Osteoblastoma is a locally aggressive, osteogenic primary bone tumor primarily affecting the axial skeleton that is known to produce a local inflammatory response surrounding the tumor. This effect, known as the flare phenomenon, has been described primarily for its implications on imaging and diagnosis of osteoblastoma. The main aim of this report is to present an unusual case of osteoblastoma of the posterior ilium associated with unilateral sacroiliac joint ankylosis and chronic right-sided sciatica, which was complicated by intractable pain, tachycardia, and hypertension requiring hospital admission after CT-guided biopsy. This pain response may be considered and discussed with patients as a possible outcome of biopsy of a presumed osteoblastoma or osteoid osteoma.
Osteoblastoma, Osteoid osteoma, Biopsy, Complication, RF ablation, Flare phenomenon
According to the 2020 World Health Organization classification of bone tumors, osteoblastoma is classified as an intermediate (locally aggressive) tumor [1,2]. It is an osteogenic tumor that has traditionally been treated by surgical curettage or marginal excision, but recurrence rates historically are between 15-25%, with continued shift towards primary percutaneous radiofrequency ablation (RFA) [3], which is usually considered among first-line therapies at our institution. The lesion in this case produced chronic right-sided sciatica and unilateral sacroiliac ankylosis, which may be novel associations with osteoblastoma. When the lesion was biopsied with CT guidance, the patient’s pain and physiologic response was striking, requiring hospital admission. Going forward, this pain response may be considered and discussed as a possible outcome when consenting a patient for biopsy of a presumed osteoblastoma.
A 26-year-old healthy man presented to an outpatient pain clinic with two years of gradual, non-traumatic progression of right lower back pain. The pain was characterized as 4/10 at baseline, with flares reaching a 9/10 occasionally waking him from sleep, and was somewhat relieved with NSAIDs. Initial outside CT scan (Figure 1) showed ankylosis of the right sacroiliac joint with sclerosis of the posterior right ilium, clinically felt reflective of chronic sacroiliitis. The patient also reported symptoms of sciatica with pain radiating from the back of his leg to his foot. He underwent right sacroiliac joint and piriformis trigger point injections that provided no pain relief, and he was referred to an orthopedic surgeon for consideration of a piriformis release; however, no procedure was performed.
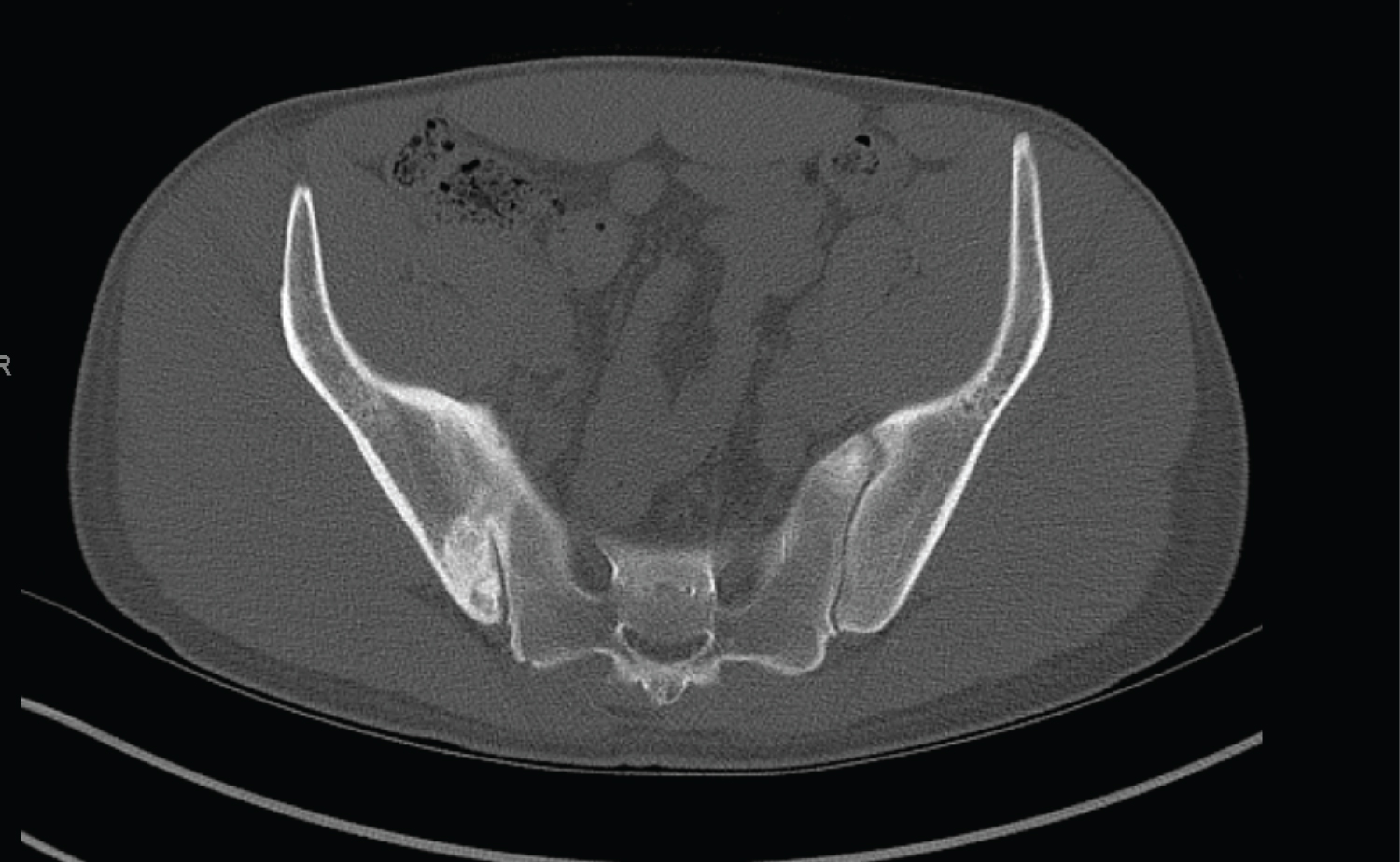 Figure 1: 26-year-old man with right pelvic pain and right-sided sciatica. Axial CT image, interpreted as chronic sacroiliitis by outside radiologist, pain management, and orthopedic surgery.
