Background: Left ventricular (LV) leads are important devices for stimulating the most delayed site in cardiac resynchronization therapy (CRT). Since April 2020, the Attain Stability Quad (ASQ) lead, which has a side helix for facilitating active fixation, has become available in Japan. We evaluated the benefits of ASQ leads compared with those of conventional passive fixation LV leads.
Methods: From April 2016 to July 2021, 70 CRT implant patients were enrolled in this single-center retrospective observational study. The patients were divided into two groups for comparison: the ASQ (n = 35) and non-ASQ groups (n = 35).
Results: There were no differences in preoperative age, gender, organic heart disease, comorbidities, LV ejection fraction, preoperative QRS complex, and the LV lead implantation threshold between the two groups. Six months after CRT implantation, the threshold was lower in the ASQ group than in the non-ASQ group (p = 0.03; 0.87 ± 0.21 V/0.4 ms vs. 1.06 ± 0.36 V/0.4 ms, respectively). In the ASQ group, LV pacing continued in all cases. The ASQ group could be implanted in the LV lateral wall and avoid placement in the apical segment. By placing the LV lead in the optimal location, the event occurrence rate for cardiovascular endpoints was lower in the ASQ group than in the non-ASQ group (log-rank p = 0.02 hazard ratio 3.83).
Conclusion: ASQ leads maintain a stable low threshold in the remote period after implantation. The ASQ lead performs LV pacing from a delayed optimal site in the LV and may contribute to preventing cardiovascular events.
Cardiac resynchronization therapy, Cardiac resynchronization therapy devices, Electrodes implanted, Heart failure, Heart ventricles, Ventricular dysfunction
Cardiac resynchronization therapy (CRT) has been established as a gold standard for heart failure treatment in patients with left bundle branch block (LBBB) in cases of chronic heart failure with systolic dysfunction [1]. It is critical for the left ventricular (LV) lead in CRT to pace the most delayed part of the LV [2]. However, the location of the LV lead is dependent on the venous anatomy of the coronary sinus (CS). There are cases in which LV pacing is performed from a site that is not the site of the most delayed part of the LV, making it impossible for the patient to receive the benefits of CRT [3]. Challenges involving the implantation of the LV lead occur when the pacing threshold of the LV lead becomes high, and the CRT itself is rendered useless due to the loss of LV capture. Dislodgement of the LV lead can also cause phrenic nerve stimulation. Phrenic nerve stimulation may be avoided by reprogramming the CRT, but it can result in ineffective LV pacing from unsuitable pacing sites. Additionally, if LV capture from all available pacing electrodes is lost or phrenic nerve stimulation cannot be avoided, reimplantation of the LV lead is required [4]. From the challenges described above, it is necessary to develop a more stable LV lead that can perform LV pacing in an ideal site.
In April 2020, the Attain Stability Quad (ASQ) 4798 lead (Medtronic), which is an active fixation LV lead with a side helix, became available in Japan. A feature of this novel ASQ lead is the placement of side helices between the 3rd and 4th pacing electrodes (Figure 1). This spiral side helix can be wrapped around the vessel wall of the target branch of the CS to secure the position of the lead. We investigated whether the LV pacing site in the new ASQ lead has no LV lead-related complications and can be safely paced from the most ideal position, along with exploring its clinical outcomes. A retrospective observational study was conducted with the aim of comparing ASQ leads with conventional passive fixation LV leads in patients with planned CRT implantation at our institution.
