Constrictive pericarditis (CP) can occur secondary to multiple etiologies such as idiopathic pericarditis, post-cardiovascular surgeries, post-chest radiation therapy, and rarely rheumatologic diseases. We report a rare case of a 41-year-old male who was found to have IgG4-related disease (RD) manifesting as isolated constrictive pericarditis treated with pericardiectomy and immunosuppressive agents.
IgG4-related disease, Constrictive, Pericarditis, Pericardiectomy, Immunosuppressive
IgG- related disease (RD) is an immune mediated disease characterized by multiorgan fibrosis, elevated IgG4 serum concentration, and dense lymphoplasmacytic infiltration. Visceral involvements of lacrimal glands, lungs, pancreas, retroperitoneum, and kidneys have been well documented in the literature; however, cardiovascular manifestations are under-recognized. We, herein, report a case of 41-year-old male found to have isolated IgG4-RD constrictive pericarditis responding to pericardiectomy and immunosuppression agents.
A 41-year-old male with past medical history of tobacco use, hypertension, hyperlipidemia, anxiety, depression, insomnia, and COVID-19 infection a year prior to presentation presented to his primary care physician with a year-long history of nausea, vomiting, and 50-55 lbs unintentional weight loss. Upon evaluation, vital signs were within normal limits and physical examination was unremarkable. Initial work up with CT chest, abdomen, and pelvis demonstrated bilateral pleural effusions, pericardial thickening, and ascites. Transthoracic echocardiogram, thoracentesis and comprehensive serum studies were performed. Transthoracic echocardiogram revealed findings concerning for constrictive pericarditis and patient was referred to cardiology for additional evaluation. Initial differential diagnosis included idiopathic or viral constrictive pericarditis as it is the most common etiology for constrictive pericarditis. Patient did not have any recent cardiothoracic surgeries or radiation therapy.
