Tuberculosis continues to pose a substantial burden on global health, with a substantial number of individuals affected by the disease worldwide. Skeletal tuberculosis, although less common, represents a significant subset of tuberculosis cases, comprising approximately 10% of those with active tuberculosis. This case report aims to describe a rare instance of isolated skeletal tuberculosis, where the diagnosis was made histologically, despite the absence of systemic tuberculosis symptoms.
Pott's disease, Spondylodesis, Tuberculous spinal surgery, Tuberculous spondylitis, Vertebral tuberculosis radiography
Tuberculosis, one of the oldest known infectious diseases, has left its mark on human history. Evidence of spinal tuberculosis is found in the spinal deformities of mummies dating back to 9000 B.C. [1]. Among the various types of tuberculous lesions of the spine, Pott's spinal disease (tuberculous spondylitis) is the most common, accounting for about 60% of cases [2]. The lower thoracic spine and upper lumbar spine are affected in about 19% of affected individuals [3,4].
Spinal tuberculosis usually arises from hematogenous spread of pulmonary tuberculosis but may manifest independently in certain cases [3,5]. Diagnosis and treatment of patients with spinal tuberculosis is a major challenge in clinical practice. Clinical presentations can be varied, and paradoxical exacerbations are not uncommon [6]. While the latter is frequently discussed in the literature, there remains a paucity of information on primary spinal cord tuberculosis, warranting further investigation.
A 62-year-old female patient presented with persistent, dull, aching back pain accompanied by right-sided radiculopathy. A comprehensive general examination and laboratory tests yielded unremarkable results, and no significant underlying medical conditions were documented. After the initial clinical suspicion of disc herniation, a magnetic resonance imaging (MRI) was performed, which revealed a 33 × 32 mm lesion on the L4-L5 vertebra that was invading the right nerve root and exerting pressure on the spinal cord (Figure 1). After obtaining explicit informed consent, a surgical procedure was carefully planned and performed.
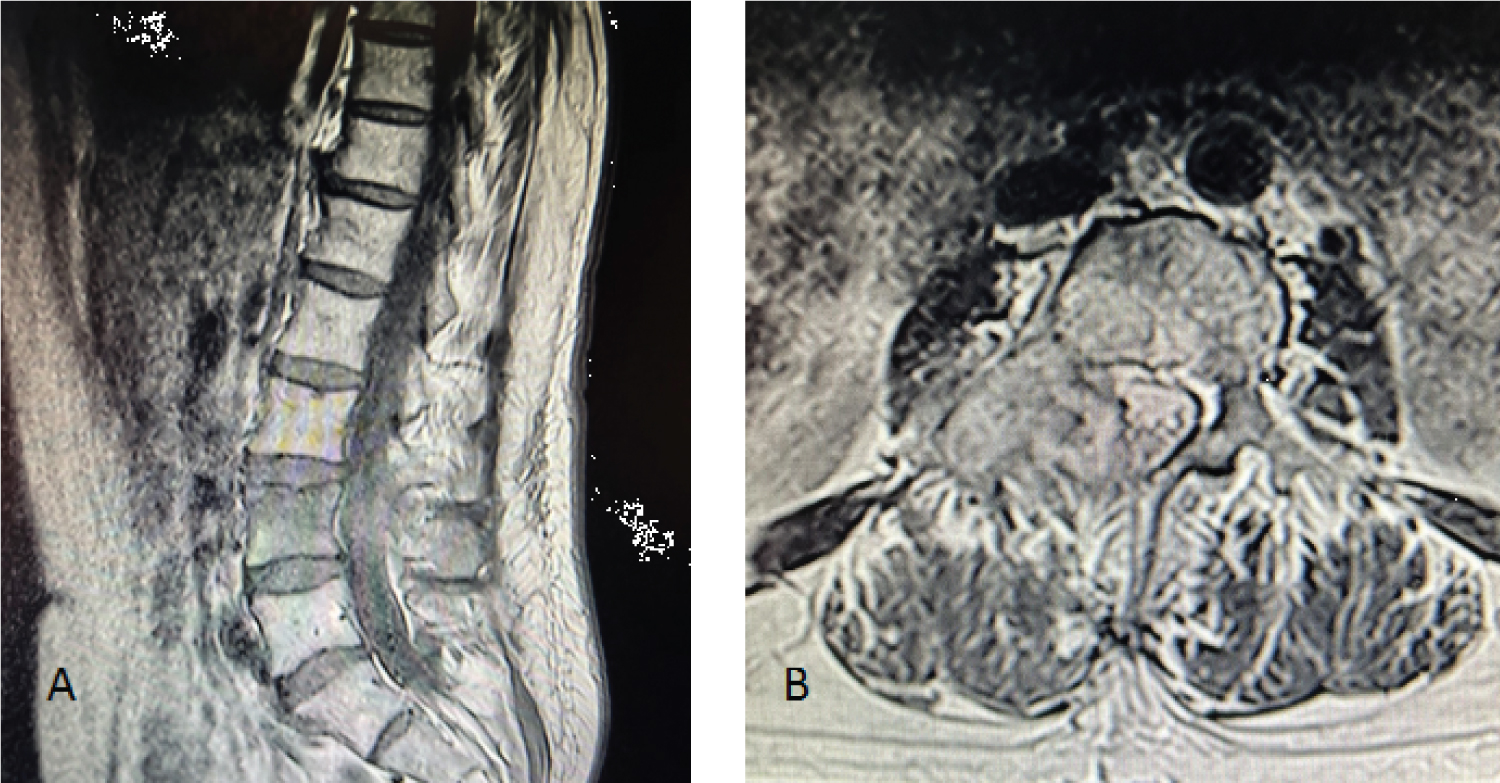 Figure 1: (A & B) Magnetic resonance imaging of the lumbosacral spine revealed a hypointense 33 × 32 mmextramedullary expanding lesion at L4-L5 level compressing the right spinal nerve root as well as the spinal cord.
View Figure 1