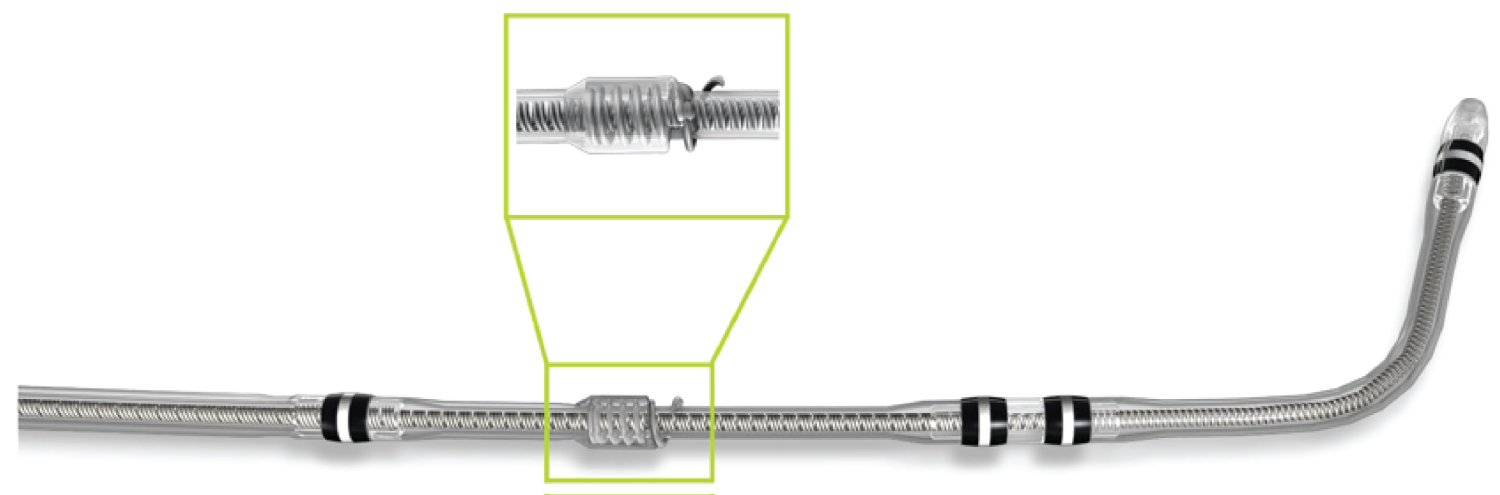 Figure 1: Attain Stability Quad (ASQ) Lead Overview. In April 2020, Medtronic made it possible to use the ASQ 4798 lead, an active passive left ventricular lead with a side helix, in Japan. A unique characteristic of ASQ leads is that the side helix is placed between the 3rd and 4th pacing electrodes.
View Figure 1
Figure 1: Attain Stability Quad (ASQ) Lead Overview. In April 2020, Medtronic made it possible to use the ASQ 4798 lead, an active passive left ventricular lead with a side helix, in Japan. A unique characteristic of ASQ leads is that the side helix is placed between the 3rd and 4th pacing electrodes.
View Figure 1
We performed an observational study using the arrhythmia registry data from St. Marianna University. All patients who underwent CRT insertion with a quadripolar LV lead from April 2016 to July 2021 were included in this study. Exclusion criteria included patients undergoing multipoint pacing therapy and stimulated conduction system pacing therapy, including His bundle pacing. Seventy patients were included in the final analysis. These patients were divided into two groups: 35 patients were treated with the active fixation lead, Medtronic Attain Stability Quad 4798 (ASQ), whereas 35 were treated with the conventional passive fixation quadripolar LV leads (non-ASQ). All CRT devices were implanted according to guidelines published in the JCS/JHRS 2018 revised edition [2]. Figure 2 shows the study design. The outcomes measured included LV lead placement positions, LV lead-related complications, the electrical performances of the LV leads, and heart failure hospitalization events. The study protocol was approved by the Institutional Committee on Human Resource at St. Marianna University School of Medicine (No. 4673), and informed consent was obtained from all patients (via the opt-out method) at our institution.
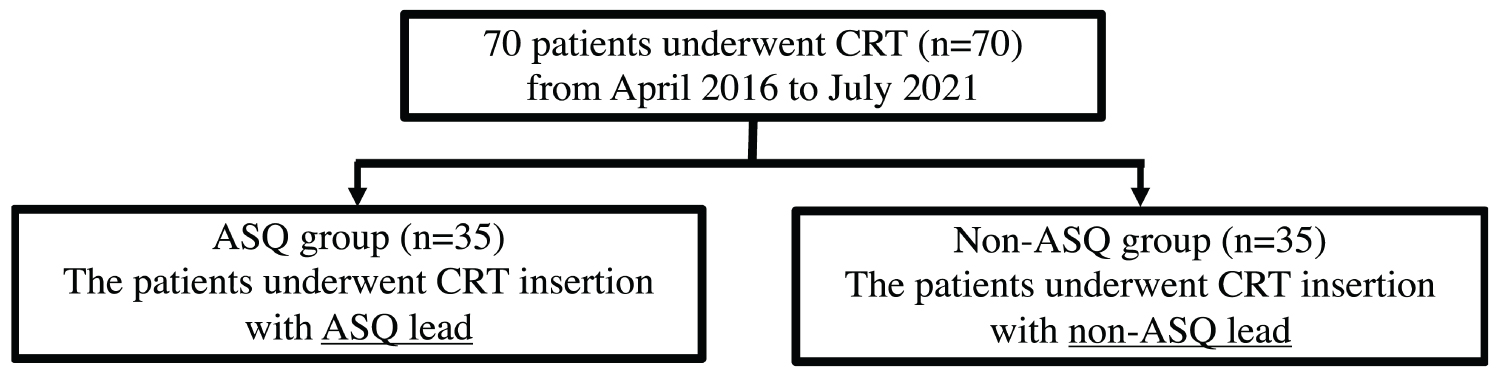 Figure 2: Study protocol. The study endpoints weighed left ventricular lead placement sites, left ventricular lead-related complications, electrical parameters of left ventricular lead, and heart failure readmission and cardiac death.