A Thoracentesis was performed revealed transudative pleural fluid, negative for malignancy and negative AFB culture. Serum ANA and anti-ds-DNA levels were normal. Viral serologies including HIV were nonreactive. Transthoracic echocardiogram revealed normal left ventricular ejection fraction (LVEF) of 55%, thickened pericardium with evidence of myocardial-pericardial tethering of left ventricular apical segments and signs of ventricular interdependence. There was leftward deviation of the interventricular septum during early diastole followed by “bounce back” or rightward deviation with late diastolic filling due to the lack of pericardial compliance, also known as “septal bounce”, highly suggestive of constrictive pericarditis (Figure 1 and Video 1).
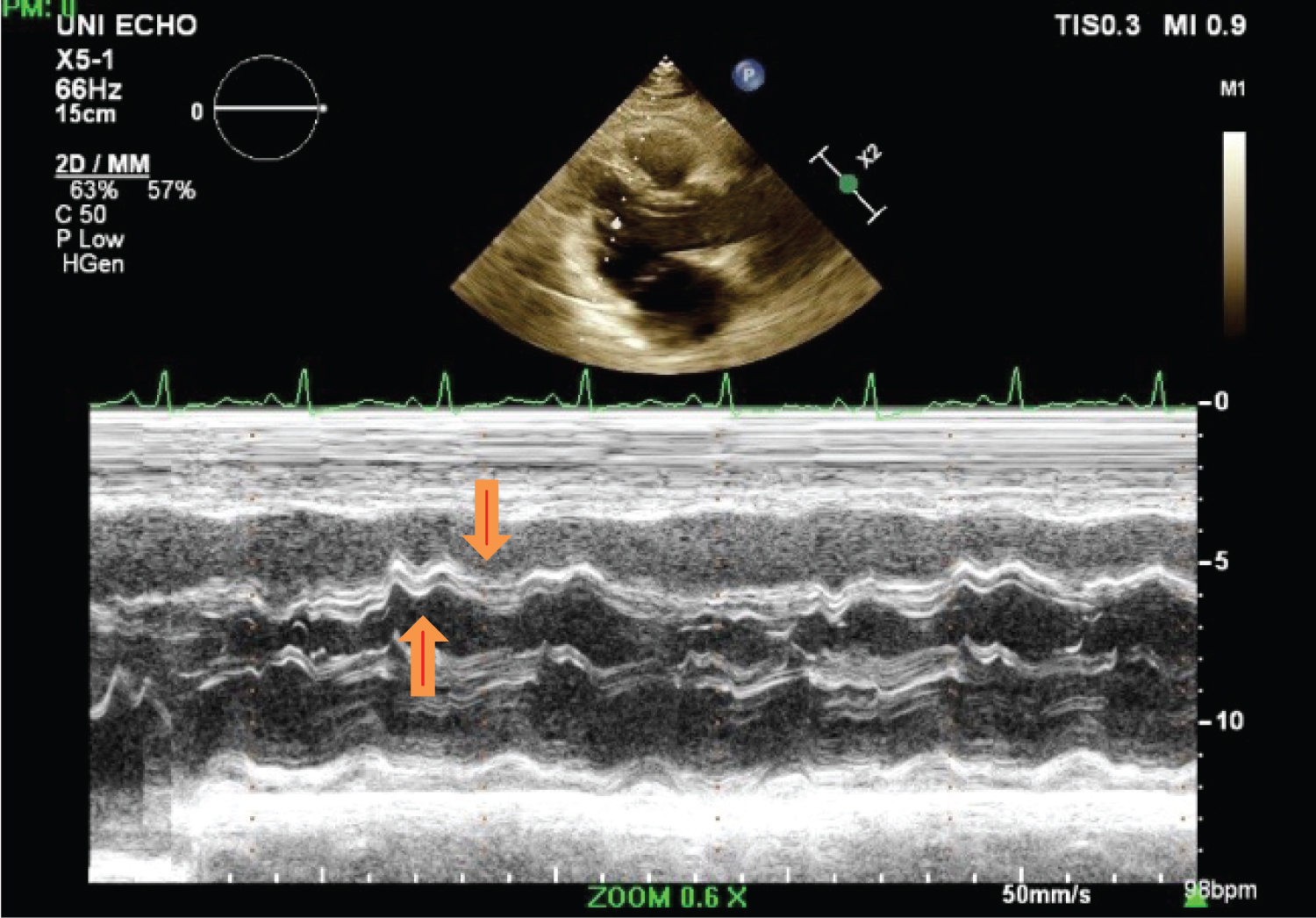 Figure 1: M-mode echocardiogram showing interventricular dependence with inspiratory bulge of the interventricular septum from right to left (downward arrow) and left to right bounce with expiration (upward arrow).
View Figure 1
Figure 1: M-mode echocardiogram showing interventricular dependence with inspiratory bulge of the interventricular septum from right to left (downward arrow) and left to right bounce with expiration (upward arrow).
View Figure 1
Video 1: Constrictive pericarditis.
Further work up was performed including cardiac catheterization (Figure 2). This revealed normal coronary arteries and various findings consistent with CP. The simultaneous LV and Pulmonary capillary wedge pressure (PCWP) tracing revealed discordance between the intra- and extra-pericardial pressures. This was due to limited transmission of respirophasic changes in intrathoracic pressure across the thickened pericardium to the cardiac chambers, resulting in a much greater variation in PCWP tracing with respiration compared to LV pressure tracing. The intracardiac pressure tracings also revealed square root sign and equilibrium or near-equilibrium of left and right diastolic pressures. Cardiac MRI (CMR) further reaffirmed the findings of pericardial thickening, apical pericardial tethering, and ventricular interdependence (Figure 3 and Figure 4).
