Calciphylaxis is rare, life-threatening calcific uremic arteriolopathy in patients with end stage renal disease. Rarely, it can occur in patients with normal renal function known as non-uremic calciphylaxis. Very scant literature and few case reports are available about non-uremic calciphylaxis. We present a case of 51-year-old female with reduced LV ejection fraction as sequelae of peripartum cardiomyopathy on long term warfarin who presented with calciphylaxis lesions with normal renal function.
Calciphylaxis is known as calcific uremic arteriolopathy and characterized by thrombosis in small sized arterioles with calcific deposit along with dermis and sub-cutaneous fat. It is rare but life threatening complication almost always associated with end stage renal disease, However it can occur with normal renal function. There are few reported case of calciphylaxis occurs after kidney transplant with normal renal function [1]. Short Case series by Nigwekar, et al. [2] and Bajaj, et al. [3] establishes diagnosis of calciphylaxis with normal renal function. Calciphylaxis may be rarely associated with warfarin as side effect if anticoagulation is not under therapeutic range. We here report case of calciphylaxis in 51-year-old female patient after 20 years of taking warfarin and INR within therapeutic range.
A 51-year-old female presented with painful skin ulcer over right thigh for 1 month. Patient also had complaint of bilateral pedal oedema for 10 days and progressive breathlessness for 7 days. On arrival to hospital patients was breathlessness at rest and having orthopnoea (NYHA IV).
She was a diagnosed case of severe LV dysfunction (LVEF 25%) as sequel of peripartum cardiomyopathy 20 years back. She also had a history of venous thrombosis of right subclavian, internal jugular and axillary vein and APLA syndrome diagnosis was made. She was on warfarin for past 20 years with irregular follow up at another institution. She was on furosemide, spironolactone, metoprolol, ramipril, and warfarin, was apparently well before the development of skin lesion and her INR was in therapeutic range.
She noticed skin lesion over right thigh one month back which was insidious in onset and gradually progressing. Initial size of lesion was 1.0 × 2.0 cm, with dark reddish colour and edge was dark brown colour and limited to right thigh. Skin lesion was associated with intermittent excruciating pain; pain was somewhat relieved with analgesics. Skin lesion progressed to other thigh also and pain was increasing in severity. She developed progressive bilateral pedal oedema 2 weeks back. Patient also becomes breathlessness while brisk walk and climbing 2 floors. Breathlessness was rapidly progressed to rest (NYHA IV) within 7 days and she was admitted at our institution with acute heart failure.
On clinical examination patients had tachycardia and tachypenic with narrow pulse pressure. On auscultation bilateral basal crepitation in chest and gallop was present. She was managed with intravenous diuretic, low dose inotropic support and Non-invasive ventilation (Bipap) for symptomatic improvement. On examination, skin lesion was firm to hard, indurate plaque with overlying skin showing ecchymosed and bullae on Right thigh and few purpuric non indurated lesions on left thigh (Figure 1).
 Figure 1: On presentation skin lesion.
View Figure 1
Figure 1: On presentation skin lesion.
View Figure 1
Initial possibility of warfarin induces skin necrosis was made, but her INR (2.3) was within therapeutic range on admission. Patient's routine blood investigations were normal (Table 1). Parathyroid and Thyroid profile, ANA by IF and ANA profile were normal. Anticardiolipin antibodies were positive for patient. Ultrasonogram of right thigh shows mild subcutaneous oedema along the antero-medial aspect of right thigh around the ulcerated lesion and underlying muscular plane appeared normal. Bilateral lower limb arterial Doppler study shows diffuse calcified bilateral below the knee vessel, no evidence of flow limiting plaque or thrombus. MRI of lower limb shows variable fatty infiltration and atrophy of muscles of the gluteal and thigh region, Active myofascial and subcutaneous oedema seen in the bilateral proximal thigh, more on the right side. No bony involvement seen in MRI pelvic region.