Figure 1: (A & B) Magnetic resonance imaging of the lumbosacral spine revealed a hypointense 33 × 32 mmextramedullary expanding lesion at L4-L5 level compressing the right spinal nerve root as well as the spinal cord.
View Figure 1
During the surgical procedure, the lesion was removed and harvested for subsequent histological analysis. As part of the patient's treatment protocol, a spondylodesis was performed from L2 to L5 (Figure 2). Postoperatively, the patient showed progressive improvement in her clinical condition. Histologic examination revealed a granulomatous formation with central caseation which was consistent with tuberculoma (Figure 3).
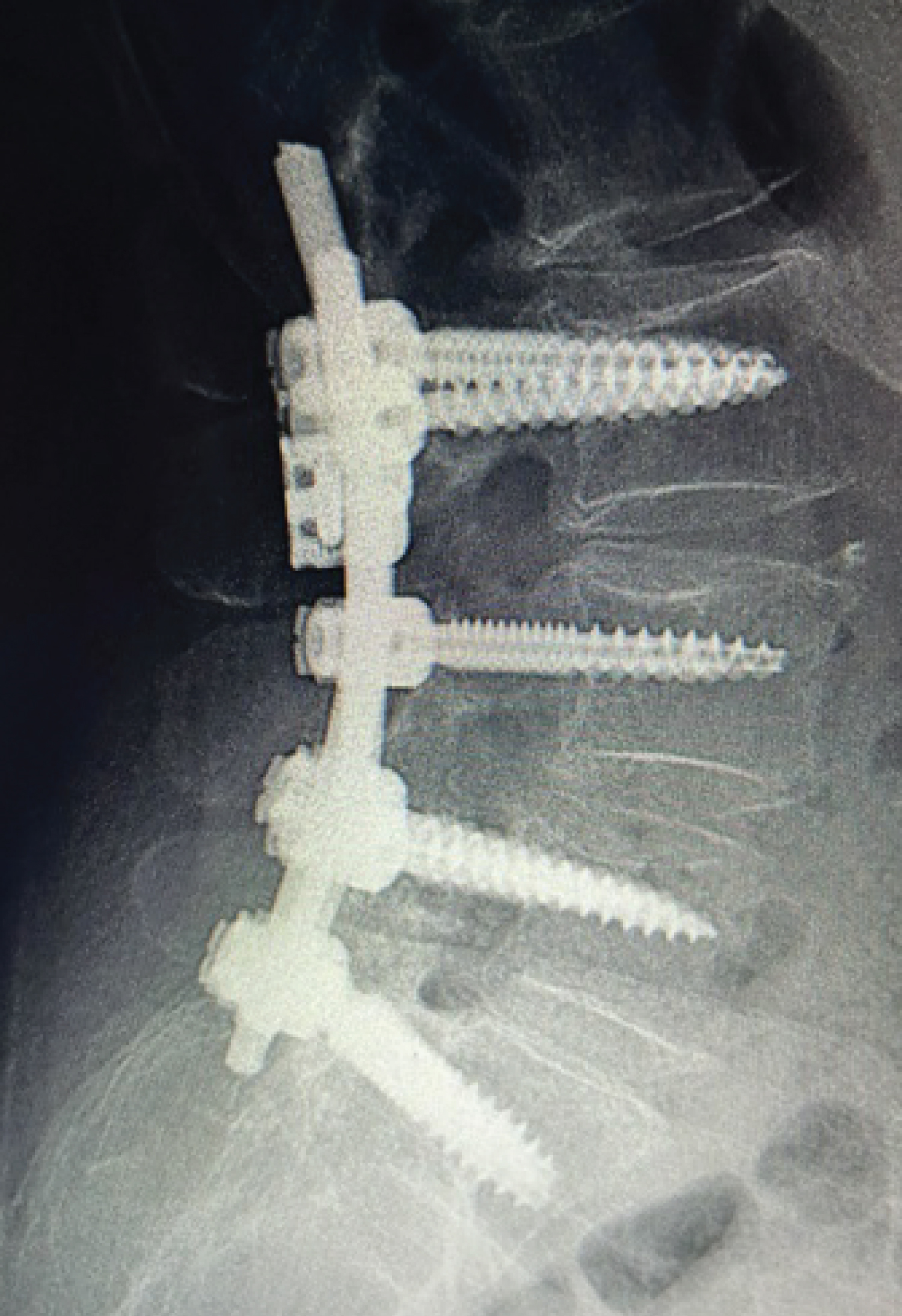 Figure 2: Post-operative lateral view X-ray illustrating successful L2-L5 spondylodesis.
View Figure 2
Figure 2: Post-operative lateral view X-ray illustrating successful L2-L5 spondylodesis.
View Figure 2
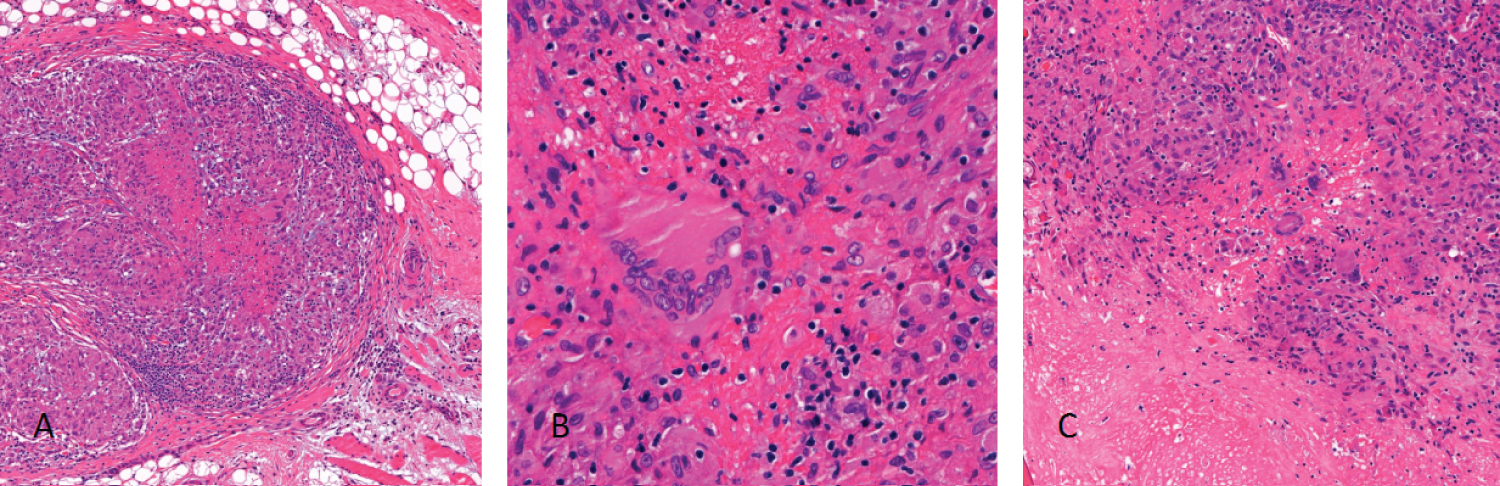 Figure 3: (A) Histology revealed characteristic granulomas in bone and soft tissue with a central necrotic area surrounded by epitheloid histiocytes; (B) Among the histiocytes the typical multinucleated giant cells, with peripherally arranged nuclei (so-called Langerhans’ giant cells) were present; (C) The bone showed areas of necrosis (left) in direct association with the granulomas (right).