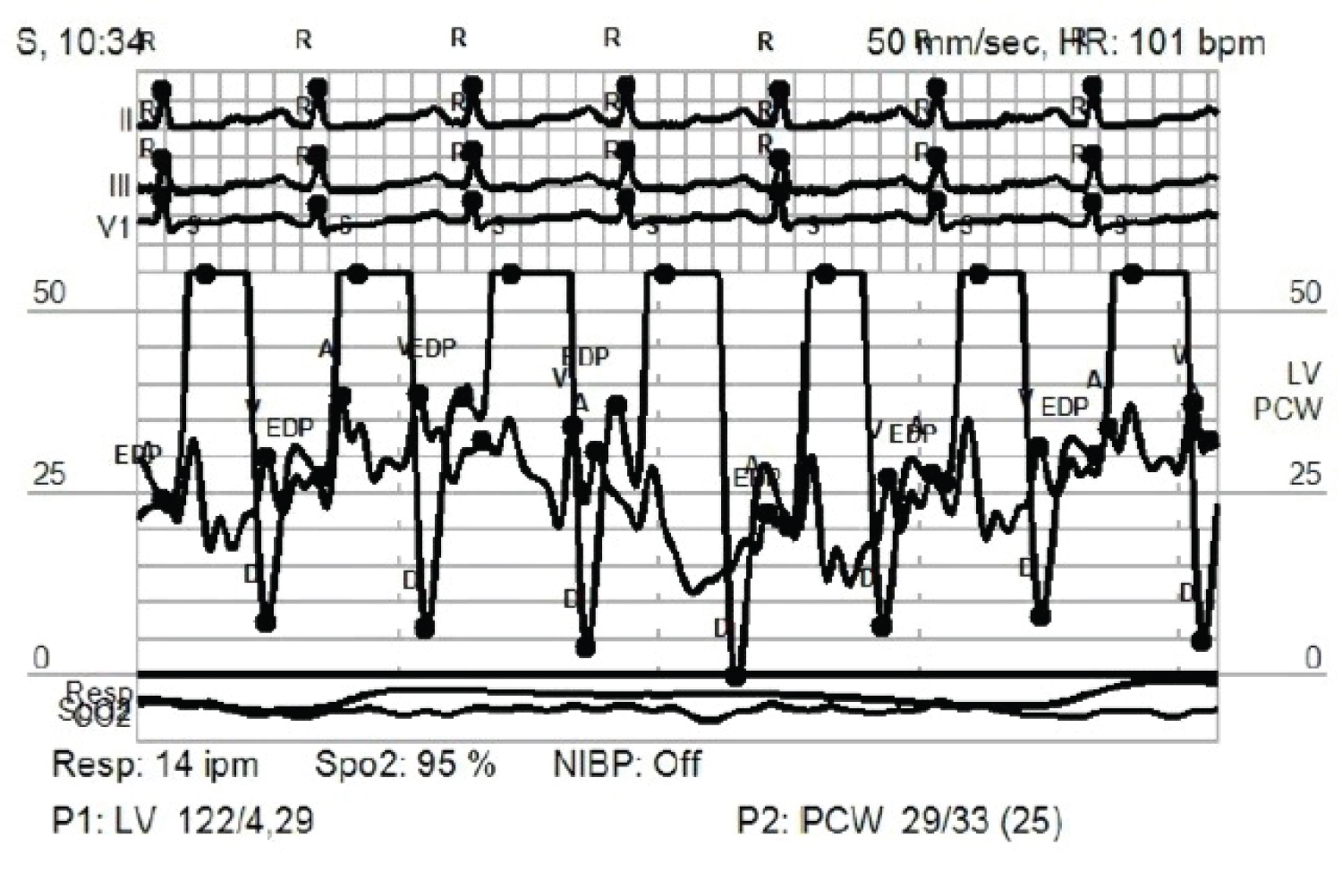 Figure 2: Simultaneous LV-PCWP tracing showing square root sign and equilibrium or near-equilibrium of left and right diastolic pressures.
View Figure 2
Figure 2: Simultaneous LV-PCWP tracing showing square root sign and equilibrium or near-equilibrium of left and right diastolic pressures.