Table 1: Routine blood investigation on admission. View Table 1
Skin punch biopsy was done at the edge of lesion. Biopsy shows extensive necrosis of epidermis and dermis. Patchy necrosis of subcutaneous fat and medium sized blood vessel deep within subcutaneous fat showed extensive calcification in media. Von kossa stain for calcium confirmed calcification (Figure 2 and Figure 3).
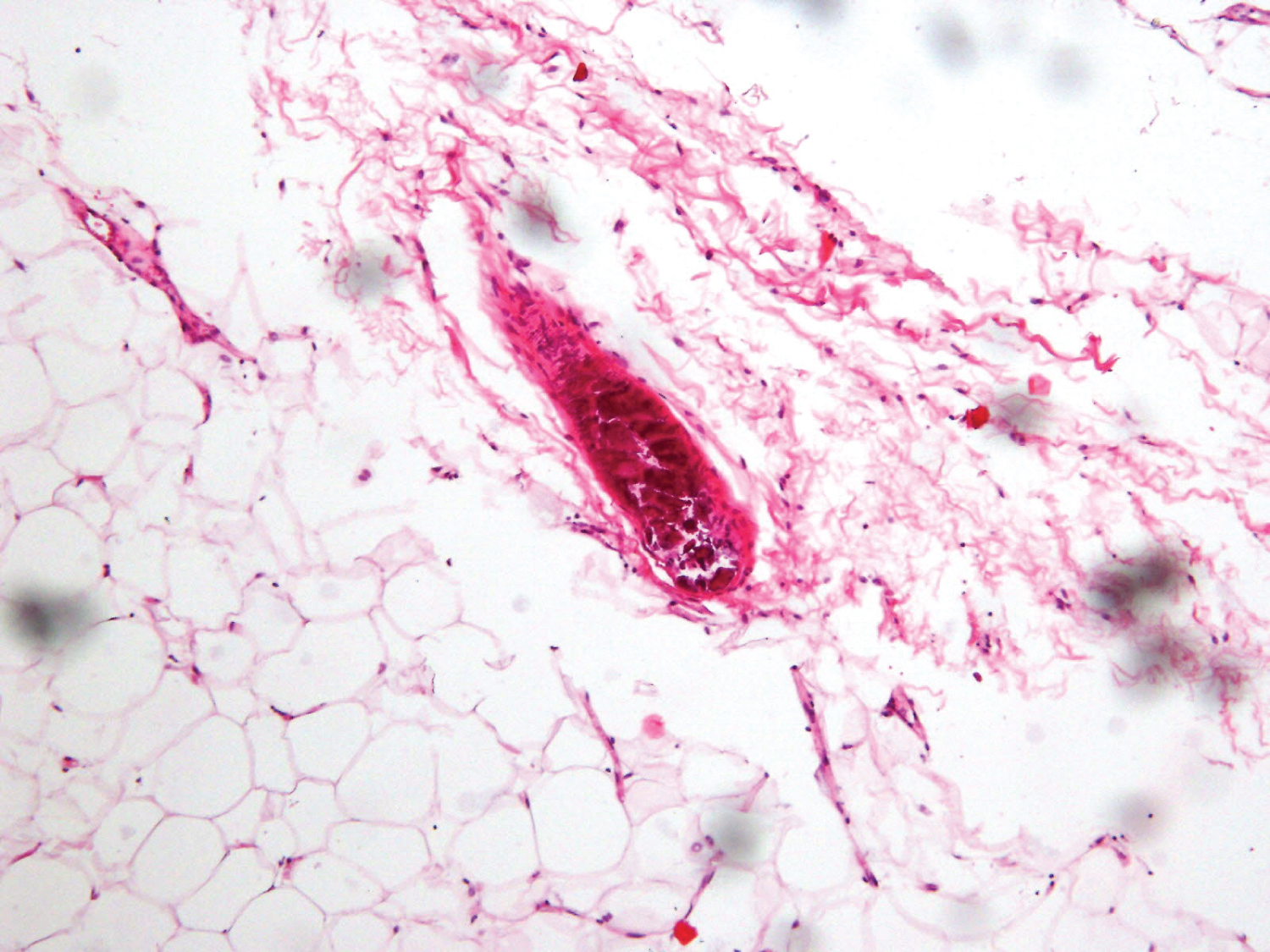 Figure 2: Deposition of calcium in the wall of medium sized blood vessels in the subcutaneous fat, obliterating the lumen (H&E 200×).
