Clavicle is an S-shaped subcutaneous bone which increases the band ring power of the shoulder. Clavicle fractures account for approximately 4% of all fractures. Fractures occur most commonly in the middle third of the bone (76-82%) and less often in the distal (12-21%) and medial (3-6%) thirds [1,2]. There appears to be a fairly uniform consensus regarding conservative management for medial third fractures and operative for displaced distal third fractures, however that for mid third clavicular fractures is still emerging. Traditionally most of these fractures have been treated with benign neglect, slings, or figure-of-eight harnesses. Historically we were taught, "All clavicle fractures do well with non-operative treatment".
We report a case of segmental clavicle fracture in an adolescent caused by direct trauma while playing cricket. An 18-year-old boy presented to the emergency department with pain over the right clavicle. There was no open wound. Physical examination revealed tenderness over the clavicle with deformity and restricted shoulder joint movements secondary to shoulder pain. The physical examination and radiography findings showing a displaced fracture of the clavicle, shortening and skin tenting and early rehabilitation required for the patient to resume his playing cricket were indications for surgery.
There was no evidence of neurovascular deficit or other significant injuries.
Radiographs showed a segmental fracture clavicle involving mid shaft.
Anteroposterior radiographs can best assess a clavicle fracture, especially in the proximal portion of the clavicle (Figure 1). Computed tomography (CT) imaging can be utilized for evaluation of intra-articular involvement of the medial and lateral ends of the bone and preoperative and detailed evaluation of the injury (Figure 2).
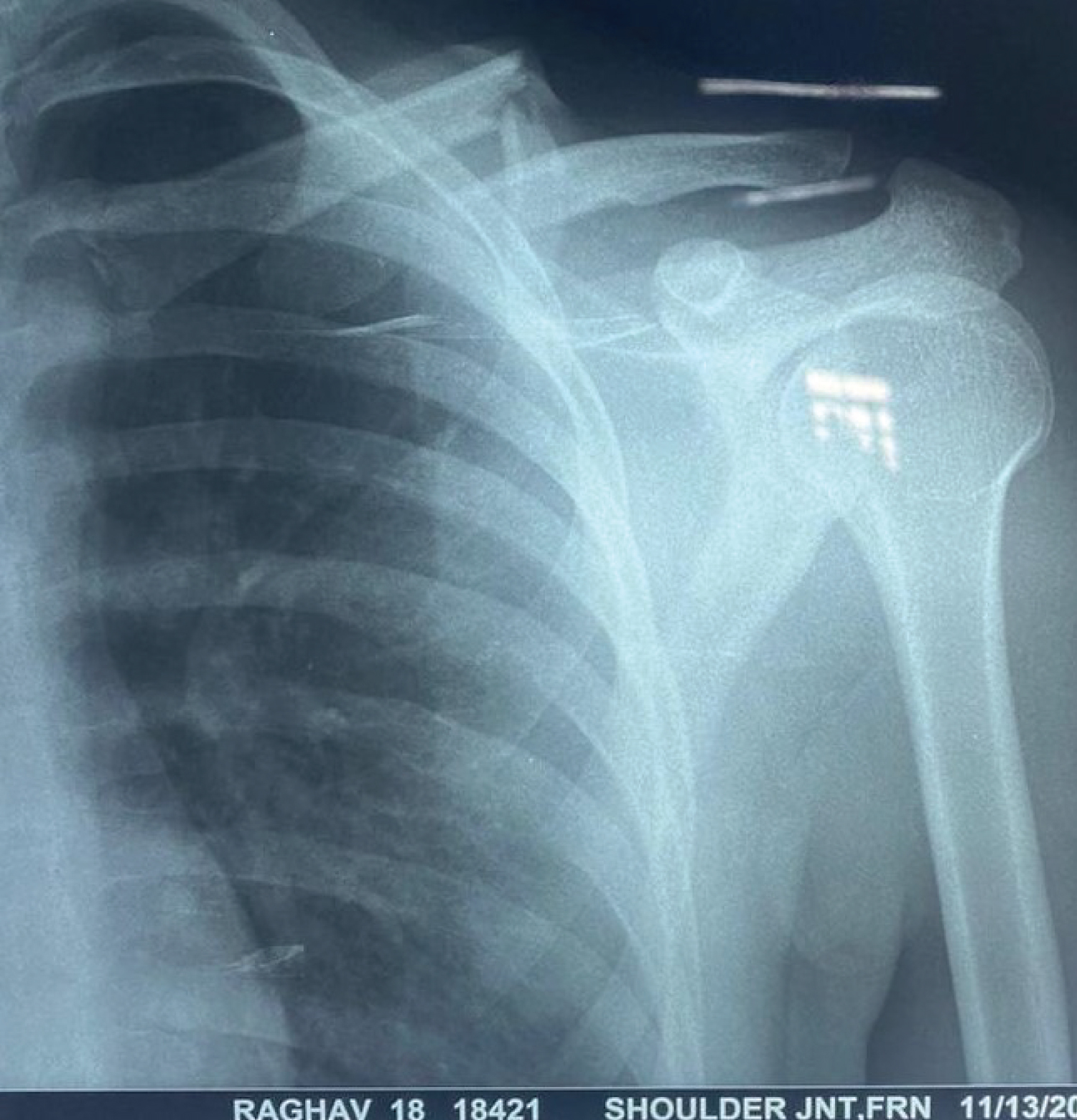 Figure 1: Anteroposterior radiograph of the clavicle showing segmental fracture of the clavicle on the left side.