View Figure 1
Figure 1: 26-year-old man with right pelvic pain and right-sided sciatica. Axial CT image, interpreted as chronic sacroiliitis by outside radiologist, pain management, and orthopedic surgery.
View Figure 1
The patient worked with physical therapy for the next 14 months, and was referred to an orthopedic spine center for concern of developing S1 radiculopathy. Further imaging evaluation included a Tc-99 m MDP bone scan and a pelvic MRI without contrast. The bone scan showed localized uptake in the posterior right ilium (Figure 2) and the MRI showed a lesion in the posterior right ilium with adjacent sclerosis and edema-like marrow pattern involving the right ilium and crossing the sacroiliac joint (Figure 3). The patient was then referred to the orthopedic oncology clinic. At this time, he reported that ibuprofen was the only medication that helped his symptoms, and he was taking over the daily recommended dose.
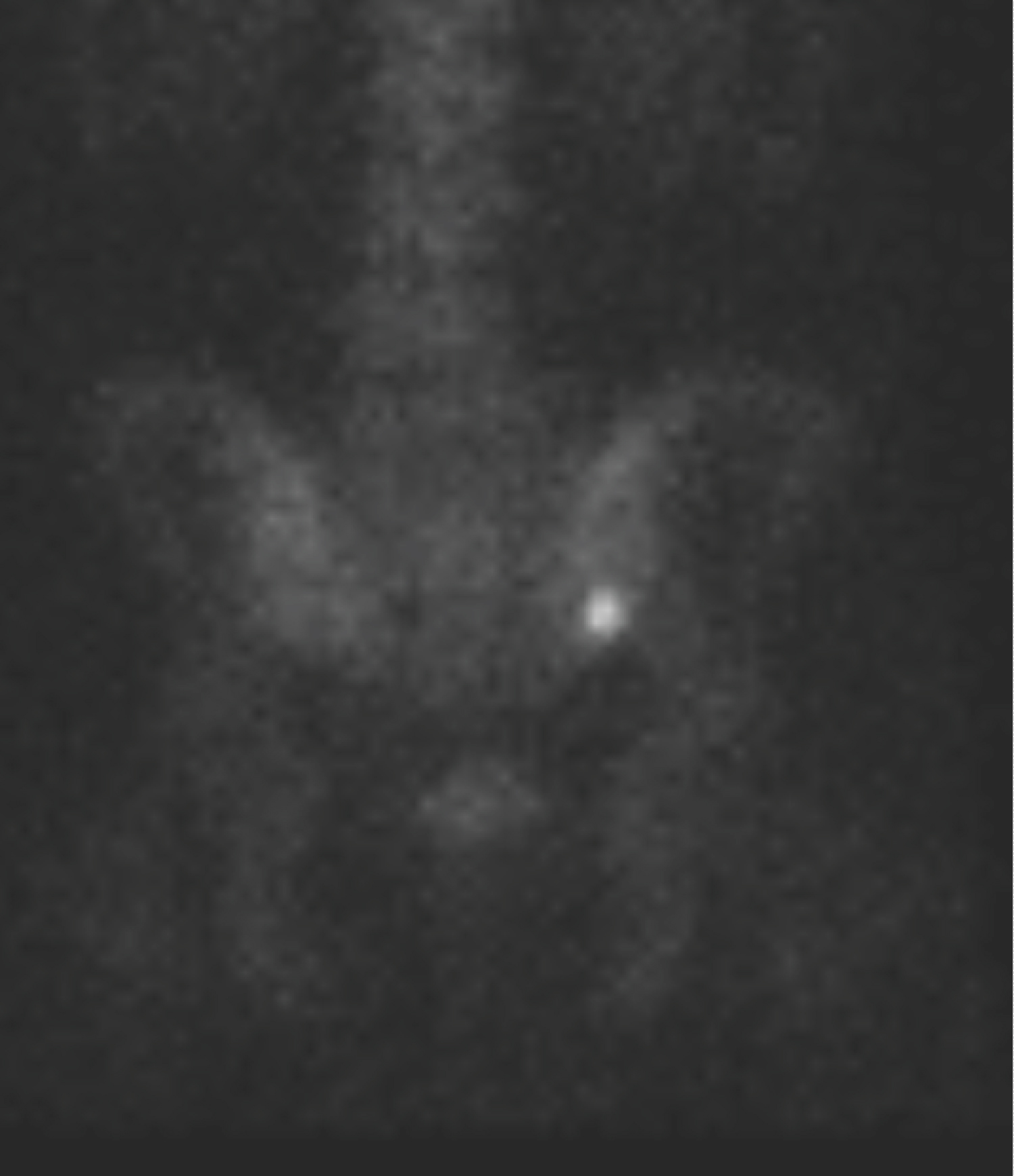 Figure 2: 28-year-old man with right pelvic pain and right-sided sciatica. Posterior view of Tcc99m-MDP bone scintigraphy 2 years after presentation showing uptake in posterior right ilium.
View Figure 2
Figure 2: 28-year-old man with right pelvic pain and right-sided sciatica. Posterior view of Tcc99m-MDP bone scintigraphy 2 years after presentation showing uptake in posterior right ilium.