View Figure 2
Figure 2: Deposition of calcium in the wall of medium sized blood vessels in the subcutaneous fat, obliterating the lumen (H&E 200×).
View Figure 2
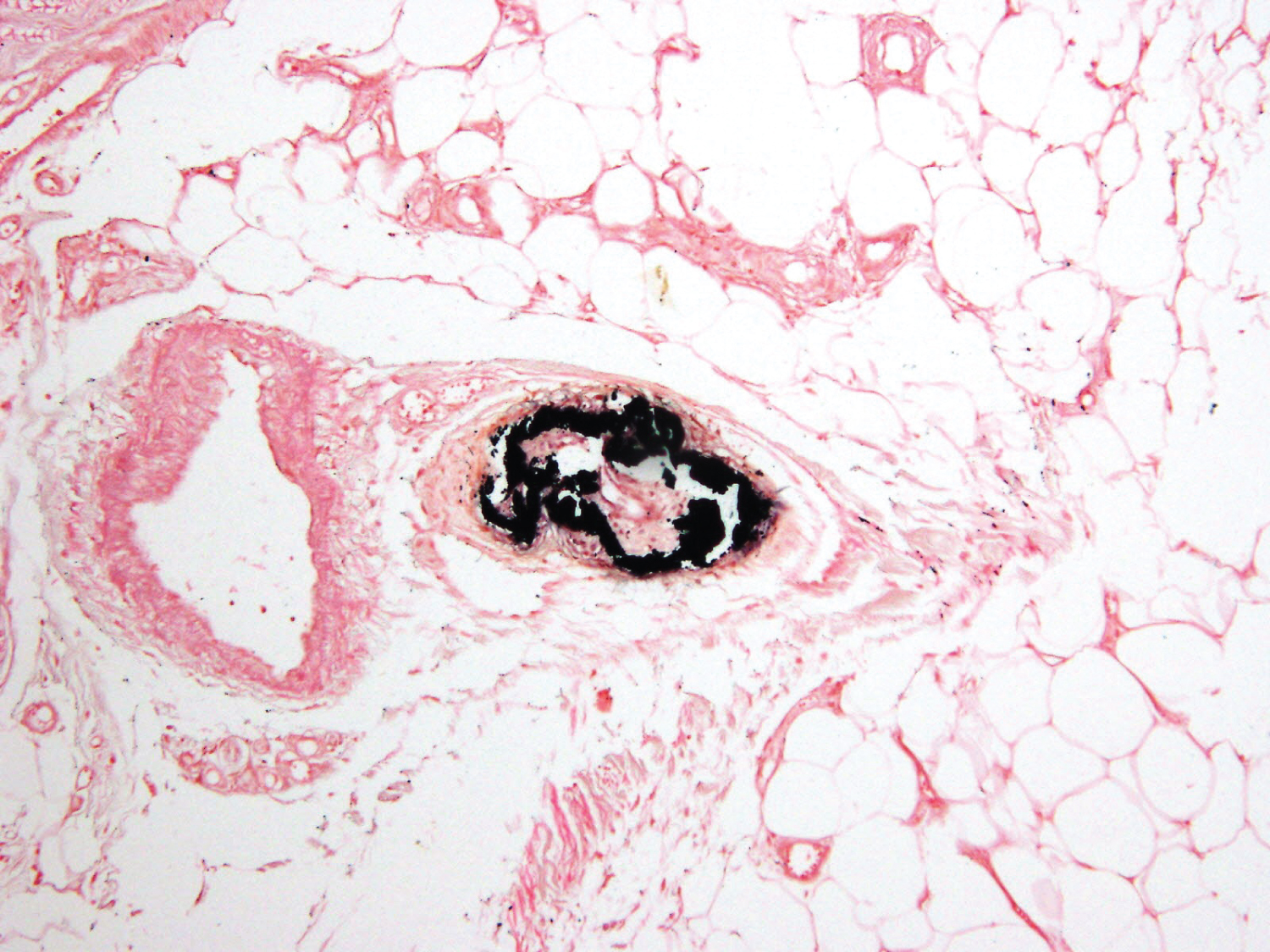 Figure 3: Calcium deposits in the wall of the blood vessel stained black by Von Kossa stain for calcium.