View Figure 1
Figure 1: Anteroposterior radiograph of the clavicle showing segmental fracture of the clavicle on the left side.
View Figure 1
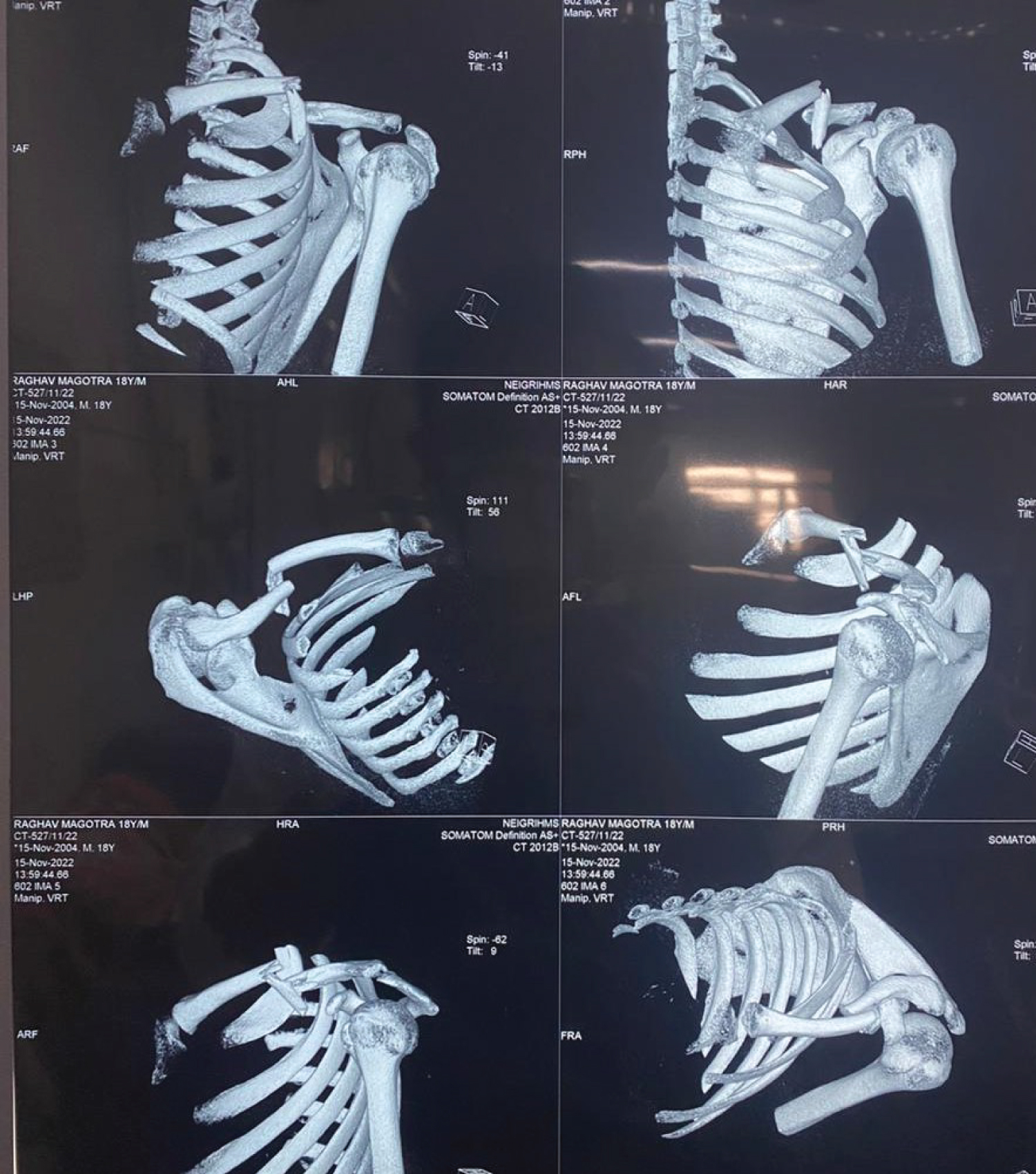 Figure 2: CT scan showing segmental fracture on the left side and rules out any other injury.
