The aim of this study is to evaluate the transaminases capacity in predicting the adverse outcomes of preeclampsia.
This study was carried out among women hospitalized in Department of Obstetrics and Gynecology and intensive care unit at maternity university hospital between January 2013 and June 2015. We have compared the group of eclampsia with preeclampsia control group, each case (eclamptic woman) was matched to a control (preeclamptic woman), a ratio of 1/1. Transaminases levels were compared in the two groups (cases and controls).
58 cases of eclampsia were observed during the study period, corresponding to a rate of 7.9 per 10,000 births. Transaminases levels were higher among eclamptic women compared to women with preeclampsia, respectively 107.10 U/L and 28.2 U/L for ALT, and 171.75 U/L and 30.12 U/L for AST (p = 0.01 and p = 0.008).
ALT area under the ROC curve was 0.718 (CI 95%: 0.62-0.81). For a sensitivity of 74% and a specificity of 66%, the best threshold value was 57 U/L. While for AST the area under the ROC curve was 0.716 (CI 95%: 0.61-0.82), the best threshold value was 59 U/l, with a sensitivity of 76% and a specificity of 57%.
Transaminases levels were significantly higher during eclampsia compared with preeclampsia. This is a clinically useful way to predict the adverse outcomes of preeclampsia. However, a prospective study is necessary to develop a clinical prediction model of eclampsia.
Preeclampsia, Eclampsia, Transaminases, ROC curve
Eclampsia is characterized clinically by hypertension, edema, proteinuria, and seizures in women during the second half of pregnancy or in the immediate postpartum period. The pathophysiology remains unclear [1-4]. One proposed mechanism is that cerebral vasospasm induced by severe hypertension results in ischemia and consequent cytotoxic edema. This is supported by angiographic findings of diffuse or focal vasospasm and by infarctions in some patients [1,2,5].
The prevalence of eclampsia in developing countries ranges from 1/2000 to 1/3448 [6,7]. In Morocco, it is 3.6% [8]. It is one of the 3 leading causes of maternal morbidity and mortality worldwide [9].
It is associated with an increased risk of maternal mortality in developed countries (0%-1.8%) [10,11]. The mortality rate is as high as 15% in developing countries [12,13].
The efforts to predict preeclampsia did not allow its prevention [14]. That is why we focused on disease progression of preeclampsia to eclampsia.
The management of preeclamptic and eclamptic women often includes the determination of some biochemical parameters exploring liver function such as transaminases (AST and ALT).
However, the contribution of modifications of biochemical values in the prediction of complications among women with preeclampsia is not yet elucidated.
In this study, we try to assess the ability of transaminases in predicting adverse outcomes of preeclampsia. The identification of threshold values (Cut-off value) of these two biochemical tests commonly asked in routine can help improve the management of pregnancy-induced hypertension.
Data for this study was drawn from the records of 116 pregnant women hospitalized between January 2013 and June 2015, for preeclampsia or eclampsia in department of obstetrics and gynecology and maternal intensive care unit of the university hospital.
A case-control study was carried out by comparing two groups of patients. The "case-group" (58 eclamptic women). Eclampsia was defined by the occurrence of one or more generalized epileptic seizures. Were excluded from this group woman with other causes of seizures, such as epilepsy, meningitis, tumor or brain hemorrhage.
The "control group" (58 women) was comprised of preeclamptic patients. Preeclampsia was defined by systolic blood pressure of more than 140 mmHg and diastolic blood pressure of more than 90 mmHg after 20 weeks' gestation in a previously normotensive patient, new-onset proteinuria (> 300 mg of protein in a 24-hour urine collection or a random urine protein/creatinine ratio of > 0.3), and resolution of hypertension and proteinuria by 12 weeks postpartum [15,16].
Each case (eclamptic woman) was matched to a control (preeclamptic woman), a ratio of 1/1. The transaminases values (AST, ALT) measured on admission to obstetrics and gynecology department or maternal intensive care unit were collected from patient records. These parameters were analysed by a Cobas Integra 400+ biochemical analyser (Roche Diagnostics GmbH).The averages of the two liver enzymes (AST, ALT) were compared in the two groups (cases and controls).