View Figure 2
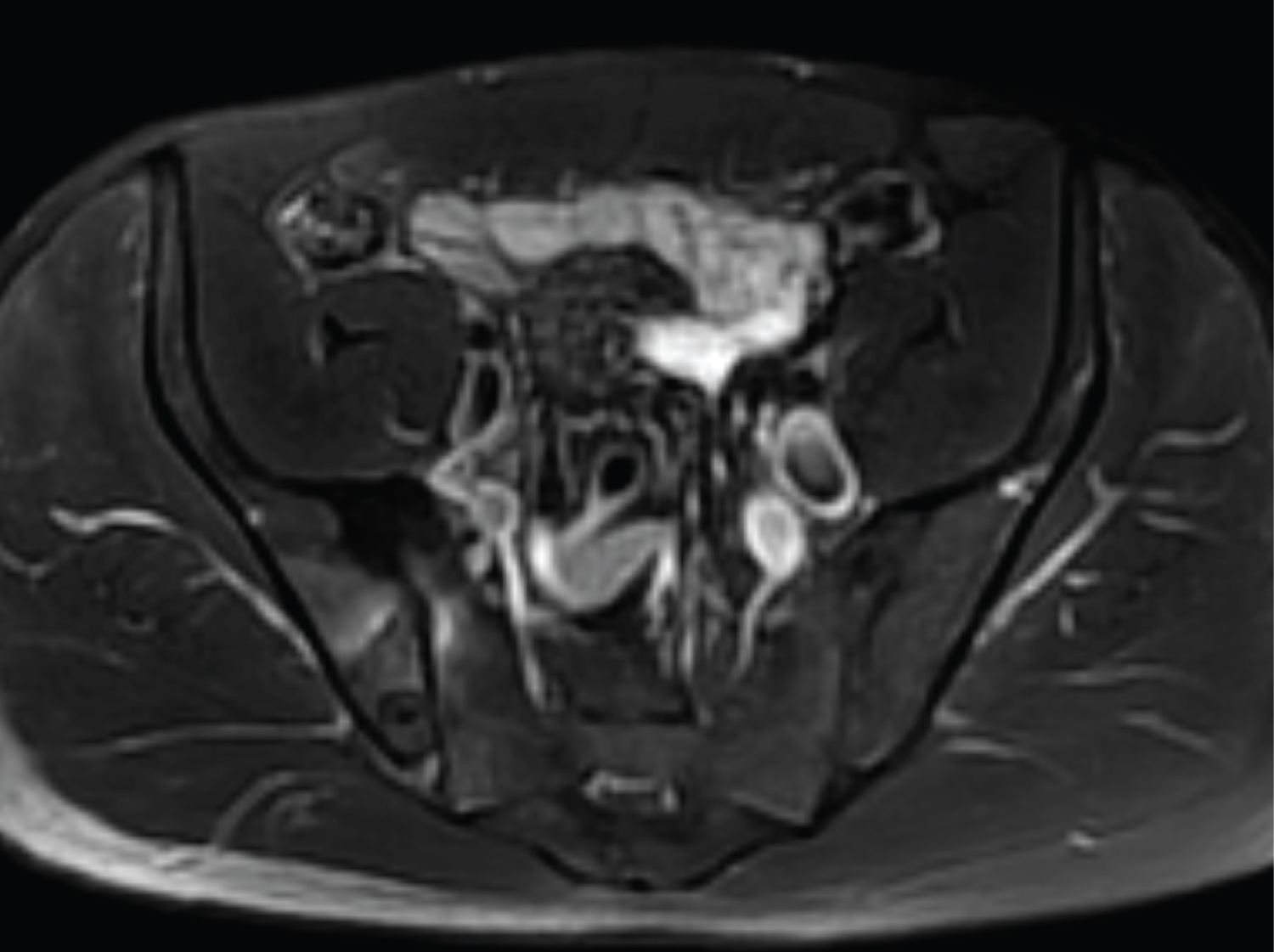 Figure 3: 28-year-old man with right pelvic pain and right-sided sciatica. Axial T2 fat-suppressed image showing lesion in posterior right ilium with adjacent low signal-intensity sclerosis and edema-like marrow pattern crossing the sacroiliac joint, with low signal intensity bone crossing the joint anteriorly.
View Figure 3
Figure 3: 28-year-old man with right pelvic pain and right-sided sciatica. Axial T2 fat-suppressed image showing lesion in posterior right ilium with adjacent low signal-intensity sclerosis and edema-like marrow pattern crossing the sacroiliac joint, with low signal intensity bone crossing the joint anteriorly.
View Figure 3
Given the two-year interval from initial CT, a repeat CT was performed which showed a defined, partially mineralized lesion in the posterior right ilium with adjacent sclerosis (Figure 4). The presumed diagnosis was osteoblastoma and treatment options were discussed with the patient including extended curettage and grafting versus CT-guided RFA. At our institution, lesions are commonly biopsied and ablated in the same setting. The patient was interested in RFA, but given the length of his presentation, he opted for a CT-guided biopsy prior to deciding on definitive treatment.
