Introduction: Anomalous origin of the right coronary artery (RCA) from the pulmonary artery (ARCAPA) is a rare congenital heart disease with varied clinical presentations, ranging from an asymptomatic murmur to sudden death. Surgery to rebuild the physiological coronary system is strongly recommended to prevent complications.
Case description: Herein, we report the case of a 46-year-old woman who presented with a 2 months history of dyspnea upon performing activities. Transthoracic echocardiography revealed rheumatic heart disease with multivalve involvement and an anomalous origin of the RCA. ARCAPA was further corroborated by the findings of coronary angiography. Ultimately, RCA re-implantation into the aorta with mitral and aortic valve replacements was performed.
Conclusions: The patient was followed up for approximately 10 years without any recurrent clinical manifestations.
ARCAPA, Right coronary artery, Rheumatic heart disease, Surgery, Case report
Anomalous origin of the right coronary artery (RCA) from the pulmonary artery (ARCAPA) is a rare con-genital heart condition, which has been attributed to a developmental anomaly of the aortic septum [1]. Although it has varied clinical symptoms, ARCAPA is a life-threatening disease due to imminent myocardial ischemia; therefore, surgical treatment is highly recommended even in asymptomatic patients. Herein, we present the case of a 46-year-old woman with ARCAPA complicated by rheumatic heart disease who underwent surgery and was followed up for 10 years.
A 46-year-old woman with no previous medical or family history of cardiac disease presented with a 2-month history of dyspnea upon performing activities. Physical examination revealed a systolic heart murmur of grade 3/6, which was best heard on the left lower sternal border. However, other examinations were unremarkable.
Transthoracic echocardiography was performed, which revealed rheumatic heart disease with multivalve involvement, including moderate mitral stenosis, moderate mitral insufficiency, and moderate aortic stenosis. Additionally, the image suggested an abnormal origin of the RCA. To ascertain the exact diagnosis and determine the condition of the coronary artery, coronary angiography was then performed. Angiography revealed collateral blood flow from the left coronary artery (LCA) to the RCA and delayed retrograde filling of the RCA via the collateral vessels back to the ostium into the pulmonary artery (PA) (Figure 1A). Electrocardiography and chest radiography were normal. Based on these findings, a diagnosis of ARCAPA was confirmed (Video 1 and Video 2).
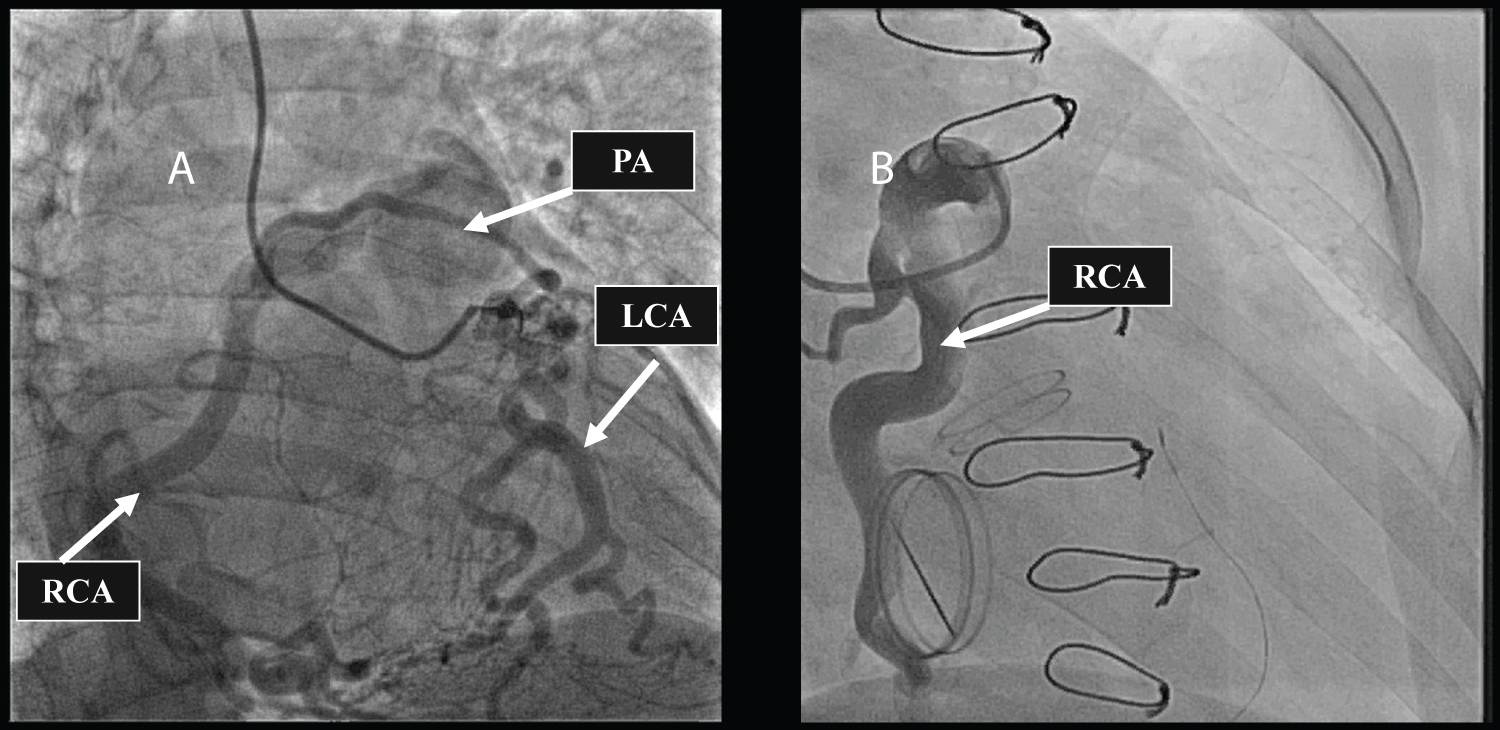 Figure 1: A) Preoperative coronary angiography showed the anomalous origin of the right coronary artery arising from the pulmonary artery and collateralization between the left coronary artery and the right coronary artery; B) Postoperative coronary angiography showed the anomalous origin of the right coronary artery arising from the pulmonary artery.
