A 57-year-old male with history of head and neck squamous cell carcinoma (HNSCC), in remission, presented with face and neck swelling and dyspnea. He was found to have recurrence of his HNSCC at the base of his tongue and a new right ventricular mass. Two endomyocardial biopsy attempts yielded benign tissue. A trans-jugular core needle biopsy performed, under fluoroscopy and intracardiac echocardiogram (ICE) guidance, revealed metastasis of primary tumor. To our knowledge, this is the first case reported in the literature of a core needle biopsy approach for diagnosis of a cardiac mass.
Squamous cell carcinoma, Cardiac mass, Metastasis, Trans-jugular, Core needle biopsy
Cardiac metastasis is a rare sequela of head and neck squamous cell carcinoma (HNSCC) with only a few cases reported in the literature. Conversely, intracardiac masses are most commonly metastases and rarely angiosarcomas, or benign tissue [1]. Imaging modalities such as cardiac MRI, CT, and PET scans have been essential for lesion characterization [1]. However, endomyocardial biopsy (EMB) via transfemoral approach is often used for definitive diagnosis to guide treatment. We present a case of a 57-year-old male with recurrent HNSCC and newly noted right ventricular mass in which his cardiac mass access was technically challenging. This has led to employment of trans-jugular core needle biopsy- an approach more commonly utilized for liver masses biopsies.
The objectives of this report are to understand the role of multimodality imaging and interdisciplinary approach in the diagnosis of cardiac tumors and to introduce a potential use of trans-jugular core-needle biopsy for cardiac mass sampling.