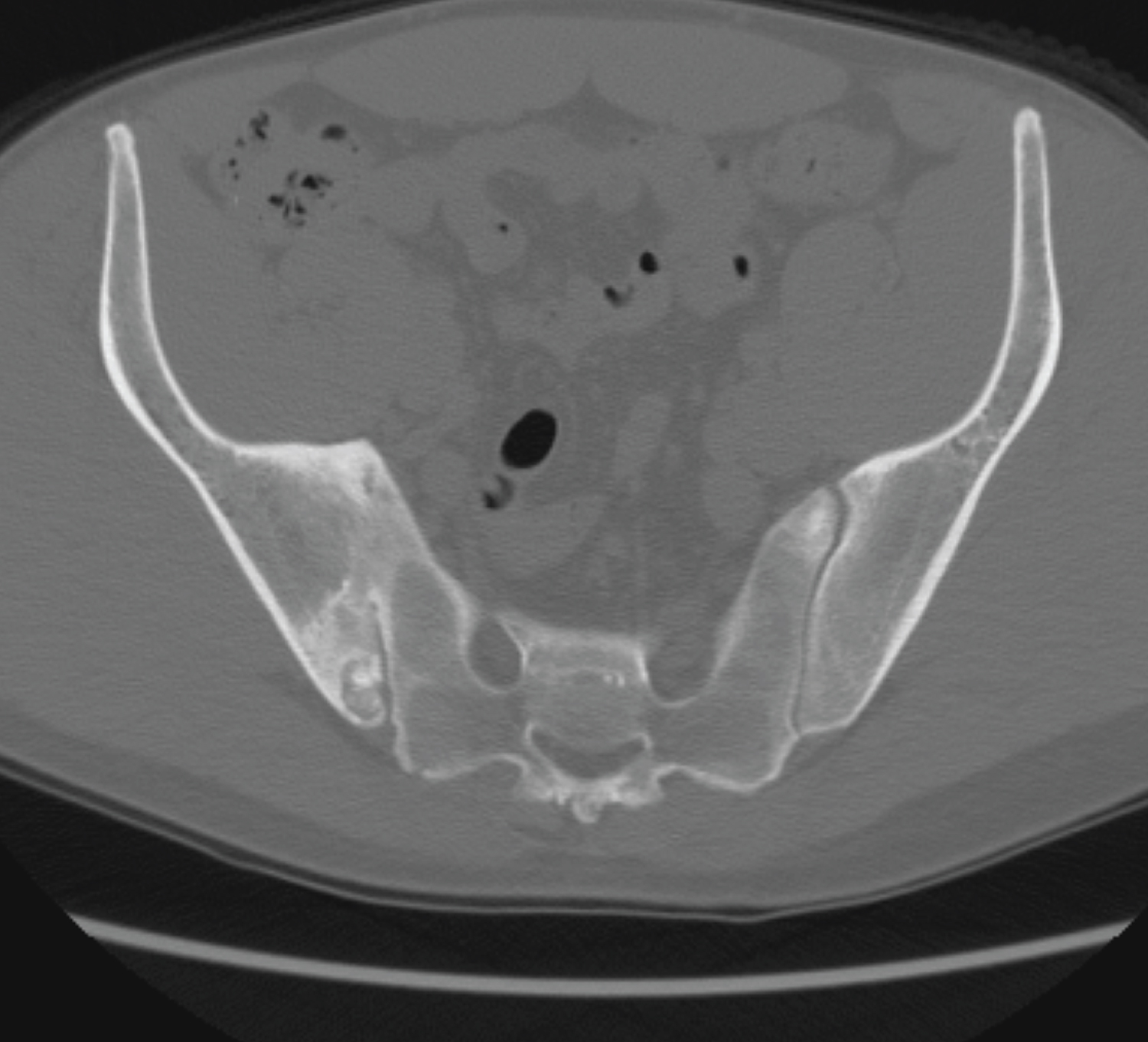 Figure 4: 28-year-old man with right pelvic pain and right-sided sciatica. Axial CT image 2-years after presentation showing enlargement of the posterior right ilium bone-forming lesion, with adjacent sclerosis and ankylosis across the sacroiliac joint.
View Figure 4
Figure 4: 28-year-old man with right pelvic pain and right-sided sciatica. Axial CT image 2-years after presentation showing enlargement of the posterior right ilium bone-forming lesion, with adjacent sclerosis and ankylosis across the sacroiliac joint.