View Figure 2
Figure 2: Study protocol. The study endpoints weighed left ventricular lead placement sites, left ventricular lead-related complications, electrical parameters of left ventricular lead, and heart failure readmission and cardiac death.
View Figure 2
Statistical analyses were performed using IBM SPSS Statistics version 23 (IBM, Armonk, NY, USA). Categorical comparisons between groups were performed using a chi-square test and a Fisher's exact test for independence. Continuous variables were compared using a Wilcoxon signed-rank test and a Mann-Whitney U test. All continuous parameters were presented as the mean ± standard deviation (SD) values. Differences were considered statistically significant if the p-value was less than 0.05 (p < 0.05).
Table 1 shows the background of the 70 patients enrolled in this study. All patients received standard medication for heart failure. There were no significant differences in age, gender, or underlying heart disease between the ASQ and non-ASQ groups.
Table 1: Baseline characteristics of patients enrolled in this study. View Table 1
Table 2 shows the success rate of LV lead implantation and complications related to LV leads. The success rate of LV lead implantation was 100% in both groups (Table 2). Complications related to the LV lead include three patients in the non-ASQ group experiencing LV lead dislodgement during CRT implantation. The ASQ group did not experience any incidence of LV lead dislodgement during CRT implantation (Table 2). LV lead-related complications 6 months after CRT implantation are shown in Table 2. The ASQ group was able to continue LV pacing in all patients (Table 2). However, in the non-ASQ group, two patients abandoned LV pacing due to the high pacing threshold, and one case abandoned LV pacing due to inadvertent phrenic nerve stimulation (Table 2).
Table 2: Implant success rates and complications. View Table 2
Figure 3 shows the LV position of the LV pacing site of the indwelling lead. The ASQ group lead was positioned at the lateral segment of the LV, producing a statistically significant difference compared with the non-ASQ group. Moreover, compared with the non-ASQ lead, the ASQ group lead was positioned in the midventricular to basal section of the LV, clearly avoiding the apical segment. In the non-ASQ group, LV leads were placed in a site other than the LV lateral wall in two cases (Figure 3).
