Microcystic adnexal carcinoma (MAC) is a rare cutaneous neoplasm with a predilection for growth in the centrofacial region. It usually presents as a unifocal lesion with indolent but invasive growth patterns.
A 39-year-old male presented with multifocal MAC of the head and neck, which had been gradually increasing in size over 10-15 years. Wide local excision was performed with a total surgical defect of 430 cm2. An anterolateral thigh fasciocutaneous free flap and cervicofacial advancement flap were used to reconstruct the defect. The patient received adjuvant external beam radiotherapy (EBRT) and later underwent flap revision and contracture scar release for cosmetic corrections.
No recurrence has been detected during an 18-month follow-up period.
We demonstrate a case of rare multifocal MAC with atypically extensive surface area of involvement, successfully treated with wide local excision combined with EBRT, and flap reconstruction.
Microcystic adnexal carcinoma
Microcystic adnexal carcinoma (MAC) is a rare cutaneous neoplasm with an indolent but locally invasive growth pattern and predilection for growth in the centrofacial region [1]. We report a rare case of multifocal MAC of the face, scalp, and axilla, successfully treated with excision and free flap reconstruction followed by adjuvant external beam radiation therapy (EBRT). Full institutional review board committee approval obtained.
A 39-year-old male was referred to the Otolaryngology clinic from Dermatology for several cutaneous head and neck lesions which had been persistent for the past 10-15 years and slowly increasing in size. Previous biopsies at an outside institution showed infiltrating poorly-differentiated carcinoma with ductal formation of the left forehead (6 × 3 cm) and left lower face (7 × 3 cm), and MAC of the right forehead (2.5 × 1.8 cm) (Figure 1). Three more ill-defined erythematous indurated plaques were noted on the right chin (3 × 4 cm), left temporoparietal scalp (8 × 4 cm), and left axilla (3 × 2 cm). Biopsies were taken at these three sites, which revealed MAC. These lesions were associated with occasional itching but no pain. Additionally, the patient had a right temple lesion that was initially misdiagnosed as basal cell carcinoma. The patient works as a delivery driver, with no history of radiation or family history of cancer. PET CT confirmed no metastatic lymphadenopathy or distant metastases.
 Figure 1: Microcystic adnexal carcinoma at the time of pre-operative assessment.
View Figure 1
Figure 1: Microcystic adnexal carcinoma at the time of pre-operative assessment.
View Figure 1
Wide local excision was undertaken with margins advanced until peripheral frozen sections were negative for tumor. A left neck dissection was also performed given the need for vessel exposure for free flap reconstruction. The total forehead and scalp defect measured 27 × 10 cm and lower face defect measured 8 × 20 cm. A right anterolateral thigh (ALT) fasciocutaneous free flap was used to reconstruct the large forehead and scalp defect, and a cervicofacial advancement flapwas used to reconstruct the lower facial defect (Figure 2). The axillary defect was closed primarily. The right temple lesion was excised with clear margins and closed primarily by Dermatology 1 month later.