View Figure 4
At our institution, routine, outpatient CT-guided bone biopsies are performed using 1% lidocaine local and periosteal anesthesia. Patients are pre-medicated with alprazolam and hydromorphone. A powered bone access system (Arrow © On Control © , Teleflex, Wayne, PA, USA) is used to obtain 12 or 13 gauge cores. After the biopsy, the patient is observed in nursing observation for 1 hour prior to discharge home. If an RFA is to be performed immediately following the biopsy, then anesthesia is consulted for the procedure. The RFA is performed as has been previously described, heating the probe to 60-90 degrees Celsius for a period of approximately 6 minutes [4]. Intra-procedural injection of ketorolac is helpful to decrease pain and inflammation on recovery [5].
During a biopsy/ablation of an osteoid osteoma, there is a predictable increase in heart rate and respiratory rate when the needle enters the tumor [6]. In this patient, once the biopsy needle entered the lesion (Figure 5), the patient immediately complained of severe pain. Two cores were obtained, which confirmed the diagnosis of osteoblastoma. When the patient returned to observation, his pain level continued to increase. He was writhing in pain and had difficulty finding any comfortable position, with severe worsening of his right sided sciatica. Vital signs demonstrated that he was tachycardicto 101 and hypertensive to 152/98. Multiple medications were given to attempt to control his pain, including ketorolac, acetaminophen, additional hydromorphone, gabapentin, and dexamethasone. Given this uncharacteristic severe pain and his vital sign changes, orthopedic oncology was consulted, and the decision was made jointly to admit to observation status. He received more medications overnight and a trigger point therapeutic injection from anesthesia which provided minimal relief. Ultimately, in the morning he decided to go home. At this time, he was still complaining of pain, only partially improved, with a gradual decrease in pain over the next few days. Due to the severity of his pain associated with the percutaneous procedure, he elected for a surgical excision under general anesthesia rather than RFA for definitive management.
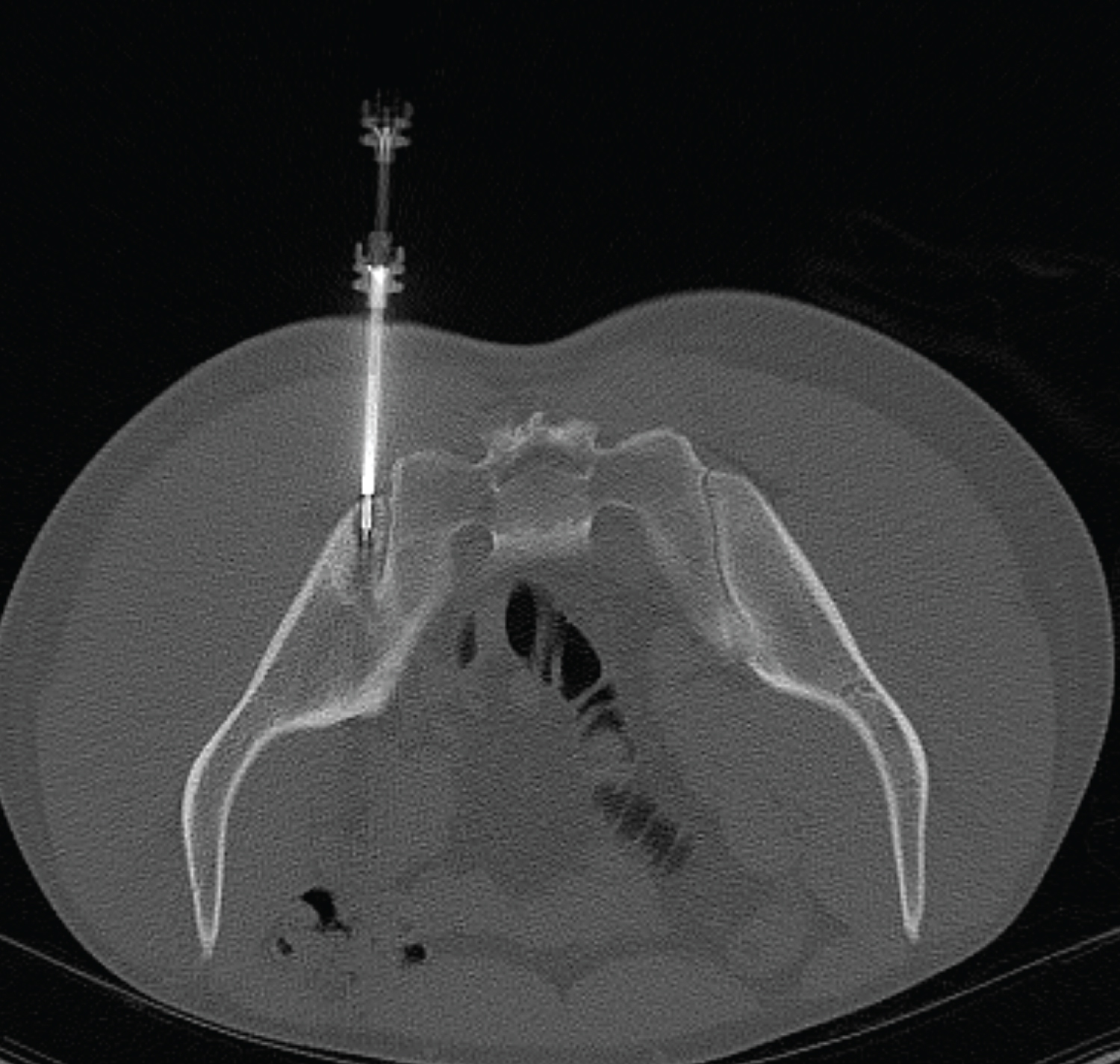 Figure 5: 28-year-old man with right pelvic pain and right-sided sciatica. Intra-procedural CT-guided biopsy showing placement of the biopsy needle into the mass of concern.
View Figure 5
Figure 5: 28-year-old man with right pelvic pain and right-sided sciatica. Intra-procedural CT-guided biopsy showing placement of the biopsy needle into the mass of concern.
View Figure 5