A 57-year-old male with a history of oropharyngeal squamous cell carcinoma treated with radiation and seven rounds of cetuximab, subsequently in remission, presented with dyspnea along with face and neck swelling. On physical exam, vital signs were within normal limits. Head and neck exam notable for swelling and firmness bilaterally and right L2 lymphadenopathy. Cardiopulmonary exam was unremarkable. Complete blood count showed normal cell line counts and metabolic panel was at baseline. CT head and neck showed large mass at base of tongue consistent with reoccurrence of malignancy. CT Imaging also revealed a moderate-to-large pericardial effusion and a mass along the epicardium (Figure 1A). Echocardiogram showed a large pericardial effusion and a right ventricular (RV) mass (Figure 2). For further characterization of current presentation, patient underwent a Lymph node biopsy which was consistent with PDL-1 positive metastatic HNSCC.
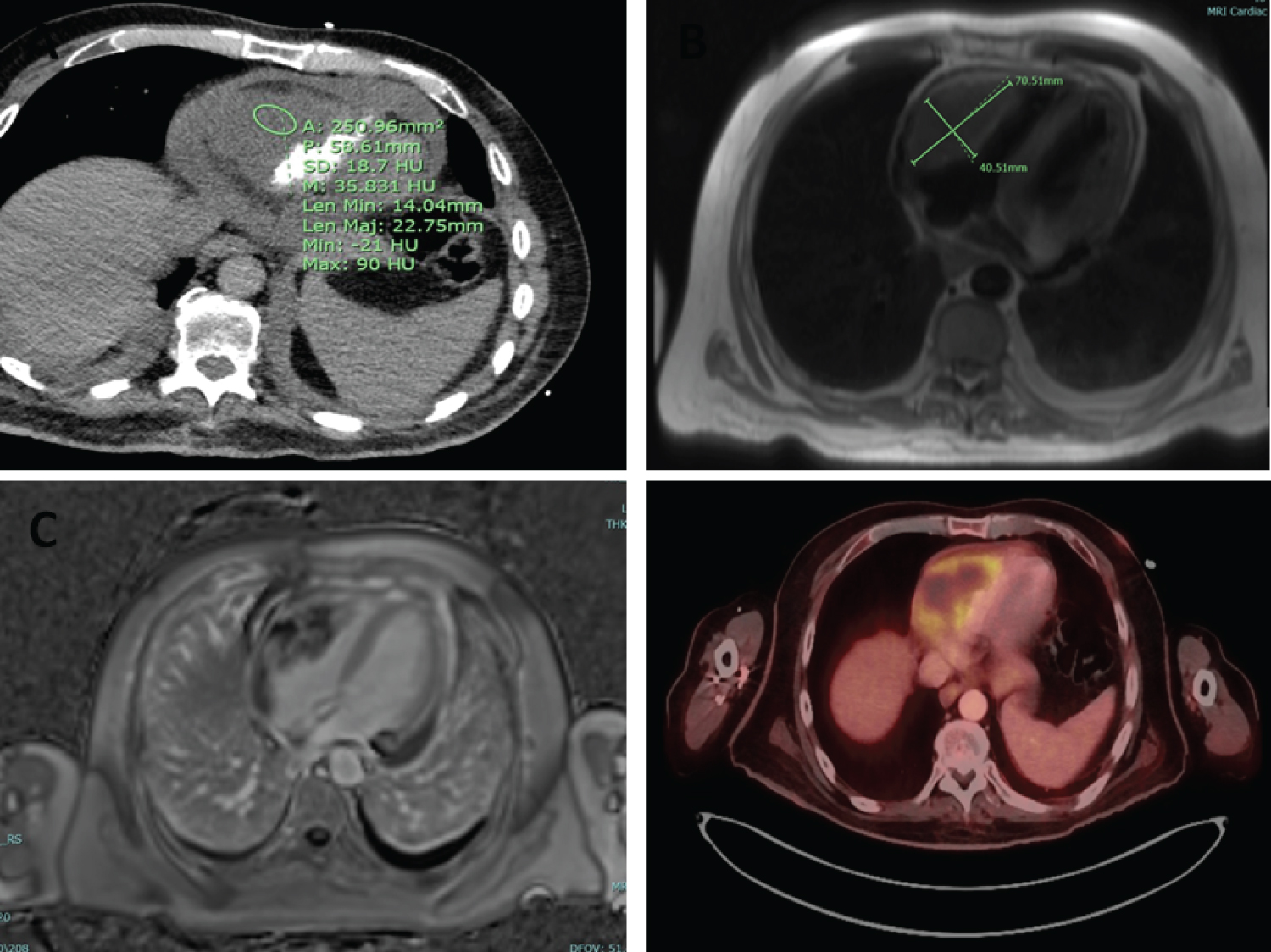 Figure 1: A) CT scan showing moderate to large pericardial effusion and a lobular hypodense mass along the visceral pericardium/ epicardium of right heart border; B) T2 weighted cardiac MRI image showing a ~7.1 × 4.1 cm mass arising from the wall of the RV and extending into the RV outflow tract; C) MRI image of RV mass showing delayed enhancement; D) PET Scan showing 8.7 × 4.7 × 6.8 cm hypermetabolic mass involving the right ventricle with mass effect on the ventricular ligament.
View Figure 1
Figure 1: A) CT scan showing moderate to large pericardial effusion and a lobular hypodense mass along the visceral pericardium/ epicardium of right heart border; B) T2 weighted cardiac MRI image showing a ~7.1 × 4.1 cm mass arising from the wall of the RV and extending into the RV outflow tract; C) MRI image of RV mass showing delayed enhancement; D) PET Scan showing 8.7 × 4.7 × 6.8 cm hypermetabolic mass involving the right ventricle with mass effect on the ventricular ligament.