View Figure 2
Figure 2: CT scan showing segmental fracture on the left side and rules out any other injury.
View Figure 2
The patient was operated in supine position with sandbag in the interscapular region, with the arm draped free for easy manipulation. A curvilinear anterosuperior subcutaneous approach along the langers lines was employed. The skin and soft tissue with platysma was incised exposing the segmental fracture including middle 1/3rd of the clavicle. The fracture was reduced ensuring a perfect anatomical reduction with use of interfragmentary lag screw fixation of the segmental fracture with oblique ends using one screw one each to proximal and distal fragment to attain normal length of the clavicle. Fracture was stabilized with the fixation of 3.5 mm clavicular locking plate on the superior surface (Figure 3). Post operative radiographs showed good reduction and alignment with stable fixation of the fracture (Figure 4 and Figure 5). Postoperatively, shoulder immobiliser was used to immobilize the shoulder. Elbow and wrist movements were started in immediate post-op period. The initial phase of the rehabilitation program involved passive mobilization of the shoulder, which was started in the third week. The second stage was usually started after the fifth postoperative week, with the aim of restoration of the entire range of motion of the shoulder.
 Figure 3: Peroperative picture showing well fixed clavicle fracture with lag screws anteriorly and superiorly placed 3.5 mm clavicle locking plate.
View Figure 3
Figure 3: Peroperative picture showing well fixed clavicle fracture with lag screws anteriorly and superiorly placed 3.5 mm clavicle locking plate.
View Figure 3
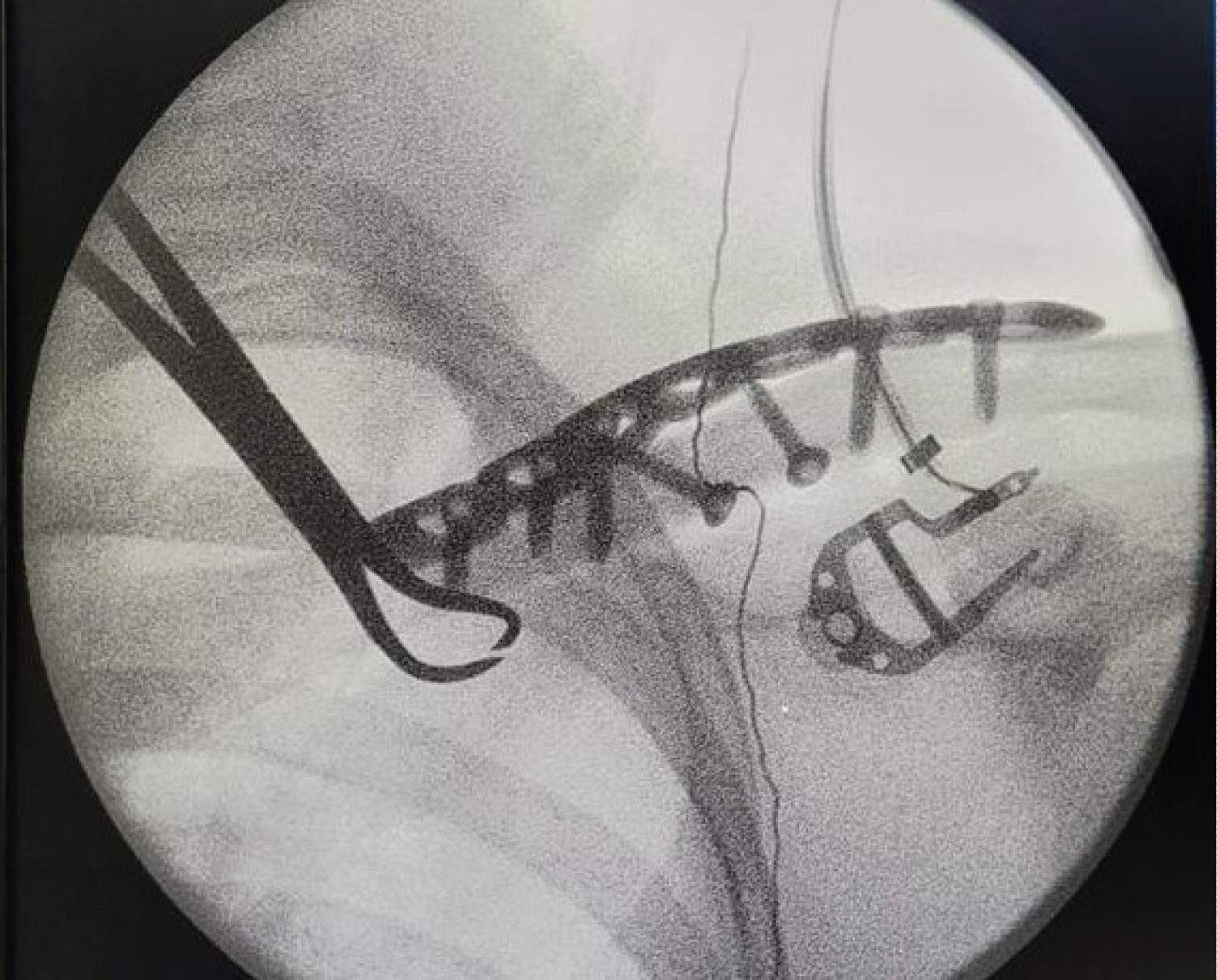 Figure 4: Image taken preoperatively confirming well aligned fracture stabilized with clavicular locking plate and lag screws.
View Figure 4
Figure 4: Image taken preoperatively confirming well aligned fracture stabilized with clavicular locking plate and lag screws.
View Figure 4
 Figure 5: Image taken preoperatively confirming well aligned fracture stabilized with clavicular locking plate and lag screws.