View Figure 3
Figure 3: Calcium deposits in the wall of the blood vessel stained black by Von Kossa stain for calcium.
View Figure 3
A diagnosis of non-uremic calciphylaxis was made. Patient was started on sodium thiosulphate pulse doses (25 grams over 30 minute every 3rd day) and wound dressing and bandaging was done daily. For initial 2 weeks skin lesion progressed. Left thigh lesion increased and spread to whole medial aspect with blackish discolouration with white exudates (Figure 4). After 2 weeks there was stabilisation of skin lesions and no further increased in size. Sodium thiosulphate bolus doses were continued for next 4 weeks with mild improvement of skin lesions at the edges was seen. A patient was discharge in stable condition and she was advice for thrice weekly sodium thiosulphate infusions at home. Unfortunately 3 days after discharge, patient succumbed at home due to sudden cardiac death.
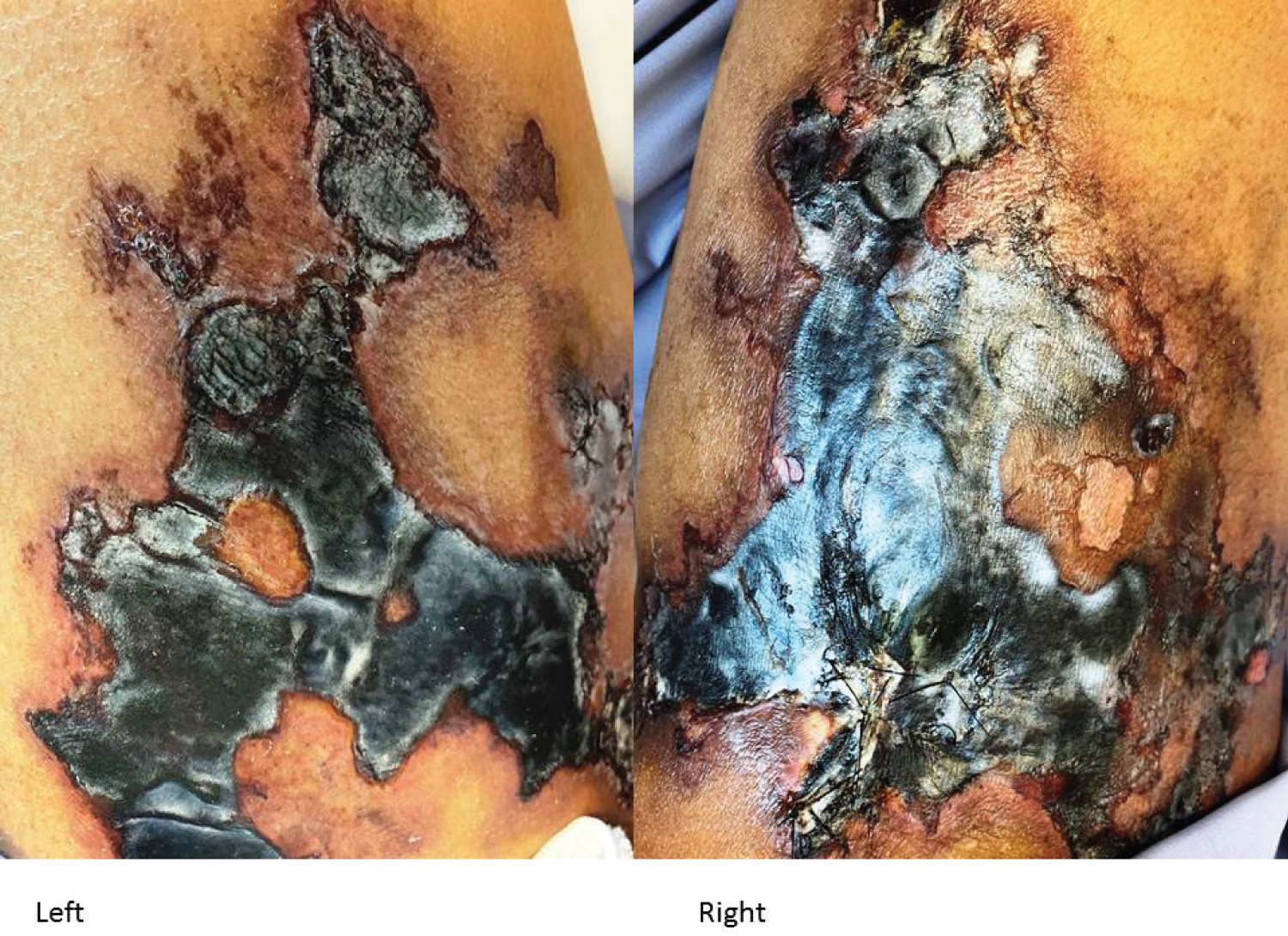 Figure 4: Skin lesion at the time of biopsy.
View Figure 4
Figure 4: Skin lesion at the time of biopsy.
View Figure 4
Calciphylaxis is life threatening condition with 1 year mortality of up to 80%, predominantly found in patients with end stage renal disease on Maintenance hemodialysis [3]. A systemic review by Bajaj R, et al. shows that with normal renal function main associated risk factor were obesity, vitamin K antagonist drugs and Diabetes mellitus [3]. Calciphylaxis is usually presents with painful skin lesion involving lower limbs, abdomen and buttocks. The presentation is no different than calciphylaxis in patients with end stage renal disease [2], but with normal renal function there is delay in the diagnosis up to 2-12 weeks in Bajaj R, et al. In our case late presentation and delay to get medical treatment were leads to extensive skin lesion.