View Figure 1
Figure 1: A) Preoperative coronary angiography showed the anomalous origin of the right coronary artery arising from the pulmonary artery and collateralization between the left coronary artery and the right coronary artery; B) Postoperative coronary angiography showed the anomalous origin of the right coronary artery arising from the pulmonary artery.
View Figure 1
Video 1: A) Movie of preoperative coronary angiography showing the anomalous origin of the right coronary artery from the pulmonary artery and collateralization between the left coronary artery and the right coronary artery; B) Postoperative coronary angiography showing reimplantation of the right coronary artery into the aorta for re-establishment of the physiological coronary system; C) Postoperative coronary angiography showing the left coronary artery.
Video 2: The orifices of left and right coronary artery were demonstrated the postoperative by transthoracic echocardiography. Color Doppler A) and spectral pulse-wave Doppler; B) showed Ostia of the right coronary artery, while Color Doppler; C) and spectral pulse-wave Doppler; D) showed Ostia of left coronary artery.
On the sixth day of admission, the patient was scheduled for mitral and aortic valve replacement as well as RCA re-implantation into the aorta. Once median sternotomy was performed, the ventricles were found to be considerably dilated, especially the left ventricle; and coronary arteries were also found to be substantially enlarged with abundant collateral circulation. In addition, the RCA was seen originating from the PA. After cross-clamping, cardiac arrest was achieved by the antegrade perfusion of cold cardioplegia via LCA. The superior and inferior vena cava was then clamped, and the PA was opened for administration of cardioplegia to the orifice of the anomalous RCA.
After exploring the valves and debriding the diseased valves, we sized the annulus using a valve sizer and fixed the two valves with suitable mechanical valves (aortic valve, ON-X Valves ONXAC 19 mm; mitral valve, ON-X Valves ONXAM 25 mm).
Then, the coronary artery system was rebuilt. The RCA ostium was separated from the PA along with the arterial wall, and the coronary button was carefully sutured using 6-0 Prolene to the incision in the aorta, where a hole with a diameter of 10.0 mm was made to avoid twisting or kinking. After completion of the aortic closure, we administered a cardioplegic solution to ensure adequate filling of the coronary artery. We then anastomosed the proximal PA to the distal PA and repaired the defect using a patch of autologous pericardium. Spontaneous return of heartbeat was achieved, and transesophageal echocardiography showed good blood flow of RCA and function of the two valves.