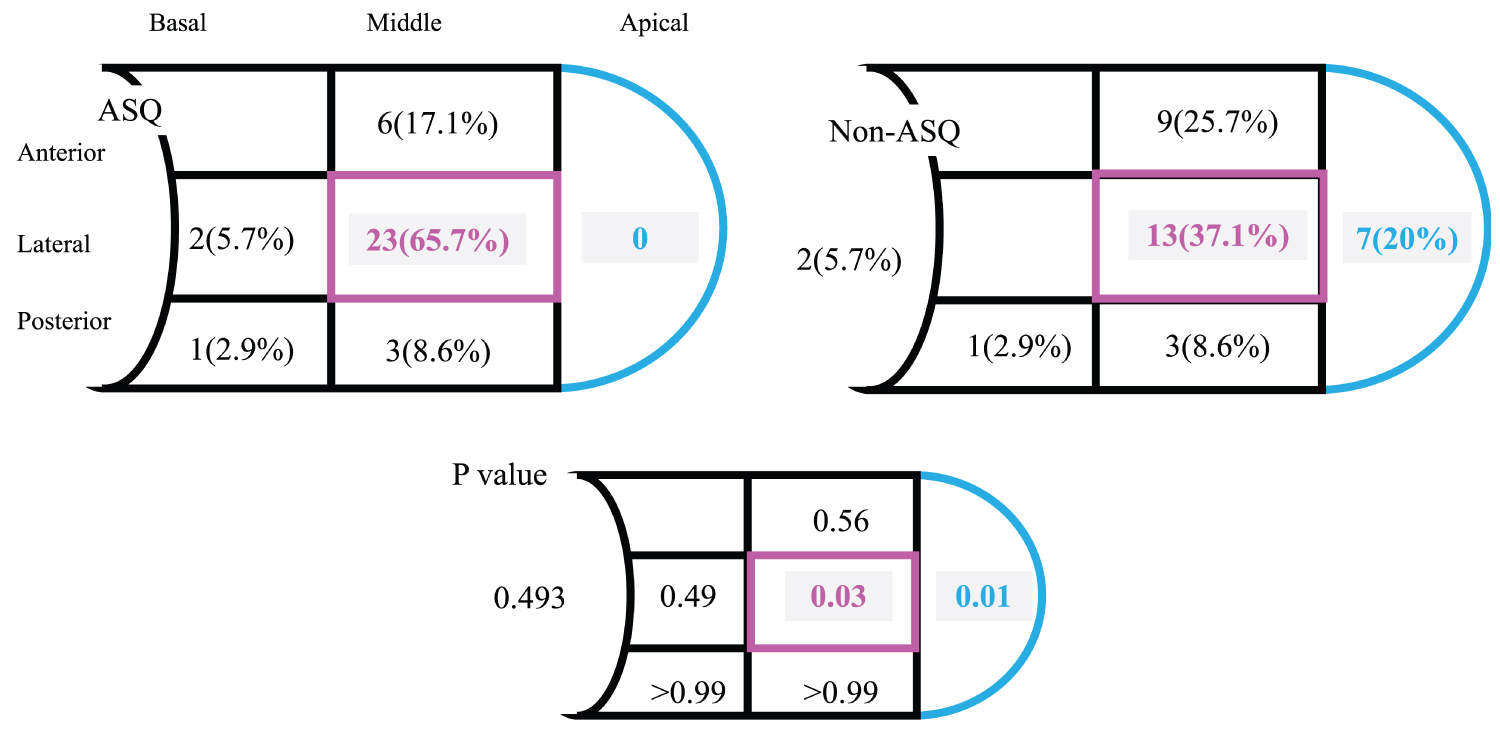 Figure 3: Comparison of left ventricular lead pacing sites. Compared with the non-Attain Stability Quad (ASQ) group, the ASQ group was able to pace from the lateral segment of the left ventricle; moreover, it was able to pace from the midventricular to the basal left ventricular segments and clearly avoided the apical segment.
View Figure 3
Figure 3: Comparison of left ventricular lead pacing sites. Compared with the non-Attain Stability Quad (ASQ) group, the ASQ group was able to pace from the lateral segment of the left ventricle; moreover, it was able to pace from the midventricular to the basal left ventricular segments and clearly avoided the apical segment.
View Figure 3
Table 3 shows the electrical parameters of the LV leads. There were no differences between groups regarding the LV lead pacing threshold (p = 0.12, ASQ group vs. non-ASQ group; 1.00 ± 0.42 V vs. 0.90 ± 0.34 V/0.4 ms) and the lead impedance (p = 0.39, ASQ group vs. non-ASQ) during CRT implantation. Of note, the pacing threshold for LV leads 6 months after CRT implantation was significantly lower in the ASQ group than in the non-ASQ group (p = 0.03, ASQ group vs. non-ASQ group; 0.87 ± 0.21 V vs. 1.06 ± 0.36 V/0.4 ms).
Table 3: Electrical performance of left ventricular leads. View Table 3
Table 4 shows the echocardiographic LV ejection fraction (LVEF), LV end-diastolic volume (LVEDV), and LV end-systolic volume (LVESV) at 6 months after CRT implantation, with no difference in LVEF, LVEDV, and LVESV between the ASQ and Non-ASQ groups. In addition, a comparison of ΔLVEF (LVEF at 6 months after CRT implantation minus LVEF before CRT implantation), the rate of change in LVEF before and 6 months after CRT implantation, showed a significant improvement in LVEF in the ASQ group. However, in the so-called "responders" using LVESV as the index, there was no difference in the amount of decrease in LVESV (LVESV 6 months after CRT implantation minus LVESV before CRT implantation) or the rate of decrease in LVESV (LVESV decrease divided by LVESV before CRT implantation).
Table 4: Table of echocardiographic data 6 months after CRT implantation. View Table 4
Figure 4 shows the Kaplan-Meier survival curve for heart failure readmission and cardiac death events. Heart failure readmissions and cardiac deaths with an average observation period of 455 days were lower in the ASQ group than in the non-ASQ group. ASQ leads were involved in reducing the risk of heart failure readmissions and cardiac deaths by 67% (Log-rank test, p = 0.04, hazard ratio 0.33).