The exact mechanism of action of vitamin K antagonism leads to calciphylaxis is unclear, but the proposed pathogenesis is alteration of in the activity of matrix GLA protein which is potent calcification inhibitor that depends on Vitamin K for its activation. Warfarin may inhibit vitamin K-dependent carboxylation of matrix-GLA protein, decreasing the activity of the protein to inhibit calcification locally. The histopathologic picture of prominent soft tissue calcification and calcification of vessels seen on Doppler findings seemed to support that view [4-6].
Currently there are no guidelines to treat calciphylaxis in patient with normal renal function, but based on case series most of patients treated with sodium thiosulphate, analgesics for pain, local wound care and use of alternative than Vitamin K antagonism drugs like Heparin and Newer oral anticoagulants [7]. Improved survival rate is noted in various recent case series with use of sodium thiosulfate [8]. In our case we gave sodium thiosulphate in bolus dose every 3rd day during hospitalization. Our case shows some improvement after 4 weeks of treatment.
Our case is unique in presentation as after almost 20 years of taking vitamin k antagonist medication patients develops calciphylaxis. Previously longest duration of warfarin induced calciphylaxis was 168 months (average 32 months) noted in review by Yu WY, et al. [9]. Good Survival rate reported by Yu Wy, et al. (83%) may be due lesion involvement difference, majority had below knee involvement. Early Improvement in skin lesion in our case then other reported case is may be due to no alteration baseline calcium metabolism, which is present in almost all cases with renal dysfunction.
Calciphylaxis can occur at any time after initiation of warfarin so patient on warfarin and skin lesion should be treated cautiously. Early involvement of Dermatologist and Nephrologists may be rewarding.