A follow-up echocardiogram revealed that the mechanical valves worked efficiently (Figure 2), and coronary angiography demonstrated normal blood flow in the RCA and LCA (Figure 1B). After an uneventful postoperative course, the patient was discharged on the 16 th day of admission and remained asymptomatic during the follow-up period of 10 years.
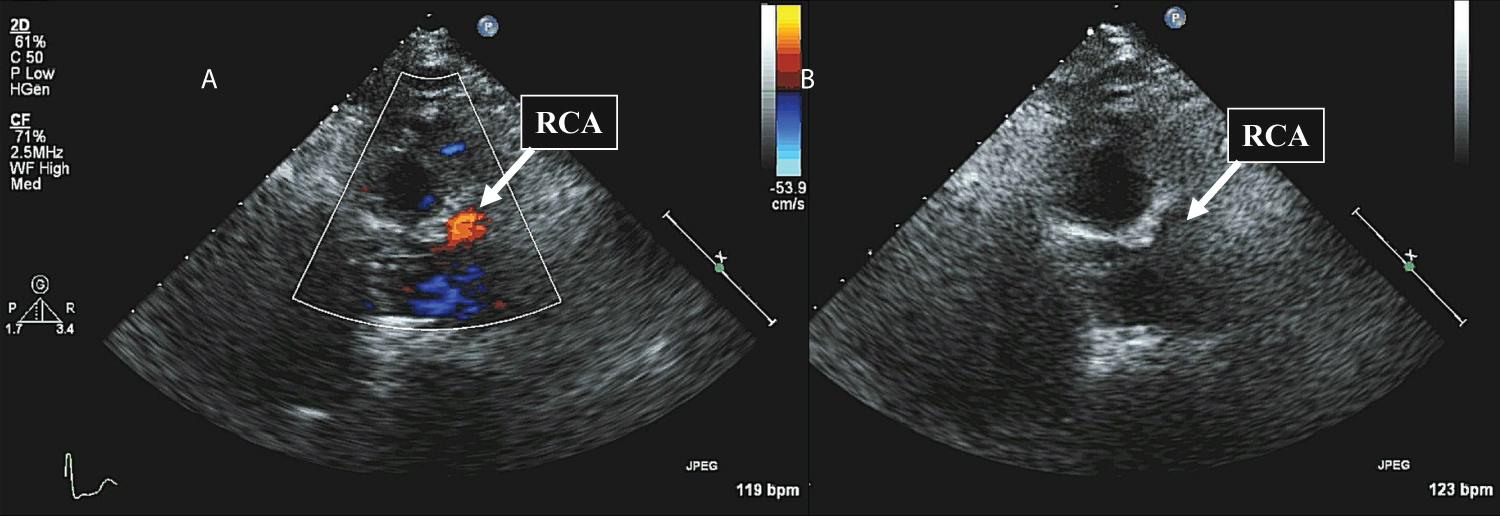 Figure 2: Transthoracic echocardiography showed the postoperative coronary artery. Color Doppler (A) and spectral pulse-wave Doppler (B) showed Ostia of right coronary artery.
View Figure 2
Figure 2: Transthoracic echocardiography showed the postoperative coronary artery. Color Doppler (A) and spectral pulse-wave Doppler (B) showed Ostia of right coronary artery.
View Figure 2
Origination of a coronary artery from the PA is one of the four described coronary artery anomalies [1]: 1) The anomalous origin of the LCA from the PA (ALCAPA), 2) ARCAPA, 3) The anomalous origin of both coronary arteries from the PA, and 4) Anomalous origin of an “accessory” artery from the PA. Although all of the exact mechanisms have yet to be elucidated, these abnormalities are widely believed to be failures of normal embryological development (4). Mal-positioning of coronary buds or malrotation of the spiral septum can lead to abnormal development of the coronary arteries [2]. Compared to ALCAPA, the most common type of coronary artery from the PA with an incidence of 0.008%, ARCAPA is a rare condition with a reported incidence of 0.002% in patients undergoing coronary angiography [1].