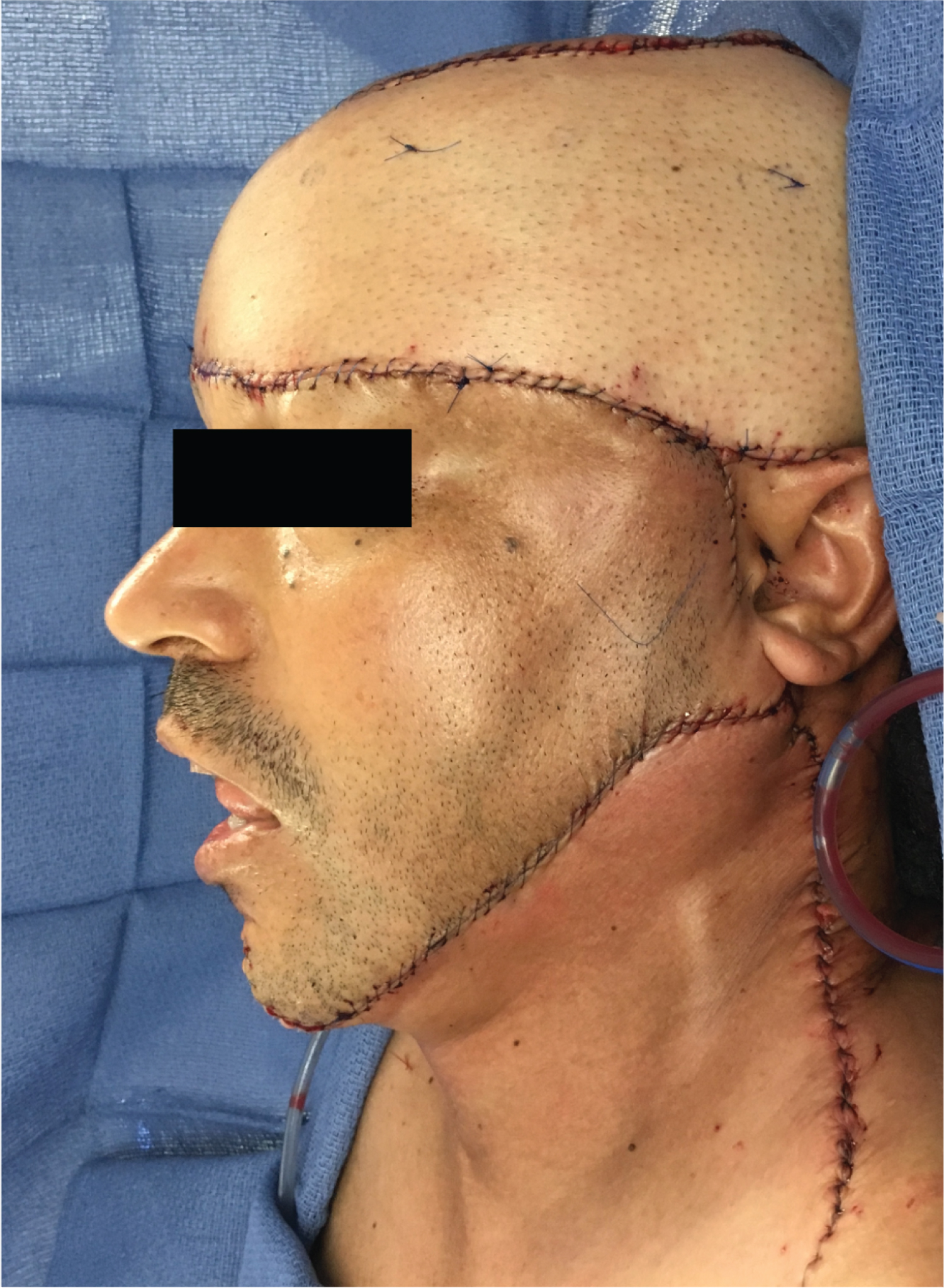 Figure 2: Following wide local excision with reconstruction via anterolateral thigh (ALT) fasciocutaneous free flap and cervicofacial advancement flap.
View Figure 2
Figure 2: Following wide local excision with reconstruction via anterolateral thigh (ALT) fasciocutaneous free flap and cervicofacial advancement flap.
View Figure 2
Histopathological analyses of the permanent sections confirmed the diagnoses of MAC and revealed evidence of perineural invasion (PNI) and positive tumor margins. All lymph nodes were negative for tumor. Adjuvant external beam radiotherapy (EBRT) to the left face, right forehead, and left axilla of 54 Gy was administered in 27 fractions.
During post-operative evaluation, the patient was noted to have a right lower lip contracture scar with eversion asymmetry as well as ptosis of the left brow and auricle caused by the weight of the flap. As such, three months following EBRT, the patient was taken for right lower lip contracture scar release and bi-pedicled flap advancement and ALT flap revision.
The patient has exhibited no signs or symptoms of recurrence during an 18-month follow-up period, with repeat clinical examination and CT every 3-months during the first year and every 6-months during the second year.
MAC was first characterized by Goldstein, et al. as a cutaneous neoplasm originating from pluripotential adnexal keratinocytes [2]. MAC demonstrates an indolent growth pattern with a long latency period usually between 1 to 11 years. Although only a few isolated cases of metastases have been reported, MAC demonstrates aggressive local infiltration and PNI, which has been reported in 41.8% of cases [3]. The surface area of pathologic involvement is, on average, four-fold that of the clinically apparent lesion [4]. This is consistent with our patient who had an estimated 93.5 cm 2 of involvement clinically, but total surgical defect of 430 cm 2 .
The presented case is notable for its multifocal nature, with seven primary lesions, unusually extensive surface area, and atypical involvement of the axilla. An estimated 80% of MAC lesions present in the head or neck [5]. To our knowledge, only one previous case of multifocal MAC has been reported. Recent systematic review of 55 studies found a mean lesion diameter of 2.8 cm. Lesion size has been directly correlated with likelihood of recurrence, with an 11% increased risk for every 1-cm increase in size [3].
Risk factors for MAC are unknown. Proposed factors include immunosuppression, radiotherapy, genetics, and UV exposure [3]. Although the role of UV exposure has been controversial, the presented patient’s occupation as a delivery driver in the absence of other identifiable risk factors and extensive lesions, points to UV radiation as a likely contributing factor.
No funding or conflicts of interest for any of the authors.
None.
Ms. Hanqing Shang: Chart review, manuscript production; Dr. Mica Glaun: Chart review, manuscript production; Dr. David Hernandez: Primary physician caring for the patient described herein and provided appropriate edits for the piece.