View Figure 1
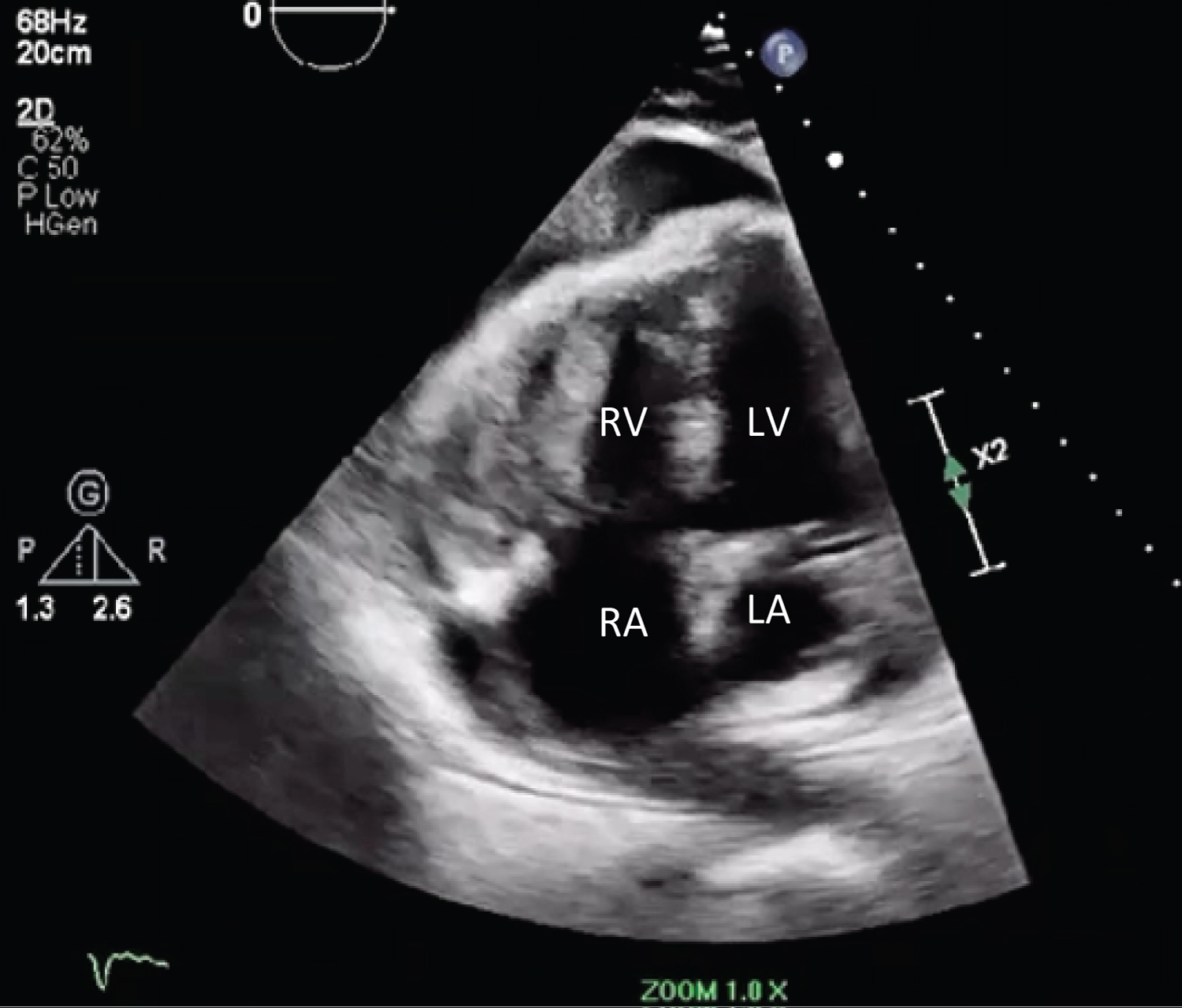 Figure 2: Apical four chamber view showing RV mass.
View Figure 2
Figure 2: Apical four chamber view showing RV mass.
View Figure 2
Initial consideration for the cardiac mass was potential metastasis of his primary tumor -SCC. However, given the rarity of the spread of SCC to the heart, alternative differential diagnoses of angiosarcoma, melanoma, or RV thrombus were considered.
A pericardiocentesis was attempted for pericardial fluid analysis, however, was unsuccessful due to small fluid accumulation. Subsequent echocardiogram showed resolution of the pericardial effusion. A Cardiac MRI confirmed the presence of a vascular RV mass with peripheral delayed enhancement (Figure 1B and Figure 1C). An endomyocardial biopsy using standard myocardial bioptome via transfemoral approach was attempted but yielded benign fibrinous endomyocardial tissue likely due to the epicardial location of the tumor. The cardiothoracic surgery team evaluated images and relayed that to obtain a meaningful tissue sample, the patient would have to be put on cardiopulmonary bypass, a high-risk procedure in the setting of his already advanced cancer. Chemotherapy options depended on whether the cardiac mass was primary versus secondary malignancy. Another endomyocardial biopsy was pursued, this time using ICE guidance, again yielding benign tissue. The Oncology team communicated that if the pathology was yielding benign tissue, they had to suspect the patient may have a new primary angiosarcoma and would not qualify for further chemotherapy.
