Brugada syndrome, Syncope, Arrhythmia, ICD
In 1992, Brugada syndrome (BrS) was described for the first time as a pattern of ST-segment elevation in right precordial electrocardiography (EKG) leads with a high incidence of unexplained cardiac arrest (UCA) and sudden cardiac death (SCD) in patients with structurally normal hearts [1]. It is associated with an autosomal dominant genetic predisposition. Therefore, in the case of diagnosed UCA or SCD, first-degree relatives are advised to be screened for cardiac abnormalities [2]. The characteristic EKG changes of the Brugada pattern could sometimes be transient or variable over time. There are some known provoking factors such as fever, medications, and toxins [3]. In this case, we present a 23-year-old Caucasian male patient with a long-standing history of substance abuse who presented with syncope. Electrocardiography performed by emergency medical services (EMS) showed a Brugada pattern.
A 23-year-old Caucasian male patient with a long-standing history of substance abuse, presented with syncope. When emergency medical services arrived, the patient had supraventricular tachycardia of around 180 beats per minute and subsequently cardioverted at 50 J on site. They attempted to reverse the patient's somnolence with Narcan, first intranasal then intravenous, without improvement. Upon arrival at the emergency department, the patient had a witnessed episode of what appeared to be seizure activity with foaming through the mouth. EKG at the time showed a Brugada EKG pattern (Figure 1). He was febrile with a temperature of 103 F. The patient's toxicity profile was positive for both Amphetamine and cannabinoid. Creatine Kinase was > 4000 I Unit\L and Troponin I was 2.38 ng\ml which suggested rhabdomyolysis. While hospitalized, the patient had another seizure-like episode while on telemetry, which showed sinus rhythm at the time of syncope. Cardiac MRI was negative for structural abnormalities. His family history was significant for SCD in his 40-years-old aunt. We contemplated the idea of placing an implantable cardioverter defibrillator (ICD). However, since he had another seizure while on telemetry without EKG abnormalities, we opted to place an Implantable Loop Recorder (ILR) instead, before discharge.
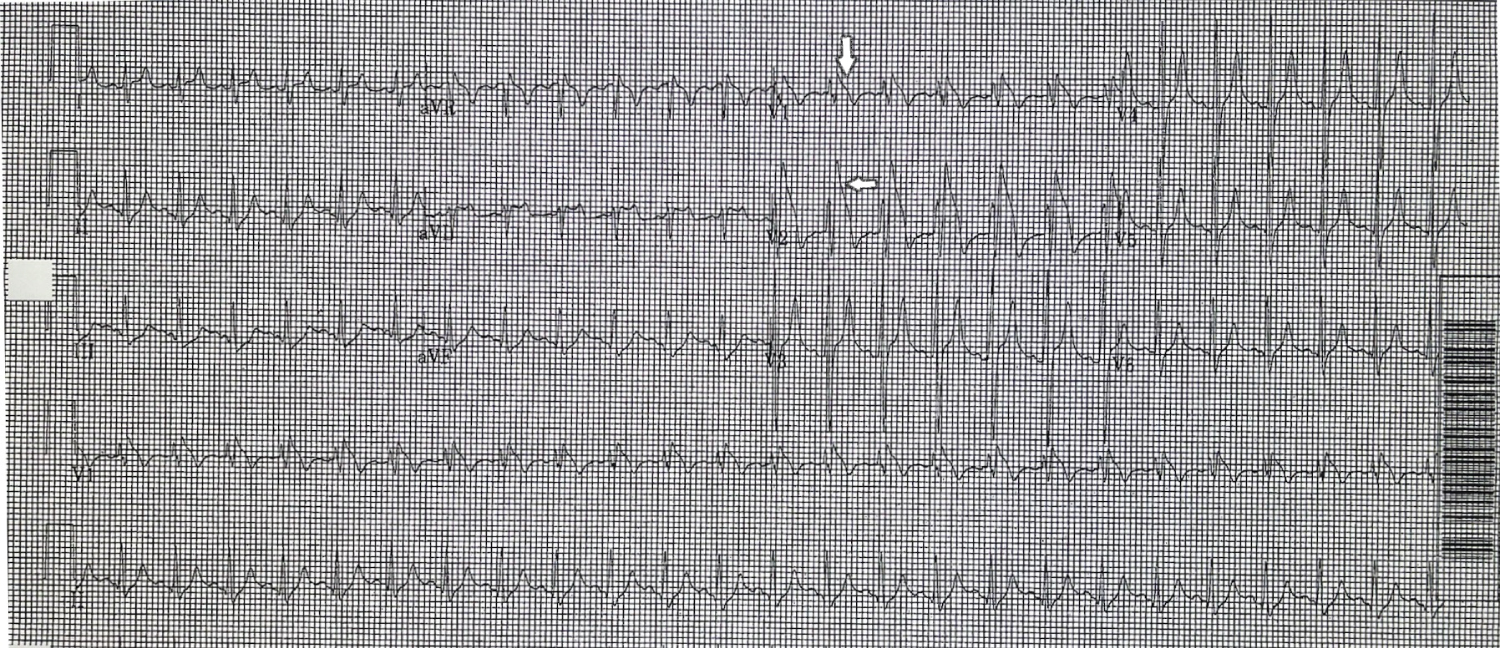 Figure 1: EKG showing descendent ST-segment elevation with negative T waves (white arrows) in the right precordial leads V1 and V2.