The Kolmogorov-Smirnov test was used to test for normal distribution. Student's unpaired t-test was used for the comparison. The interest of the dosage of these parameters in predicting the occurrence of eclampsia was evaluated by the ROC curve (Receiver Operating Characteristic). It was obtained from the results of the various threshold values; the area under the curve was also calculated. The statistical significance was set at p < 0.05 and statistical Package for the Social Sciences (SPSS for Windows, version 10.1) was used for all statistical analysis.
Women's age ranged from 16-43 years with an average of 27.9 years (SD = 7.6). The average age of preeclamptic women was 28.9 years (min = 16; max = 43; SD = 7.4). The one of eclamptic women was 27 years (min = 18; max = 43; SD = 7.7). The difference of the average ages of the two groups (pre-eclampsia and eclampsia) were not significant (t-test = 1.16; p = 0.25).
Our study shows that from a total of 73,000 births, the rate of eclampsia during the study period was 7.9 per 10,000 births.
For the average value of transaminases in the case group (eclamptic women), it was significantly higher than the control group (preeclamptic women) Table 1.
Table 1: Comparison of transaminases average in both groups (eclamptic vs. preeclamptic). View Table 1
Furthermore, ALT area under the ROC curve was 0.718 (CI 95%: 0.62-0.81). For a sensitivity of 74% and a specificity of 66%, the best threshold value was 57 U/L. While for AST the area under the ROC curve was 0.716 (CI 95%: 0.61-0.82), the best threshold value was 59 U/l, with a sensitivity of 76% and a specificity of 57% Figure 1.
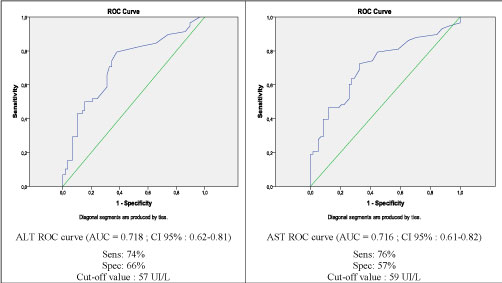 Figure 1: Performance of ALT and AST in predicting eclampsia using ROC Curve.
View Figure 1
Figure 1: Performance of ALT and AST in predicting eclampsia using ROC Curve.
View Figure 1
In this study, the ALT level of eclamptic women was significantly higher than that of preeclamptic ones (p = 0.01).
During eclampsia, there are areas of ischemia and subcapsular hemorrhage in liver. Various hepatic changes include hemorrhage which explains ALT elevation.
Also, our study showed that the AST level of eclamptic women was significantly higher than that of preeclamptic women (p = 0.008). In their study, Von Dadelszen, et al. [17] observed increased AST level in eclamptic women compared to the preeclamptic ones. Also Salem, et al. [14] found that an AST level greater than 30 U/L was more frequently observed in eclamptic women, compared with women with preeclampsia. The areas under the curve of ALT and AST were respectively 0.718 (0.62 to 0.81) and 0.716 (0.61 to 0.82).
Our results corroborate those of Von Dadelszen, et al. [17], which recorded the following values 0.72 (0.66 to 0.78) and 0.73 (0.67 to 0.79) respectively for ALT and AST.
However, research on the ability of biochemical parameters for the prediction of the evolution of preeclampsia remains mixed. Indeed, some studies have shown a strong association between AST and ALT level and adverse outcomes of preeclampsia, but no consensus has been established on the reproducibility of the predictive value of these biochemical parameters [18,19].
Some authors believe that AST is more predictive because they reflect the multiple organ dysfunction [20,21]. The ALT reflects the tissue damage and liver dysfunction.
The pathophysiology of eclampsia still unclear and it is difficult to determine risk factors. This study showed that high levels of transaminases increased significantly during eclampsia compared to preeclampsia. We believe that this is an inexpensive useful in predicting the outcome of preeclampsia. However more studies are necessary to verify the reproducibility of the results.
The authors declare that they have no competing interests.
We thank the Health authority of Marrakesh which allowed us to carry out this work.