Colovesical fistulas (CVFs) represent a rare but clinically significant complication, often associated with diverse etiologies including malignancies. Herein, we present a case of a 71-year-old male with a history of Benign Prostatic Hyperplasia (BPH) who presented with hematuria and dysuria. Initial investigations revealed a bladder mass, which upon further evaluation unveiled a colovesical fistula secondary to colorectal adenocarcinoma. The patient underwent laparoscopic sigmoidal resection, colostomy creation, and partial cystectomy. Histopathological staging indicated pT4a pN0 for sigmoid colon adenocarcinoma, with no lymph node involvement. This case underscores the diagnostic challenges posed by overlapping benign and malignant conditions and highlights the importance of comprehensive evaluation and multidisciplinary management. Accurate diagnosis and timely intervention are paramount for optimal patient outcomes in cases of CVF, especially when associated with colorectal malignancies.
Colovesical fistulas exhibit diverse etiologies encompassing congenital, acquired, iatrogenic and direct malignant invasion origins [1]. Manifestations such as pneumaturia, fecaluria, severe urinary tract infection and urinary discharge via the rectum frequently experience relief through the implementation of fecal and urinary diversion [2]. We present a case of colovesical fistula secondary to colorectal adenocarcinoma.
The patient, a 71-year-old male with a history of Benign Prostatic Hyperplasia (BPH), presented with hematuria persisting for two months, which intensified to gross hematuria over the last three days. He also reported dysuria with clots, mostly appearing at the end of urination. Despite being diagnosed with BPH six years ago, the patient irregularly used medication due to irritative and storage symptoms. He denied experiencing vomiting, nausea, fever, night sweats, weight loss, changes in appetite, or alterations in bowel habits. Upon clinical examination, a CT scan revealed diffuse irregular thickening of the urinary bladder wall (up to 1.8 cm) with a partially exophytic mass at the bladder dome (Figure 1). This mass exhibited mucosal breakthrough and was inseparable from the adjacent sigmoid loop, accompanied by mild peri nephric fat stranding. No ureteric filling defects or hydroureteronephrosis were observed.
 Figure 1: Coronal and sagital sections of CT pelvis showing Urinary bladder dome partially exophytic mass inseparable from the adjacent sigmoid.
View Figure 1
Figure 1: Coronal and sagital sections of CT pelvis showing Urinary bladder dome partially exophytic mass inseparable from the adjacent sigmoid.
View Figure 1
As regard the findings in the CT a transurethral resection of the bladder tumor (TURBT) was done and three way foleys catheter was applied, the patient tolerated the procedure and tissue biopsy was obtained and sent for histopathological examination. On the second day post-operative and with patient stabilization and observation of clear urine from the catheter, the patient was discharged and instructed for a follow up after three weeks for histopathology discussion and catheter removal. Two days post-operative the patient presented to the ER with foul smelling brown urine. A post-procedure CT scan with enema contrast showed a colovesical fistula between the sigmoid colon and the urinary bladder, characterized by wall thickening and peri vesical fat stranding (Figure 2). Subsequent MRI revealed a defect in the superior wall of the urinary bladder communicating with the sigmoid colon, indicative of a fistulous tract. At that time histopathological examination confirmed moderately differentiated invasive adenocarcinoma in the sigmoid colon mass and urinary bladder mass, consistent with colorectal origin (Figure 3). Colonscopy was done with a rectosigmoidal biopsy further confirmed invasive adenocarcinoma.