At one final attempt, a trans-jugular approach using a 19-guage core needle was advanced 3-cm into the myocardium from the RV cavity, by interventional radiology under fluoroscopy and ICE guidance, obtaining tissue biopsy. This yielded the diagnosis of squamous cell carcinoma (Figure 3), suggesting metastasis of primary cancer. Oncology team started patient on cycle 1 of Carboplatin, paclitaxel, and Pembrolizumab regimen with plans for close monitoring of RV mass as patient continues current treatment plan. Improvement in symptoms was initially noted on patient’s follow-up visit. However, patient relapsed and passed away a few months later.
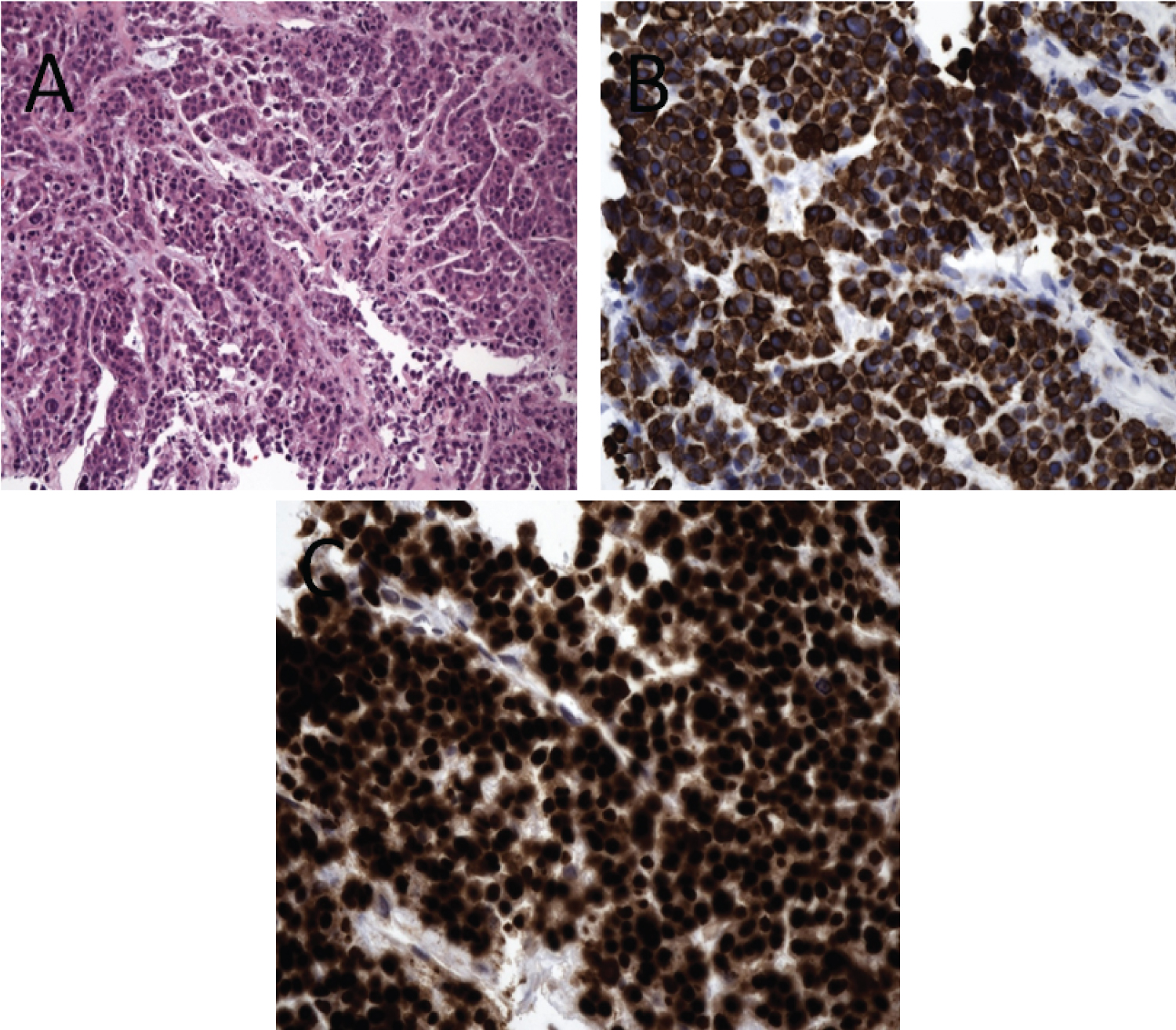 Figure 3: A) Nests and cords of pleomorphic malignant cells with round to oval nuclei and abundant eosinophilic cytoplasm (Hematoxylin and Eosin on FFPE section); B) Tumor cells show positive nuclear staining for P63 (P63 IHC on FFPE section) and strong diffuse cytoplasmic staining with nuclear enhancement for Cytokeratin 5/6; C) (CK5/6 IHC on FFPE section), compatible with metastatic squamous cell carcinoma.