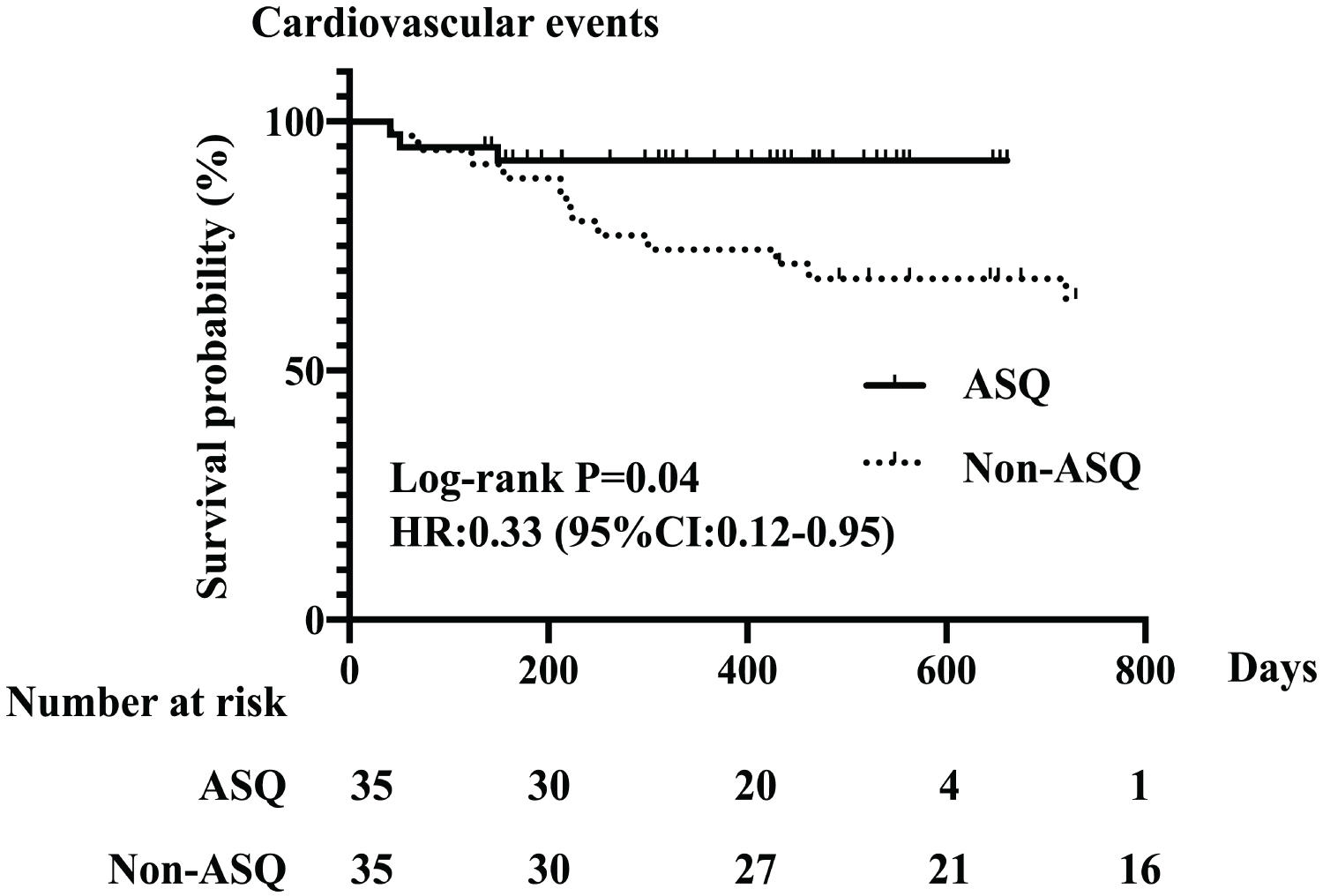 Figure 4: Kaplan-Meier curve for heart failure hospitalizations and cardiac death events. The Attain Stability Quad (ASQ) group exhibited lower event rates for heart failure readmission and cardiac death during an average observation period of 455 days than the non-ASQ group (log-rank test, p = 0.02, hazard ratio 0.33). Cardiovascular events: heart failure readmission and cardiac death.
View Figure 4
Figure 4: Kaplan-Meier curve for heart failure hospitalizations and cardiac death events. The Attain Stability Quad (ASQ) group exhibited lower event rates for heart failure readmission and cardiac death during an average observation period of 455 days than the non-ASQ group (log-rank test, p = 0.02, hazard ratio 0.33). Cardiovascular events: heart failure readmission and cardiac death.