Since John Brooks reported the first case of ARCAPA in 1885 [3], over 100 cases of ARCAPA have been reported with varied clinical presentations. The clinical symptoms of ARCAPA are largely determined by the presence or absence of collaterals from the RCA to the LCA. If patients have enough collateral, they have sufficient perfusion of the coronary system, therefore, symptoms are absent. Approximately 38% of individuals with ARCAPA have been found to be asymptomatic before examination [3]. On the other hand, if collaterals are not sufficiently developed, patients may present with symptoms of myocardial ischemia and ventricular dysfunction, including chest pain, dyspnea, congestive heart failure, myocardial infarction, and even sudden death [4]. In those symptomatic patients, Guenther, et al. described a bimodal distribution of the age at presentation, some early after birth and some between 40 and 60 years [1]. Early in life, high pulmonary pressure causes antegrade flow of deoxygenated blood through RCA territory, leading to the formation of collateral vessels. As pulmonary pressure decreases, oxygenated blood flows retrograde into the PA via these collateral vessels, referred to as “coronary steal” [1]. If this phenomenon occurs, symptoms of ischemia in the RCA territory appear in the early years. However, some patients with ARCAPA are generally asymptomatic during their childhood and do not show ischemic symptoms until they are 40-60 years of age. These changes are likely related to atherosclerotic changes to the patient’s single coronary artery system [1].
In the past, coronary artery anomalies were diagnosed during surgery or at autopsy; however, coronary angiography is currently regarded as the gold standard for diagnosing ARCAPA [5]. Although invasive, it provides clear visualization of retrograde flow through the coronary artery, extensive collaterals between the LCA and RCA, increased flow with a dilated coronary system, and direct flow between the coronary and pulmonary arteries [6]. The use of echocardiography in diagnosing ARCAPA has recently been popularized due to the improved technology and non-invasiveness of the procedure. Features suggestive of ARCAPA on echocardiography include evidence of collateralization, dilation of coronary arteries, increased flow in the LCA, and flow between the RCA and the PA [1]. In our case, transthoracic echocardiography was used to evaluate the postoperative condition of the coronary artery and the valves. Computed tomography angiography and magnetic resonance angiography (MRA) can provide a three-dimensional representation of cardiac anatomy, which can help confirm the suspected diagnoses of echocardiography. MRA has the advantage of determining blood flow direction and velocity as well as not requiring ionizing radiation or intravenous contrast [7]. However, these two methods are very expensive and are not commonly used in practice.
Surgical treatment is strongly recommended as soon as the diagnosis is confirmed to prevent further complications. There are two purposes in the surgical treatment of ARCAPA, the elimination of left to right “coronary steal” and the establishment of dual coronary circulation from the aorta. Three surgical strategies have been applied clinically: Simple RCA ligation, RCA ligation with coronary artery bypass graft (CABG), and RCA re-implantation into the aorta. RCA re-implantation into the aorta is the most commonly performed procedure in the treatment of ARCAPA to establish a dual coronary artery system, which was applied in our study. During the surgery, the surgeon should pay more attention to avoid kinking of the re-implanted vessel. For our patient, a good result was obtained after rebuilding the coronary artery system. In addition, coronary angiography and echocardiography also showed good recovery. Another surgical technique for establishing a dual coronary artery system is CABG. However, compared to RCA re-implantation, CABG decreases the patency rate [1]. Currently, CABG is mainly selected when ARCAPA originates from the posterior wall of the PA, and re-implantation cannot be performed. Previously, simple RCA ligation was the main surgical method of ARCAPA, but it also put the patient at serious risk if blood flow from the LCA becomes compromised [1]. Nevertheless, simple RCA ligation is also used for some patients who are not deemed good surgical candidates for cardiopulmonary bypass.
In summary, we present the case of a patient with multivalve heart disease who was diagnosed with ARCAPA through coronary angiography and treated with RCA re-implantation into the aorta. ARCAPA is a rare coronary anomaly, most commonly diagnosed using coronary angiography. Once the diagnosis is confirmed, surgery is strongly recommended to minimize the risk of death.
Written informed consent has been obtained from the patient to publish this paper.
The data that support the findings of this study are available on request from the corresponding author.
The authors declare no conflict of interest.
This research received no external funding.
Conceptualization: LG and OC; Methodology: LG and WW; Software: LG and QM; Validation: LG and FC; Formal analysis: LG and OC; Investigation: LG and HQ; Resources: XJ, XL, and QM; Data curation: XJ; Writing-original draft preparation: LG; Writing-review and editing: LG, OC, WW, FC, HQ, QM, XL, and XJ; Visualization, LG; Supervision: XJ; Project administration: XJ. All authors have read and agreed to the published version of the manuscript.