View Figure 1
Figure 1: EKG showing descendent ST-segment elevation with negative T waves (white arrows) in the right precordial leads V1 and V2.
View Figure 1
Brugada pattern on EKG associated with syncope is worrisome for a diagnosis of Brugada syndrome which puts patients at high risk for sudden cardiac death and requires an ICD placement by the guidelines. The patient's family history further makes this diagnosis more likely. However, given the absence of a Brugada pattern on EKG during the second episode, and given his history of substance abuse, we elected against immediate ICD placement in this case as the Brugada pattern was probably brought up by the fever and the patient likely does not have Brugada syndrome. His young age is also another reason to hesitate in placing ICD unless proven to be necessary. Provocative testing for Brugada is another possibility that we will consider in follow-ups.
Brugada pattern describes asymptomatic patients with EKG findings of a pseudo-right bundle branch block and persistent ST segment elevation in leads V1 to V2 with no other clinical criteria. It can be discovered in casual EKG or as part of the screening of first-degree relatives of a Brugada proband. There are two main types of Brugada EKG patterns. Type one is when the elevated ST segment is more or equal to 2 mm descends with an upward convexity to an inverted T wave. This is referred to as the "coved type" Brugada pattern. Type two is when the ST segment has a "saddle back" ST-T wave configuration. In which the elevated ST segment descends toward the baseline, then rises again to an upright or biphasic T wave [2]. In some patients, the characteristic EKG changes of the Brugada pattern are transient or variable over time. Brugada pattern can be provoked by fever, medications (eg. class 1c antiarrhythmic agents, Beta blockers, tricyclic or tetracyclic antidepressants), metabolic disturbance (eg. severe hyperkalemia), and toxins (eg. Alcohol and Cocaine).
On the other hand, Brugada syndrome is a symptomatic Brugada pattern with one or more of these clinical criteria: Sudden cardiac arrest (SCA), episode of syncope due to tachyarrhythmia cause, palpitation due to related atrial fibrillation, nocturnal agonal respiration, and arrhythmic events.
SCA occurs in one-third of the patients due to nonstructural ventricular tachyarrhythmia, most often presented as ventricular fibrillation (VF) or polymorphic ventricular tachycardia. SCA is usually not associated with exercise, and it's more common at night and during sleep. It is very important to differentiate episodes of syncope due to tachyarrhythmia cause from syncope due to non-arrhythmic causes (eg, neurocardiogenic), which could happen with a benign prognosis. Palpitation due to related atrial fibrillation (AF) occurs in 10 to 20 percent of patients with Brugada syndrome. The presence of AF is associated with increased disease severity and a higher risk of VF. On the other hand, palpitations related to ventricular tachyarrhythmia are not common. Nocturnal agonal respiration may represent aborted cardiac arrhythmias and is considered an ominous symptom. Arrhythmic events generally occur between the ages of 22 and 65 years and peak between 38 and 48 years. They are rare in children. However, patients with ventricular premature beats or non-sustained ventricular tachycardia are generally not considered as Brugada syndrome but Brugada pattern.
In the case of an EKG showing a Brugada pattern, all additional tests should be done to exclude underlying heart disease (eg. myocardial ischemia). Then evaluate the risk through electrophysiology testing, signal-averaged EKG, 12-lead EKG, and drug challenge in specific cases. Genetic testing (eg. SCN5A, SCN10a genes) should also be done for Brugada syndrome probands. In the end, an implantable cardioverter-defibrillator (ICD) should be applied in case one of documented ventricular fibrillation, polymorphic ventricular tachycardia, unexplained syncope strongly suggestive of a tachyarrhythmia, or nocturnal agonal respiration in the setting of type 2 Brugada pattern.
Fever is a common source for the Brugada pattern; a study that assessed the prevalence of the Brugada pattern in consecutive patients with fever showed that type I Brugada pattern was 20 times more prevalent among febrile patients. In the same study, all patients with fever-induced type I Brugada pattern were asymptomatic and remained so during 30 months of follow-up. The study concluded that type I Brugada pattern is definitively more common among patients with fever, suggesting that asymptomatic Brugada pattern is more prevalent than previously estimated [4].
Brugada patterns are masked and usually are due to provocative factors, such as fever. It is important to screen family members of SCD victims and to keep in mind the Brugada EKG pattern as a differential diagnosis of ST-segment elevation in anterior precordial leads of EKG. It is also important to mention that some Brugada pattern cases, such as fever-induced Brugada pattern, can be safely monitored, and usually do not require ICD placement.
None.
The authors declare that there is no conflict of interest.
The authors are grateful to the associate editor for the comments provided, which significantly improve the manuscript's clarity.
Written informed consent was obtained from the patient to publish this report following the journal's patient consent policy.