View Figure 4
This study is a retrospective observational study comparing the new active fixation LV lead (ASQ lead) with the conventional passive fixation LV lead of CRT. Three points are described below as the findings obtained from this study.
The first notable feature garnered from the results of this study is the stability of a low pacing threshold in the remote period observed in CRT implantation patients using ASQ leads. The lower pacing threshold may be due to better contact with the LV resulting from the active fixation mechanism of the side helix. In addition, ASQ leads are associated with a lower incidence of lead dislodgement and phrenic nerve stimulation than are conventional quadrupole leads [5]. By using the side helix, which is a unique feature of ASQ leads, the stability of the basal CS, maximized by the vein diameter of the CS, is increased. ASQ leads also make LV pacing via a short and small CS branch possible [6]. Inamura, et al. reported on a new implantation technique that facilitates insertion of ASQ leads into bent CS branches, a difficult maneuver to achieve with conventional leads, while simultaneously reducing the LV pacing threshold and avoiding phrenic nerve stimulation [7]. Another report demonstrated that the use of ASQ leads resulted in a 98% LV lead implantation success rate, making it possible to select the most delayed site as the pacing site [8]. Based on the above, it is considered that the clinician greatly influences the LV lead determination process when selecting the type of LV lead for CRT.
The second advantageous characteristic of an ASQ lead is its ability to avoid the LV apical segment while enabling pacing at the midventricular LV segment, which cannot be achieved with the conventional LV lead. Previous studies have shown that ASQ leads showed a stable pacing threshold and avoided the apical segment, similar to the results of this study [9]. In this study, in the non-ASQ group, a CRT operator abandoned pacing from the midventricular to the basal segment of the LV by placing a lead on a small CS branch present at the apical segment, resulting in stable fixation and low pacing. The threshold may have been reached at the time of implantation. Similar studies have reported that ASQ leads were able to avoid LV pacing from the apical segment [8]. In addition, subgroup analyses of prospective randomized trials such as the Multicenter Automatic Defibrillator Implantation Trial–Cardiac Resynchronization Therapy (MADIT-CRT) and REVERSE trials showed that LV pacing from the apical segment showed less favorable clinical outcomes and was associated with high phrenic nerve stimulation [10,11].
Therefore, the midventricular to basal LV segments are clinically considered ideal target sites for indwelling LV leads. Situating LV pacing at the electrically delayed site has been shown to improve clinical outcomes for heart failure readmission and cardiac death [12].
The third advantageous feature of ASQ leads is demonstrated by the results of this study. The rates of heart failure readmission and cardiac death were lower in the ASQ group than in the non-ASQ group. The ASQ lead made it possible to avoid phrenic nerve stimulation and to perform LV pacing from a delayed optimal site in the LV. Therefore, this favorable clinical outcome, which has been reported in previous studies as a critical factor in both readmission rates for heart failure and cardiac death, is ascribed to the use of ASQ leads [13]. By using ASQ leads and avoiding the apical segment as an LV lead pacing site, CRT can result in good clinical outcomes, with a reduction in the readmission rates specifically for heart failure.
This is a small retrospective observational and nonrandomized study of 70 patients. It is also based on data that reflects routine clinical practice at our institution. In addition, various algorithms for optimizing CRTs were used in both groups. Moreover, LV leads were implanted by several different CRT implanters. Therefore, this study could not demonstrate that the LV lead was implanted at the site where the conduction was most delayed. Another limitation is that the use of ASQ leads in multivariate analysis of heart failure rehospitalization and cardiac mortality is not a statistically significant point.
ASQ leads were able to maintain a stable, low LV pacing threshold in the remote period after CRT implantation. Furthermore, ASQ leads avoided pacing from the apical segment of LV and enabled LV pacing on the lateral side and from the midventricular to the basal LV segment. The ASQ lead performs LV pacing from a delayed optimal site in the LV. Therefore, ASQ leads may contribute to the prevention of cardiovascular events.
We would like to thank Editage (www.editage.com) for English language editing. We would like to thank Yusha Izaki for the technical assistance.
No funding was received for this study.
The authors declare no conflict of interest for this article.
The study protocol was approved by the Institutional Committee on Human Resource at St. Marianna University School of Medicine (No. 4673).
Informed consent was obtained from all patients (via the opt-out method) at our institution.
N/A.
N/A.
The data that support the findings of this study are available from the corresponding author upon reasonable request.