View Figure 3
Figure 3: (A) Histology revealed characteristic granulomas in bone and soft tissue with a central necrotic area surrounded by epitheloid histiocytes; (B) Among the histiocytes the typical multinucleated giant cells, with peripherally arranged nuclei (so-called Langerhans’ giant cells) were present; (C) The bone showed areas of necrosis (left) in direct association with the granulomas (right).
View Figure 3
Spinal tuberculosis, a pathological condition often originating within the anterior subchondral region of the vertebral body adjacent to the intervertebral disc while typically exhibiting limited involvement of the posterior elements, has the potential to extend directly into the intervertebral disc and spread through subligamentous pathways to neighboring levels [2,7]. Notably, the development of paravertebral abscess formations is a frequently observed manifestation [7]. Among the affected regions, the thoracic spine stands as the most commonly affected site [8].
Dissemination of spinal tuberculosis can transpire either through arterial dissemination within the paradiscal region or via the Batson's paravertebral plexus, an intricate valveless venous plexus, which allows access into the central vertebral body [1]. If the condition is allowed to progress untreated, the consequential outcomes can encompass destruction of the anterior vertebral body and subsequent development of kyphosis, underlining the potential severity of this ailment [1,9].
Back pain is a predominant complaint that occurs in majority of patients with spinal tuberculosis (between 90% and 100%) [1,7,10]. The characteristic clinical profile includes a gradual and insidious onset of back pain accompanied by stiffness, local tenderness, and sporadic episodes of fever [1]. Complications such as cord compression, paresis, paresthesia, cauda equina syndrome and paralysis can also occur [2,7,11].
Radiographic manifestations of spinal tuberculosis typically manifest in the later stages of the disease, necessitating the destruction of over 50% of trabecular bone before becoming evident on radiographs [12,13]. These radiological characteristics include a constellation of findings, comprising intervertebral disc space narrowing, irregularities and erosion of adjacent endplates, sequestrae formation, as well as the presence of paravertebral body masses [7]. Variations from conventional imaging may also occur, such as cases in which only the central portion of a vertebral body is affected without involving the intervertebral disc [7,10].
Recognition of spinal cord involvement in the setting of tuberculous meningitis (TBM) is paramount because of the serious complications that result [6]. Timely and accurate identification of spinal tuberculosis remains essential as it serves as a critical measure to prevent the potential progression of these complicated complications.
This case report highlights the complicated diagnostic difficulties in identifying spinal tuberculoma, especially when the patient has no history of active tuberculosis. Rapid recognition and careful performance of diagnostic tests play a critical role in revealing the underlying lesion and subsequently determining the appropriate treatment.
Although tuberculous spondylitis is a rare neurosurgical condition, it should be included in the spectrum of differential diagnoses for spinal cord compression, even in the absence of obvious evidence of extramural tuberculosis. The present case underscores the pivotal role of histologic diagnosis in isolated vertebral lesions without concomitant evidence of systemic tuberculosis. Timely recognition and prompt treatment of such cases is critical to ensure favorable patient outcomes and to prevent progression of potential complications.