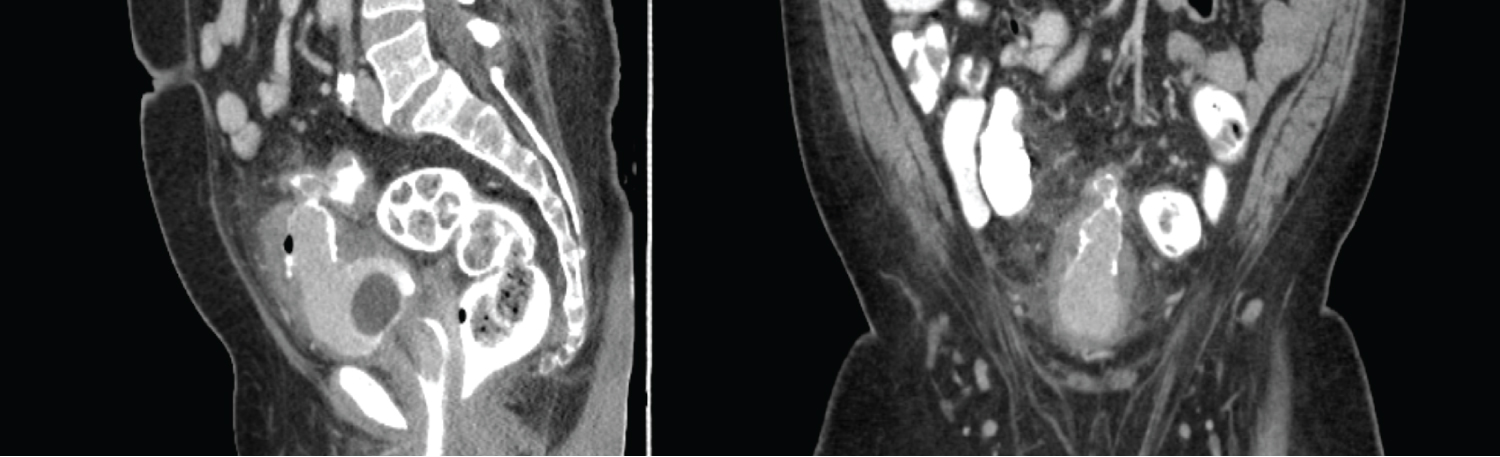 Figure 2: Coronal and sagital sections of post contrast CT Pelvis showing a post TURT status short, where there is a segment of sigmoid circumferential wall thickening seen adherent to the urinary bladder dome with contrast seen tracking between sigmoid and urinary bladder.
View Figure 2
Figure 2: Coronal and sagital sections of post contrast CT Pelvis showing a post TURT status short, where there is a segment of sigmoid circumferential wall thickening seen adherent to the urinary bladder dome with contrast seen tracking between sigmoid and urinary bladder.
View Figure 2
 Figure 3: Sagital and coronal sections of the MRI pelvis showing a post TURT status, where the colovesical fistulous tract associated with urinary bladder dome and sigmoid colon mural thickening and hyperenhancement.
View Figure 3
Figure 3: Sagital and coronal sections of the MRI pelvis showing a post TURT status, where the colovesical fistulous tract associated with urinary bladder dome and sigmoid colon mural thickening and hyperenhancement.
View Figure 3
The patient underwent laparoscopic sigmoidal resection, colostomy creation, and open partial cystectomy as part of the treatment plan. Pathological staging indicated pT4a pN0 for sigmoid colon adenocarcinoma invading to bladder, with no lymph node involvement observed in either the bladder or sigmoid specimens.
Colovesical fistula (CVF), an abnormal epithelized connection between the rectum and the urinary bladder, presents a significant challenge for clinicians due to its rarity, diverse etiologies, complex presentations, and lack of a standardized treatment approach [1]. While the exact prevalence remains elusive, several factors can contribute to CVF formation. Patients diagnosed with diverticulitis or inflammatory bowel disease (IBD) demonstrate an elevated susceptibility, highlighting the potential involvement of chronic inflammation in the pathogenesis of tissue impairment and structural vulnerability between the rectum and bladder [2]. Colorectal malignancies, especially those involving a direct local spreading into the bladder wall, forming an CVF in up to 20% of cases [2], same as we conclude in our presented case. Iatrogenic injury during pelvic surgeries, such as laparoscopic or robotic prostatectomy, is another significant cause, with an incidence of up to 1% following radical prostatectomy [3]. Moreover, factors such as trauma, radiotherapy, and congenital anorectal malformations have been identified as a less common causative contributor to the development of colovesical fistula (CVF) [4].
