Nutritional status of patients with rheumatoid arthritis (RA) is often poor. In addition, popular trends in avoiding certain foods have been noted among patients with RA yet recent data on dietary intake is lacking. The aim of the present study was to examine possible differences in food intake between Swedish women with and without RA. In total 150 women with RA, selected from the Swedish Rheumatology Quality Register, and 163 women without RA, answered a postal food frequency questionnaire includsing questions on 45 food items, food choices, age, weight, height, educational level and serious illness. Women with RA consumed red meat and nuts less frequently and did not eat any butter/margarine on sandwiches or chose low fat varieties to a higher extent than women without RA. Background characteristics differed between the groups and were adjusted for in the analyses. To conclude, habits of women with RA differ to some extent from that of women without the disease; most importantly many women with RA exclude red meat. Future studies should include meal patterns and amounts of food consumed to obtain a wider, more accurate understanding of food consumption patterns of women with RA and to link this with concurrent disease activity.
Rheumatoid arthritis, Dietary habits, Sweden, Red meat
Rheumatoid arthritis (RA) is a common inflammatory joint disease that is more frequent in rich societies and affects more women than men [1]. No cure exists for RA although pharmacological treatment may diminish disease progression and symptoms. Despite a tremendously improved treatment, including biologics, the last decades, a substantial number of patients do not reach remission, and some suffer from side effects, which leads to a search for alternative remedies such as dietary treatments [2].
The nutritional status and dietary intake of patients with RA are reportedly poor although recent data are lacking [3-6]. Few dietary intervention studies that could guide improved intake have been carried out and the ones that exist are dated; many having been performed in the 1980-1990s when less effective pharmacological treatments were in use. Fish oil or dietary n-3 PUFA, in addition to treatment with disease-modifying antirheumatic drugs (DMARD) have been reported to increase the number of successful and continued DMARD treatments, indicating that pharmacological and dietary treatment complement each other [7,8] and thus diet could be an important part of the treatment. Data from observational studies indicate that a Mediterranean diet might be beneficial for patients with RA [9]. A systematic review from 2009 concluded that a Cretan Mediterranean diet may alleviate pain but did not seem to improve physical function or decrease stiffness. The review also concluded that seven to ten days of fasting followed by a vegetarian diet could have the same effect [10]. Unfortunately, the scientific evidence, from few and diverse dietary interventions, are insufficient to reinforce specific dietary advices for patients with RA.
Despite the lack of specific dietary recommendations, many patients with RA believe that diet is a contributing factor to their disease and on their own alter dietary habits after diagnosis [11]. For example, in a survey in USA, asking patients with RA if certain food made their symptoms better, worse or unchanged, 24% responded positively to the question. Among these 15% reported improvements and 19% worsening and most of the patients avoided some food [12]. This underscores the need for up to date knowledge of habitual diets of patients with RA.
Approximately 75% of all patients with RA are women. Physicians have noted that women with RA tend to exclude a variety of foods, although it is unclear if they do so to a larger extent than women without RA. Since patients with RA have an increased risk for cardiovascular diseases, it is even more important that they have a healthy diet. In addition, it is of importance in the clinical practice to know about dietary trends among the patients, since avoidance of specific foods can have an important impact on nutritional status and overall health.
The aim of the present study was to examine possible differences in dietary intake between Swedish women with and without RA and to identify potential variations in the women's intakes of fruit and vegetables, red meat, seafood, fat quality and foods with limited nutritional values such as sweets, ice cream, snacks and pastries.
This population-based cross-sectional study compares habitual food intake of women with and without RA, using data from a self-administered food frequency questionnaire (FFQ), with an addition of questions regarding food choices and background information such as age, weight, height, educational level and serious illness such as RA.
The coded FFQs were posted with an information letter, a form for signed informed consent and a prepaid return envelope. An option existed to answer the questionnaire online. No incentives were used to increase participation.