Three weeks later, he was taken to the operating room for surgical excision in the form of curettage and bone grafting. General anesthesia was induced, and he was positioned prone on a radiolucent operating table. Fluoroscopic images were used to localize the lesion on the posterior ilium. An incision was made directly overlying the lesion in line with the gluteus maximus fibers. Dissection was carried through the gluteus maximus and the posterior ilium was exposed. An 18 gauge needle was used to localize the lesion fluoroscopically. A burr was then used to create a cortical window and remove the contents of the lesion. Next, three-dimensional fluoroscopic images were obtained to verify complete removal of the contents of the lesion. Subsequently, argon beam electrocautery was used for extended curettage. The defect was then filled with 4 cc of demineralized bone matrix, and the wound was closed in layered fashion.
At his first, post-operative appointment two weeks following the procedure, the patient reported complete resolution of his pain as well as sciatic nerve symptoms. His incision was healing well, and he had returned to normal activities. Three months following the procedure, he continued to report complete resolution of his symptoms. X-rays demonstrated expected post-operative changes with interval bony remodeling of the bone graft, without evidence of local recurrence.
Crim, et al. described “the flare phenomenon,” an inflammatory response to osteoblastoma associated with marrow edema, sclerosis and periostitis in adjacent bones in the spine [7]. Subsequently, a similar case was described in the lumbar spine associated with contiguous ankylosis of the facet joints [8]. Osteoblastoma has been previously described crossing the joint itself, even though cartilage is a relative barrier to the spread of tumor [9]. However, this case differs as the adjacent periostitis fused across the joint, rather than the tumor itself, mimicking sacroiliitis. More interestingly though, the chronic sciatic symptoms, and subsequent severe pain and transient tachycardia and hypertension at time of biopsy may be related to release of local inflammatory mediators.
Cyclo-oxygenase (COX) has two primary forms, COX-1 and COX-2, and is a key enzyme in prostaglandin synthesis through the arachidonic acid metabolic pathway. COX-2 is characteristically induced in inflammatory tissue [10], and is expressed in certain tumors, including osteoid osteoma and osteoblastoma [11]. COX-2 expression is hypothesized to be the cause of the local flare phenomenon and of systemic inflammatory responses in certain patients with osteoblastoma. Specifically, Cox-2 synthesizes prostaglandin that mediates not only inflammation, but also acute pain and primary hyperalgesia [12]. In this case, we felt that acute activation of this pathway when the biopsy needle punctured the tumor likely produced the patient’s symptoms at biopsy. Given the severity of this particular response, we will discuss this possible outcome with future patients with suspected osteoblastoma (or osteoid osteoma) at time of biopsy consent.
Not applicable.
The authors declare that they have no conflict of interest.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
TS, MR, and CA all participated in care of the patient and preparation of the manuscript.