Accurate differentiation between CVF and recto urethral fistula is crucial for guiding surgical management. Unlike CVF, where the abnormal connection originates in the bladder neck at the level of the vesicourethral anastomosis, a recto urethral fistula involves a fistulous tract located within the true urethra. This distinction is critical because the surgical approaches for each condition may differ [2].
Furthermore, CVFs can be classified based on their complexity, which influences treatment decisions. Simple fistulas are characterized by a single tract, less than 2 cm in size, with no prior repair attempts or exposure to energy treatments. In contrast, complex fistulas involve multiple tracts, are larger than 2 cm, have a history of failed repair attempts, have been exposed to energy treatments like radiation therapy, or coexist with bladder neck strictures. These additional features often necessitate more complex surgical interventions [5].
Diagnosing CVF requires a comprehensive evaluation. A detailed history exploring underlying diseases, previous surgeries, and potential risk factors like radiotherapy exposure forms the initial step [2]. Clinically, CVF can manifest with a range of symptoms, the most common presentation is recurrent urinary tract infections (UTIs), affecting up to 88% of patients [2]. Depending on the severity of the fistula and the direction of flow, other symptoms like fecaluria, pneumaturia, and urinary leakage per rectum may also occur. Local pelvic examination can reveal localized signs such as erythema around the fistula opening or a palpable rectal defect on digital examination.
While clinical features are suggestive, definitive diagnosis relies on imaging studies. Abdominopelvic CT with oral or rectal contrast, without intravenous (IV) contrast, emerges as the primary diagnostic tool, exhibiting high sensitivity in detecting CVFs [6]. Findings include intravesical air, colonic diverticula, and thickening of the colon-bladder wall [7]. Also the efficacy of MRI has been established in the diagnosis of complex fistulas with high sensitivities and specificities [7]. Colonscopy complements CT imaging by elucidating underlying pathologies, although its lower sensitivity for CVF detection. Also cystoscopy allows visualization of the bladder and potential identification of the fistula opening within [8]. In cases where malignancy is suspected based on the patient's history or imaging findings as we identified in the current case, a biopsy may be necessary to confirm the diagnosis [8].
Treatment options for CVF can be broadly categorized into conservative and surgical approaches. Conservative management, often the initial approach, aims to promote healing by performing a urinary and fecal diversion away from the fistula. This typically involves using a urinary catheter, either transurethral or suprapubic, with performing a defunctioning colostomy. The duration of conservative management is individualized and lacks standardization, often decided by the treating physician based on the patient's specific condition and response to treatment [9].
Surgical intervention may be necessary in specific cases, particularly when conservative management fails to achieve complete healing or when the patient experiences significant symptoms. While there is no single standardized surgical approach for CVF repair, a transabdominal approach offers several advantages. This approach allows the surgeon to access both the fistula and the colon for repair, potentially placing interposed tissue, like healthy muscle or fat, between the repaired areas to prevent recurrence [10]. Additionally, it allows for the creation of a colostomy or urinary diversion during the same surgery, if deemed necessary [10]. However, other surgical approaches like transperineal, trans-sphincteric transrectal (York-Mason), transanal, and trans-sacral techniques are also available [5]. These approaches may be technically more challenging due to limited space and carry a higher risk of complications compared to the transabdominal approach. Minimally invasive techniques, such as laparoscopy and robotic surgery, are gaining traction in CVF repair due to their potential benefits [1].
The presented case underscores the diagnostic challenges posed by overlapping benign and malignant etiologies of colovesical fistula. Initial symptoms suggestive of bladder pathology in a patient with a history of Benign Prostatic Hyperplasia (BPH) led to the discovery of a bladder mass, subsequently revealing a colovesical fistula and underlying colorectal adenocarcinoma. Timely surgical intervention, including laparoscopic sigmoidal resection and partial cystectomy, aimed at addressing both the fistula and malignancies. The absence of lymph node involvement offers a favorable prognosis, highlighting the importance of early detection and comprehensive treatment strategies. This case emphasizes the necessity for clinicians to maintain a broad differential diagnosis and pursue thorough investigations, especially in patients with uncommon presentations related to the urinary and/or the lower gastrointestinal tract.