View Figure 2
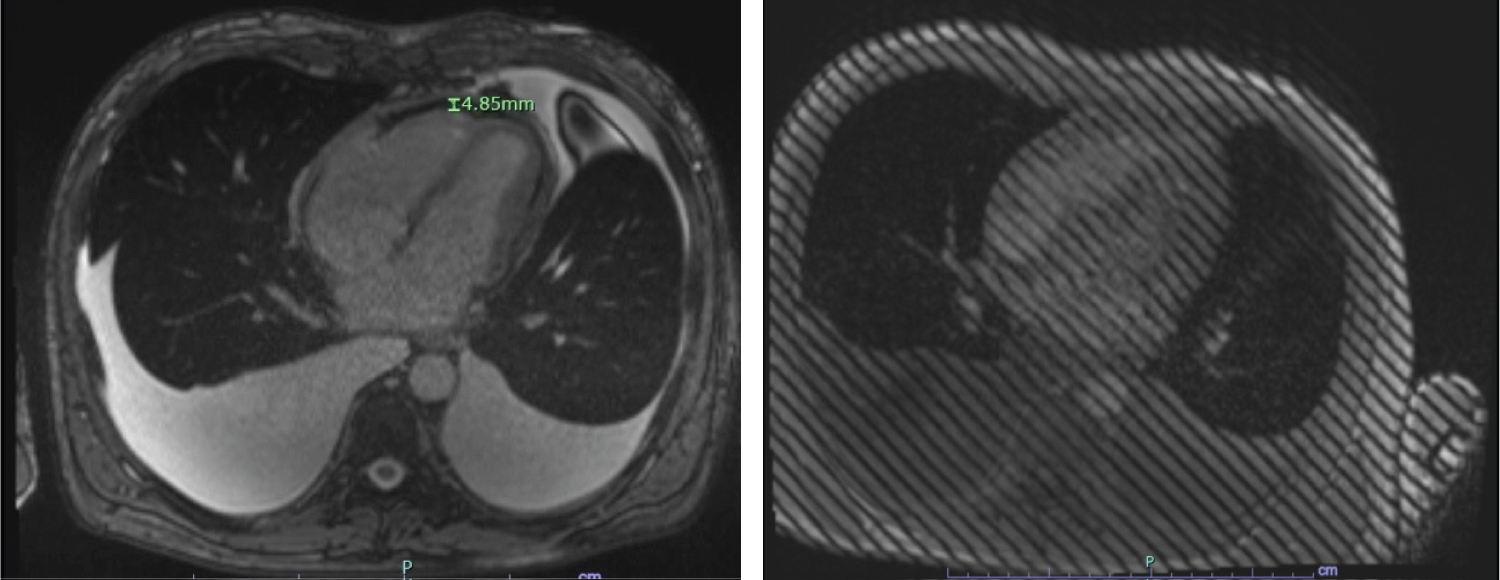 Figure 3: A) CMRI showing 4.85 mm pericardial thickening; B) Tagged cine MRI showing adhesion of pericardium to myocardium.
View Figure 3
Figure 3: A) CMRI showing 4.85 mm pericardial thickening; B) Tagged cine MRI showing adhesion of pericardium to myocardium.
View Figure 3
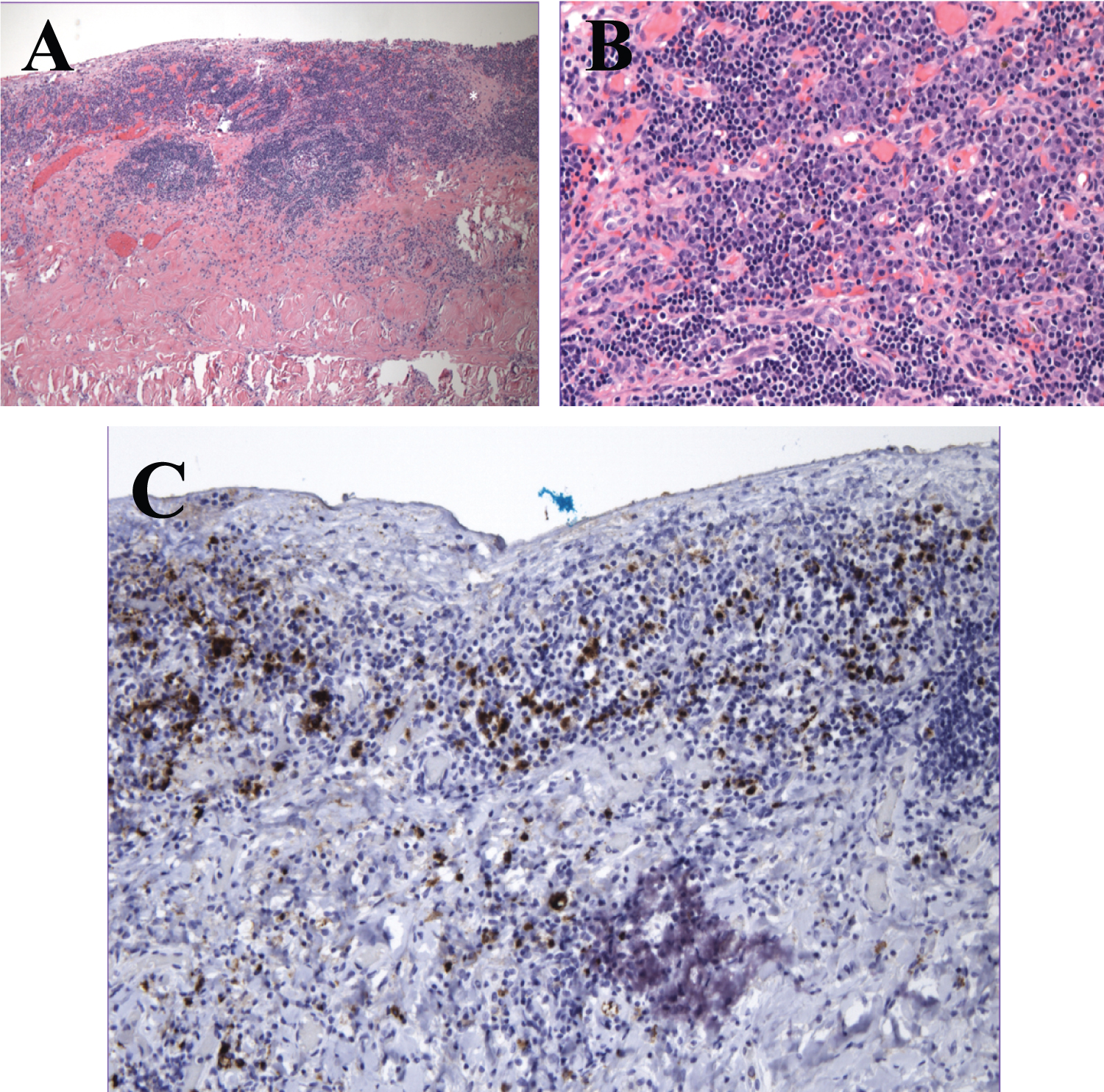 Figure 4: A) H&E 40× - Pericardium with focally storiform fibrosis and a dense chronic inflammatory infiltrate; B) H&E 200× - High power view of the infiltrate showing lymphocytes and plasma cells with a plasmocytic predominance; C) IgG-4 stain 100× - Greater than 40% of the plasma cells stain for IgG-4 with greater than 30 IgG-4 positive plasma cells per high power field.
View Figure 4
Figure 4: A) H&E 40× - Pericardium with focally storiform fibrosis and a dense chronic inflammatory infiltrate; B) H&E 200× - High power view of the infiltrate showing lymphocytes and plasma cells with a plasmocytic predominance; C) IgG-4 stain 100× - Greater than 40% of the plasma cells stain for IgG-4 with greater than 30 IgG-4 positive plasma cells per high power field.
View Figure 4
Shortly after, the patient developed worsening symptoms dyspnea on exertion, worsening ascites, and lower extremity edema. Due to progressive symptoms, he underwent a complete pericardiectomy. Pericardial pathology showed densely fibrotic tissue with focal dense lymphoplasmacytic inflammation with IgG4 positivity > 30 plasma cells/HPF and IgG4 positive plasma cell/total plasma cell ratio > 40%. Serum IgG4 was elevated to 123 mg/dl and IgGA 482 mg/dl. No alternate inflammatory or rheumatologic disorder associated with high serum IgG4 was identified. The post-surgical course was complicated by takotsubo cardiomyopathy with EF 23% and LV thrombus with subsequent LVEF recovery to 61% within 10 days. Patient was started on prednisone 30 mg daily for 4 weeks with plans for tapering over 2 to 3 months. He was additionally initiated on Azathioprine 50 mg twice a day. Repeat imaging with CT chest, abdomen, and pelvis obtained with no additional organ involvement identified. At two-month follow-up, patient was doing well on azathioprine with no signs of additional organ involvement. Follow up echocardiogram revealed normal LV function and inferior vena cava dynamics suggestive on normal right atrial pressure.