In May 2015, 678 women with RA living in the Västra Götaland Region, Sweden, between 25-65 years old and with a disease duration of > two years (to avoid temporary changes in diet in newly diagnosed patients), were identified from the Swedish Rheumatology Quality Register (SRQ). Among these, 428 women living in Gothenburg or nearby postal areas and not participating in other studies were invited with a postal letter.
A random sample of 800 women aged 25-65 and living in the Gothenburg area, was selected from the Swedish State Personal Address Registry (SPAR) in February 2016. Of these 407 were matched by postal area to the sample of women with RA and they were invited by postal letter to participate. The only inclusion criteria for the control group (women without RA) was female sex and postal code matching the women with RA. A preliminary analysis showed that the women without RA had a significantly higher educational level than the sample of women with RA. In an attempt to get more similar education level in both groups, the remaining 210 women living in selected areas with a low mean monthly income (< 25 000 SEK) were invited. In total, 428 women with RA and 617 without RA were invited to the study. The recruitment process is shown in Figure 1.
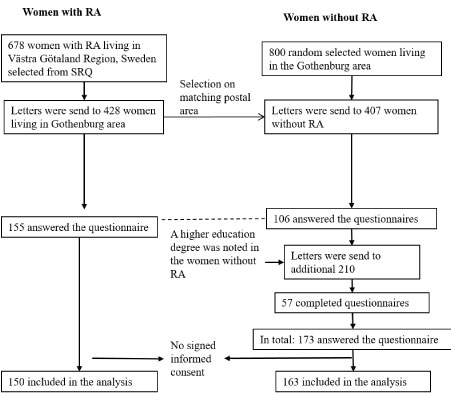 Figure 1: Flow chart of the study.
Figure 1: Flow chart of the study.
RA: Rheumatoid arthritis; SRQ: Swedish Rheumatology Quality Register. View Figure 1
The FFQ included questions on food choices and intake frequencies of 45 food items (Supplementary File) and was available in Swedish only. The FFQ was twelve pages long and took 15-30 minutes to complete. To cover seasonal variation, participants were asked to answer the questions with the last twelve months in mind. The six intake-frequency options ranged from "less than once per month or never" to "three times per day or more". Additionally, the FFQ included an open-ended question where the respondent was asked if she avoided any food items for other reasons than allergies or intolerances.
The FFQ was an adjusted version of a validated FFQ from the Swedish National Food Agency, specifically developed to be used in public health surveys as indicator of diet quality and physical activity [13]. To make the questionnaire less extensive and easier for the respondents, the number of options for intake frequency was reduced from fourteen to six in the present study. Questions about processed meat, nuts and whole grains were added to enable examination of healthy eating habits according to the latest Swedish dietary advice [14].
Differences in background characteristics between women with and without RA are, due to skewed distribution in the variables, presented as median and interquartile range and tested with Mann-Whitney U tests. Body mass index (BMI) was calculated as kg/m2 and classified according to WHO [15]. Categorical data were analysed with Chi2 tests and Fisher's exact test.
Multivariable linear regression was used to evaluate differences in consumption patterns between groups, to allow adjusting for confounders. Here, intake frequency data were transformed into continuous variables. The frequency 1-2 times per week was coded as 1.5 times per week; "once a month or less" as 0 intakes and "3 times per day or more" as 3 times per day. Age, BMI and education were evaluated as confounders. All variables were log-transformed before used in the regression models.
Answers to open ended questions such as "What food allergies or intolerances do you have?", "What foods do you not eat?", "Do you have any illness besides from RA?" and "Do you avoid any foods because of your illness?" were categorised by the most common replies and new dichotomous variables were created. Answers to the question "What foods do you not eat" that gave an impression of being due to personal taste such as liver, offal and sushi or specific single foods with no explanation given were not analysed. In the few cases when a participant had inappropriately answered with more than one response for a food, that specific answer was disregarded and labelled as a missing value. All statistical analyses were carried out in SPSS Statistics 22 (IBM) and P-values < 0.05 were considered significant.