View Figure 3
Figure 3: A) Nests and cords of pleomorphic malignant cells with round to oval nuclei and abundant eosinophilic cytoplasm (Hematoxylin and Eosin on FFPE section); B) Tumor cells show positive nuclear staining for P63 (P63 IHC on FFPE section) and strong diffuse cytoplasmic staining with nuclear enhancement for Cytokeratin 5/6; C) (CK5/6 IHC on FFPE section), compatible with metastatic squamous cell carcinoma.
View Figure 3
In our case, the patient's oncologic treatment plan was contingent on tumor characterization. If cardiac mass is determined to be HNSCC, the tumors are usually responsive to targeted treatments. Initial diagnostic efforts with cytological evaluation of pericardial effusion via pericardiocentesis and transfemoral EMB have failed to yield diagnostic information. Therefore, further evaluation with advanced imaging was pursued with CMR for further tumor characterization and anatomical evolution which revealed a highly vascular lesion. Given the vascularity on cardiac MRI and the benign tissue from EMB, the team was concerned for new primary angiosarcoma. Given, the unclear etiology of the tumor, a multidisciplinary approach was taken involving interventional radiology and cardiothoracic surgical team. Ultimately, a more targeted but rare approach for cardiac biopsy with trans-jugular core needle under fluoroscopy and ICE guidance was performed.
Cardiac tumors are a rare entity presenting a challenge with diagnosis; therefore tissue confirmation is essential [1]. Multimodality imaging has been employed as a means for further structural characterizations and etiology identification. Transthoracic Echocardiography has been the first line imaging modality for preliminary hemodynamic and structural evaluation of cardiac masses; however, it poses the limitation of evaluation of mass origin and extent [2]. Follow-up evaluation with TEE can provide further insight into mass characteristics. Use of ultrasound enhancing agents provides information regarding mass vascularity which can be different with different pathologies [3]. Cardiac MR can provide morphological information along with histopathologic characteristics such as tissue infiltration, calcification, hemorrhage, vascularity, etc. [1,4,5] while PET can aid in staging and optimization of biopsy location [5]. Although imaging can provide valuable information, histopathologic evaluation remains to be the gold standard for confirmation.
Endomyocardial biopsies are conventionally undertaken via the transfemoral route. A few case reports have discussed the use of alternative techniques for tissue sampling such as CT [6] and percutaneous ultrasound (PUS) [7] guided core needle biopsies of cardiac tissue; however, there had been no prior mention of ICE guided, trans-jugular core needle biopsy in the diagnosis of HNSCC cardiac metastasis. Trans-jugular biopsy approach is commonly used for liver tissue sampling during which a small sheath is introduced into the right internal jugular vein to access the hepatic vein [8]. Additionally, it was also introduced for kidney biopsy in 1989 after the accidental discovery by Mal F, et al. while intending to perform a trans-jugular liver biopsy [9]. Since then, it had been used alongside percutaneous approaches. However, trans-jugular cardiac core needle biopsy has yet to become a potentially utilized procedure. Based on our case, we believe that trans-jugular cardiac core needle biopsy can be utilized as an alternative approach in cases where the cardiac mass location poses difficulty in obtaining tissue using standard current methods.
Cardiac tumor evaluation and characterization is critical for management and prognosis. Often, tumor sampling can be challenging requiring an interdisciplinary approach involving interventional cardiology and interventional radiology to obtain a direct biopsy of the mass using alternative techniques and approaches.
BG, MS, RB, SM wrote the manuscript and reviewed the literature. SC critically revised the manuscript for important intellectual content, supervised the process and approved the final draft.
The authors have no funding for this research from any funding agency in the public, commercial or not-for-profit sectors to disclose.
None declared.
Informed consent was obtained from the patient’s next of kin for publication of this case report, including accompanying images.