View Figure 5
Figure 5: Image taken preoperatively confirming well aligned fracture stabilized with clavicular locking plate and lag screws.
View Figure 5
Mid-shaft clavicular fractures represent an overwhelming majority of these injuries (80%). Open reduction and internal fixation is associated with shorter time to union and better functional recovery.
It is now well documented that displaced mid-third clavicular fractures in adults do poorly when treated non-operatively [3], have higher rate of nonunion and, even when they unite, often result in an unsightly cosmetic bump in the centre of clavicle, shoulder ptosis, shoulder discomfort, and patient dissatisfaction [4,5]. When it involves a young active soldier any compromise in shoulder function due to malunion/nonunion of clavicular fracture severely hampers his employability.
Segmental long bone fractures are considered unstable injuries with the risk of nonunion and nonoperative approach being considered unacceptable [6]. The clavicle forms an important part of the shoulder girdle and is vital for the normal functioning of the upper limb. Non-union of the clavicle fracture would result in considerable functional deficit. With meagre literature regarding segmental clavicle injuries, no consensus exists about the management of these fractures with some case reports advocating a non-operative [7,8] while others an operative approach [6,9].
The optimal treatment needs to be individualised based on the patient and fracture pattern. The most predictable method to maintain anatomic reduction of displaced mid shaft clavicular fractures, including length and rotation is in my opinion a plate and screw fixation. Athletic involvement like playing cricket can increases the risk for clavicle fracture. The use of protective equipment like clavicle and shoulder pads when participating in contact sports may decrease the risk of clavicle fracture and other injuries in the region. The treatment should be based on the individual fracture pattern and patient characteristics.
Informed consent was taken.
The author declares that there is no conflict of interest.