A total of 155 women with RA and 173 women without RA answered the FFQ, resulting in a response rate of 36% (155/428) and 28% (173/617) respectively. The FFQ was answered by 15 women who had not signed the consent form and who were therefore excluded. Hence, in the final analysis 150 women with and 163 women without RA were included.
Background characteristics of the participating women are shown in Table 1. Statistically significant differences were seen in age, education and BMI, where the women with RA were reportedly slightly older and had a higher weight and BMI (Table 1). Also, the women with RA reported a higher degree of other illnesses besides RA and women without RA more often stated that they had a university education. No significant difference was seen in the use of nicotine.
Table 1: Background characteristics of a sample of Swedish women with and without rheumatoid arthritis. View Table 1
Response rates from the different postal areas were compared between groups and there were no overall differences between the women with and the women without RA (P = 0.376). Analysis using only postal areas with more than ten individuals in the initial sample selection showed that the postal area Angered, a suburb to Gothenburg with a high proportion of foreign-born inhabitants, had the lowest response rate (13%).
No significant differences were seen in fruit and vegetable intake between women with RA and in women without RA (Table 2). A compiled variable for the intake frequencies of root vegetables, legumes, vegetables, fruit and berries showed that 16% of women with RA and 19% of women without RA consumed fruit and vegetables five times a day or more (Figure 2a).
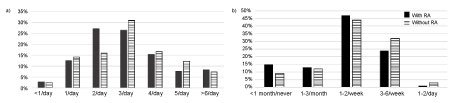 Figure 2: a) Daily intake of fruit and vegetables including root vegetables, legumes, vegetables and fruit and berries of Swedish women with (n = 144) and without rheumatoid arthritis (n = 163) (P = 0.966, adjusted for age, education and BMI). b) Intake frequencies of red meat by Swedish women with (n = 150) and without rheumatoid arthritis (n = 163) (P = 0.001 adjusted for age, education and BMI). View Figure 2
Figure 2: a) Daily intake of fruit and vegetables including root vegetables, legumes, vegetables and fruit and berries of Swedish women with (n = 144) and without rheumatoid arthritis (n = 163) (P = 0.966, adjusted for age, education and BMI). b) Intake frequencies of red meat by Swedish women with (n = 150) and without rheumatoid arthritis (n = 163) (P = 0.001 adjusted for age, education and BMI). View Figure 2
Table 2: Intake frequencies of different foods based on a sample of Swedish women with and without rheumatoid arthritis. View Table 2
Analyses of consumption of red meat showed significant differences between the groups when adjusted for age, BMI and education (P = 0.001). Women with RA reported eating red meat less frequently than women without RA: 15% of women said that they ate red meat as part of a main meal less than once a month or never compared to 9% in without RA (Figure 2b). No differences were seen in reported intake frequencies of chicken, or processed meats such as charcuteries or hamburgers, sausages and kebab (Table 2).
Choice of spreadable fat differed between the two groups (Figure 3) (P = 0.032). Women without RA chose butter and margarine blends with a fat content of 70-80% to a higher extent than women with RA, where more women chose low fat options or did not use any spreadable fat. Both groups were similar in their choices of cooking fat. More women with RA answered that they typically chose low fat milk (16% in the RA-group, 8% in the control group) and low-fat yoghurt (29% in the RA-group, 18% in the control group); the differences were however not significant.
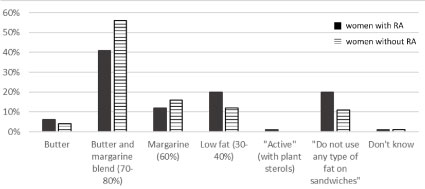 Figure 3: Type of spreadable fat typically used on sandwiches by Swedish women with (n = 143) and without rheumatoid arthritis (n = 161) (P = 0.032). View Figure 3
Figure 3: Type of spreadable fat typically used on sandwiches by Swedish women with (n = 143) and without rheumatoid arthritis (n = 161) (P = 0.032). View Figure 3
More women with RA reported a low intake (less than once a month or never) of nuts and seeds compared to the control group, 21% and 9% respectively (Table 2). Furthermore, only 12% of the women with RA said that they ate nuts or seeds daily in comparison with the women without RA where 25% stated the same. The differences in nut and seed intake were statistically significant also when adjusted for education (P = 0.029).
