliteration.
We believe that even if an osteoplastic approach is performed, the frontal sinus should not be obliterated.In case of excessive damage to the mucosa it is preferable to combine the external approach with an endonasal approach (Draf II - III) to enlarge the endonasal sinus drainage.
Endonasal surgery with endoscopes using the Draf II or Lothrop technique is useful in giant frontal osteomas, using the cavitation and fragmentation techniques.
Seiberling, et al. [7] described 23 patients with frontal osteomas, who were treated by an endonasal approach with endoscopes. Eight were staged grade IV, 6 grade III and the rest grade I and II.
In 15 they performed a modified Lothrop, in one they also did a transorbital approach through a blepharoplasty-type incision (extension to the orbit) and in another a frontal trephination at the level of the eyebrow. In the remaining patients, they performed a frontal endonasal sinusotomy associated with a minitrephination.
In cases where the osteoma was attached to the skull base without a defined dissection plane, a residual margin of peripheral tumor was left to avoid penetrating the endocranium (in 4 patients, between 5-10% of the osteoma was left attached to the skull base). They had no recurrences.
In a systematic review published in 2019, they included 32 studies with 477 patients treated with surgery for frontal osteomas since 1990. In 214 (45%) the approach was transnasal with endoscopes, in 176 (37%) they made an external approach with osteoplastic technique and in 87 (18%) a combined approach [8].
Comparing by decade, there was less indication of osteoplastic approaches alone or combined in 2010 compared to 1990.
Implantation of the osteoma in the floor of the frontal sinus (roof of the orbit) was the main predictor they found for performing an external approach followed by extrasinus extension.
In another systematic review, they described a greater indication for external approaches (59.8%), followed by endonasal approaches with endoscopes (25%) and then by the combined ones (11.5%). They also reported a significant growth in the indication for endonasal surgery with endoscopes since 2015 (49.3%) compared to the years 1995-1999 (6.3%).
According to the extension (Chiu classification), of 69 grade I-II frontal osteomas, 1.4% were treated by an external approach, 14.5% by a combined technique, and 84.1% by an endonasal approach with endoscopes. Of 86 grade III - IV osteomas, 18.6% were treated externally, 34.9% by combined technique and 46.5% by endoscopic surgery [9].
Surgery was a very effective treatment to resolve the symptoms caused by frontoethmoid osteomas. The endonasal approach with endoscopes is of choice to treat ethmoidal osteomas. In frontal osteomas, the total occupation of the sinus, the lateral location, and the extensive implantation are factors to consider in the choice of external approaches, although they do not exclude the indication of an extended endonasal approach with the cavitation technique or a combined approach.
The authors have no conflicts of interest to declare.