Traumatic injuries account for 9.6% of the global burden of disease, they represent the third most common cause of death in young adults and adolescents among patients admitted to hospital facilities; penetrating abdominal trauma remains an important cause of mortality and morbidity [1]. This type of lesions can cause vascular injuries that are associated with massive hemorrhage and could develop physiologic exhaustion, resulting in high reported mortality [2]. Inferior's cava injuries secondary to penetrating trauma are rare, accounting for approximately 0.02% of gunshot wounds to the abdomen [3]. Surgical treatments for this type of lesions represents one of the most difficult challenges with high complications rate, including infections of the graft and vascular dehiscence; a timely and accurate surgical intervention in hands of experienced surgeons is crucial for better results in their management [4].
A 26-year-old male patient was admitted to the emergency room after receiving four gunshots; the first one was in the neck, penetrating through the submental region exiting at the level of the right labial commissure of the mouth. The second gunshot was in the thorax, with an entry wound in the left hemithorax at second intercostal space precisely in middle clavicular line level, with an exit wound in the axillary region. The third was on the right hemithorax with an entry orifice located in the fifth intercostal space posterior axillary line level, with exit orifice located on the fourth intercostal space clavicular middle line level. And the fourth impact was on the abdominal region, passing through the left hypochondrium without exit wound.
At its initial assessment the patient presented tachycardia (135 bpm), hypotension (90/60 mmHg) and tachypnea (25 bpm); crystalloid solutions were administrated (Hartmann 1000 cc solution); physical examination revealed well ventilated lungs, present heart sounds and pain at soft palpation of the abdomen with muscular resistance, based on the clinical data obtained and without the need of another type of study or instrumental examination it is taken to the operating room in a period no longer than 10 minutes since the admission.
Exploratory laparotomy was executed finding 3000 ml of hemoperitoneum, with grade IV lesions in mesentery and small intestine at 180, 280, 290, 310, 330 cm from Treitz angle of the retroperitoneal hematoma (zone I); retroperitoneum was accessed finding a lesion on the lateral side of the inferior vena cava of approximately 3 cm (Figure 1); vascular control of right and left iliac veins was performed as well as vena cava, proper reconstruction was performed with prolene 6-0 continuous suture (Figure 2), followed by intestinal resection with anastomosis at 180 cm and another intestinal anastomosis at 280 cm; an open drainage is placed located at the surgical bed and a right endopleural catheter was placed obtaining 50 cc serohematic fluid.
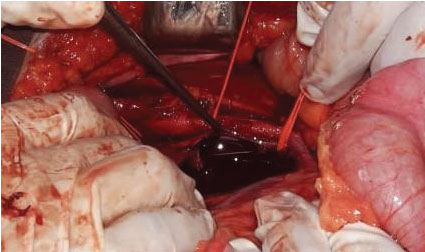 Figure 1: Lateral vena cava injury of approximately 3 cm. View Figure 1
Figure 1: Lateral vena cava injury of approximately 3 cm. View Figure 1
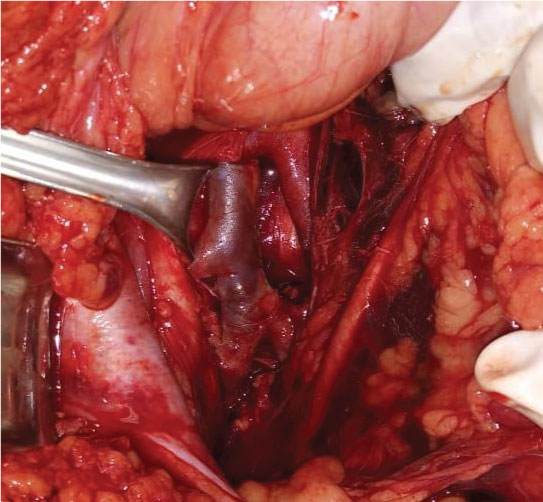 Figure 2: Inferior vena cava reconstruction with continuous 6-0 prolene suture. View Figure 2
Figure 2: Inferior vena cava reconstruction with continuous 6-0 prolene suture. View Figure 2
On his second post-operative day a Facial tomography was requested, finding fracture of the lower jaw. The patient evolved favorably, we start oral nutrition and removed the open drainage on the third day, also recanalized and evacuation present at fourth day. The surgical repair of the jaw fracture was performed at 6th postoperative day; he was discharged after 8 days of hospitalization.
Abdominal vascular injuries are associated with a high mortality/morbidity rate representing a challenge for vascular and emergency surgeons. Proper and prompt management requires early diagnosis; surgical intervention in hands of an experienced surgeon with advance knowledge of the retroperitoneal anatomy and of the surgical approaches to access these vessels is crucial. The immediate dissection and reconstruction of damages vessels prevents rapid loss of blood. Despite the complex approach and anatomy of the great retroperitoneal vessels, in the hands of an expert surgeon, survival is possible.