The intake frequencies of seafood were similar in both groups. Most women in both groups reported fish or shellfish intake twice a week or more (with RA = 50%, without RA = 56%). By contrast 28% of the women with RA and 24% of the women without RA answered that they consumed seafood less than once a week.
Women with RA reported eating foods with limited nutritional value (i.e. sweets and chocolate, ice cream, snacks and pastries) "less than once a month or never" to a higher extent than women without RA (Figure 4). The differences in intake frequencies were however not statistically significant.
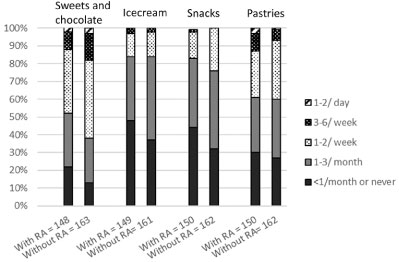 Figure 4: Intake frequencies of foods with limited nutritional value by Swedish women with and without rheumatoid arthritis (Sweets and chocolate P = 0.0118 adjusted for age and education. Ice cream P = 0.359 adjusted for age, education and BMI. Snacks P = 0.388 adjusted for age and education. Pastries P = 0.559 adjusted for age, education and BMI). View Figure 4
Figure 4: Intake frequencies of foods with limited nutritional value by Swedish women with and without rheumatoid arthritis (Sweets and chocolate P = 0.0118 adjusted for age and education. Ice cream P = 0.359 adjusted for age, education and BMI. Snacks P = 0.388 adjusted for age and education. Pastries P = 0.559 adjusted for age, education and BMI). View Figure 4
The proportion of women who stated that there were certain food items or food groups they excluded from their diet did not differ significantly between groups. Approximately one third of the women in both groups declared foods they did not eat. Red meat was the most common food group to exclude and significantly more women with RA claimed to exclude or avoid red meat than women without RA (25% in women with RA and 12% in women without RA) (P = 0.002). Other foods/food groups listed were gluten (5% in both groups), sugar (women with RA = 3% and women without RA = 4%) and milk/dairy products (women with RA = 4% and women without RA = 3%).
The primary aim of this study was to examine possible differences in reported dietary intake between women with and without RA. The main finding was that women with RA tended to report consuming less red meat than those without the disease. Other differences were that women with RA either did not consume any butter/margarine on sandwiches, or chose low fat varieties to a higher extent than women without RA. The women with RA also reported a less frequent intake of nuts and seeds. These results suggest that women with RA, as a group, do indeed eat differently than other women. Previous studies, which did not find any differences in diets, have focused primarily on energy- and protein-intake [16,17] and not on specific foods and food groups as this study aimed to do. Existing information on what women with RA consume is limited and our findings are important for future nutrition interventions and in clinical practice.
The finding that women with RA report consuming less red meat is in line with a study of diets among Finnish women with RA, where the most common dietary change was reduced intake of meat, sausages and fatty foods [11]. Moreover, 20% of women in a Swedish study on patients with RA claimed to follow a Mediterranean-like diet [18]; one of the characteristics being a low consumption of meat. Studies investigating the effect of elimination of red meat in patients with RA have reached contradictory conclusions [19]. Thus, it would be interesting to learn whether the women experience a reduction of symptoms by doing so, or if they consume less meat because they simply assume it is beneficial to them, because of data from the few uncontrolled studies on vegan diet in patients with RA [19,20]. Concerns have been raised as indications of a reduction of lean body mass were seen in a study where the intervention group fasted and thereafter followed a vegetarian diet [19]. No optimal amount of protein intake has been identified for patients with RA, even though it has been suggested that supplementation of amino acids could be advantageous in treatment of rheumatoid cachexia [21]. Although a reduced intake of red meat, along with processed meat, is recommended to the general population [14], this may have negative consequences if done without consideration of diet quality especially for patients with RA, as meat is an excellent source of amino acids.