CP is an uncommon disease entity characterized by fibrous thickening or calcification of the pericardium leading to pericardial non-compliance [1]. Common etiologies are idiopathic pericarditis, post-cardiovascular surgeries, post-chest radiation therapy, and rarely rheumatologic diseases. Immune mediated disease accounts for 3-7% of CP cases [2] with rare association with IgG4-RD: A fibro-inflammatory disease commonly seen with pancreatic involvement but rarely with pericardial involvement.
Diagnosis of CP can be challenging therefore good history and physical exam are key along with imaging modalities for confirmation. As the pericardium loses its reserve volume, two pathophysiologic principles become evident: Dissociation of intrathoracic (PCWP) and intracardiac pressures (LV diastolic) and ventricular interdependence [3]. Dissociation of intrathoracic and intracardiac pressure occurs because during respiration, the intrathoracic pressure varies significantly, however the stiffened pericardium limits the degree of transmission of intrathoracic to intracardiac pressure resulting in a lesser change in intracardiac pressure. Similarly, during inspiration there is an increase in venous return to the right heart. However, the constrained pericardium limits cardiac compliance, thus the intraventricular septum shifts leftward to accommodate the additional volume during inspiration and vice versa during expiration resulting in ventricular interdependence (Video 1) [1,3,4].
Clinically, patients present with signs of volume overload, predominantly lower extremity edema, pleural effusions and ascites that are a result of unsatisfactory diastolic filling. Echocardiogram is the first line imaging modality for assessment of hemodynamic and structural changes. In cases where CP is suspected, cardiac catheterization can be used to further evaluate cardiovascular hemodynamics and confirm presents of constrictive physiology. Meanwhile, cardiac CT and CMR aid in assessment of cardiac anatomy and pericardial thickening. There is some evidence suggesting that T2-weighted short-tau inversion recovery and late gadolinium enhancement sequences can be valuable tool to assess extent of pericardial edema and inflammation and can help guide decision regarding use of anti-inflammatory therapy [5].
Even though radiographic images and serologies can assist with IgG4-RD diagnosis, histopathologic assessment of the affected organs remains the gold standard. IgG4-RD classically features a dense lymphoplasmacytic infiltrate, increased IgG4 positive plasma cells, storiform fibrosis, and obliterative phlebitis. Histologic sections from this patient's pericardial tissue show a dense lymphoplasmacytic infiltrate with increased IgG-4 staining plasma cells and patchy storiform fibrosis. Pathologic diagnosis of IgG4 related disease is somewhat site specific, but generally requires an increased number of IgG4 positive plasma cells and at least one of the three other histologic criteria [6].
In management of IgG4-RD, glucocorticoids are used as first line agents, as was seen in our case. However, relapse can occur during tapering. Therefore, glucocorticoids sparing immunosuppressive agents are considered such as azathioprine, mycophenolate, or rituximab.
Even though majority of IgG4-RD CP cases end up requiring pericardiectomy, Sekiguchi, et al. and Yuriditsky, et al. reported cases of complete or near complete resolution of CP with glucocorticoids [7,8].
IgG4-RD is a rare cause of isolated constrictive pericarditis however it should be considered as a potential diagnosis in patients presenting with concerning constellation of symptoms without alternative etiology. Early diagnosis and management with glucocorticoids followed by glucocorticoids-sparing agents for maintenance therapy are critical to prevent or slow down fibrotic changes.
The authors have nothing to disclose.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent was obtained from patient for publication of this case report including accompanying images.