Women with RA in our study, more often chose low fat dairy products, or reported that they did not consume the food in question, to a higher extent than did women without RA and reported a significantly less frequent consumption of nuts and seeds. This could be interpreted as more women with RA avoid fatty foods, possibly in an attempt to eat healthily and maintain their weight. These results are also in line with the Finnish study [11].
Most women in Sweden eat some type of vegetable and fruits and berries 2-4 times per day [22]. These numbers are comparable with the findings of the present study. In both groups, few women reported consuming fruits and vegetables five times per day or more, similar to a Swedish study from 2008 where less than one in ten consumed this amount. No significant differences were seen between the groups, which differs somewhat from the results from an American study [23,24] that found that healthy controls ate slightly more fruit than women with RA.
Fish and seafood consumption were high in both groups, with over 50% of the women eating fish at least twice a week. The corresponding proportion for Swedish women [22] is 31%. An explanation for the much higher intake frequencies in our study might be that Gothenburg is a coastal town with a tradition of eating fish.
A tendency to report fewer intakes of foods with limited nutritional value was seen amongst the women with RA, which was unexpected as their BMI was higher than that of the group of women without RA; a higher BMI often is associated with higher intakes of sugary and energy-dense foods [25,26]. These results could be due to differences in portion size, resulting in different amounts of consumed energy. Another explanation could be the lower total energy expenditure [27] in patients with RA with a lower dietary energy requirement as a consequence, forcing them to avoid energy-dense food not to gain weight. A third explanation could be that the women with RA under-reported more than did the control women. The higher BMI in the RA-group were anticipated as these are characteristic for this patient group. This was also true for the difference in educational level since low formal education has been associated with an increased risk of RA [28,29]. However, since the reported educational level of the RA-group in the present study was not lower than the population in general, it is likely that the educational level was higher in both study groups than in the source population they represent [28].
High BMI, low socio-economic status, psychological conditions and higher age are all factors that influencing under-/over reporting and eating habits [22,30,31]. Thus, in the current analyses, age, BMI and education were evaluated as confounders and adjusted for in regression models when applicable. Additional strengths of this study include the use of a validated instrument, a relatively high response rate and a large number of participants in both groups. Women with RA were selected from a population-based high-quality register and control women were matched on area of residence.
A limitation of this study is that the current disease activity of the women with RA, both responders and non-responders, was unknown. It is reasonable to believe that women with very high disease activity or who have comorbidities have lower response rates and have greater difficulties with food-related tasks such as shopping, preparing and cooking food, influencing their diet. In addition, a non-response analysis was not possible to perform as no background characteristics are known for those not answering the FFQ.
The results of this study suggest that reported dietary habits of women with RA differ from women who do not have the disease: The most important difference being that many women with RA exclude red meat from their diets. Future studies examining dietary habits of women with RA should include meal patterns and amounts of food consumed to obtain a wider and more accurate understanding of how women with RA eat and to link this with concurrent disease activity.
We would like to thank all the women who responded to the questionnaire and also Linnea Bärebring for her help with distributing the questionnaires.
This work was supported by grants from the Swedish government under the ALF agreement (grant numberALFGBG-716341) to author AW.
KNS, HL and AW designed the study. HL and IG was involved in the selection of patients. KNS send out the questionnaire, collected all the data and made statistical analysis. KNS interpreted the data and wrote the manuscript in collaboration with AW, IG and HL. HL and AW are the guarantors of the study.
The authors declare no conflict of interest.
Supplementary File: Content of the Food Frequency Questionnaire. Frequencies, foods and specific questions included in the questionnaire.