Background: Fractional flow reserve (FFR)-guided percutaneous coronary intervention (PCI) has shown better clinical outcomes than conventional angiography-guided PCI. The optimal FFR cut-off value for revascularization is debated. With FFR ≤ 0.75, revascularization for coronary artery disease (CAD) stenosis is associated with improved clinical outcomes, whereas with FFR ≥ 0.8, medical treatment has been shown to result in favorable long-term outcomes. However, there has been controversy over revascularization decision-making for coronary stenosis with FFR between 0.75 and 0.80, the so-called grey zone.
Objectives: The present study aims to compare intermediate-term outcomes of performed versus deferred Percutaneous Coronary Intervention in moderate coronary stenosis with FFR values in the grey zone (0.75-0.80) and the primary outcome will be six months major adverse cardiac event (MACE).
Methods: A non-randomized prospective clinical study was conducted over 3 years period between January 2019 and January 2022. The study included stable CAD patients with coronary lesions between 40-70% diameter stenosis who underwent FFR study using intracoronary (IC) adenosine and had FFR values between 0.75-0.80 and were divided into two groups: group 1 who have undergone revascularization and group 2 who have undergone deferred revascularization.
Results: This study was conducted on 50 patients with moderate coronary artery stenosis with an FFR value in the grey zone undergoing performed or deferred revascularization. The age of the studied group ranged from 38-67 (mean 53.16 ± 7.83) years. The studied group included 12 females (24%) and 38 males (76%). 72% of the patients have diabetes, 70% hypertension, 94% dyslipidaemia and 52% were smokers. There was no significant difference between patients undergoing performed or deferred PCI as regard the risk factors (p-value 0.697).
The most common culprit vessel is the left anterior descending (LAD) (64%) followed by right coronary artery (RCA) (20%) then left circumflex (LCX) (16%). 54% of the patients have undergone performed PCI while 46% have undergone deferred PCI with LAD (33.3% and 26.0%) followed by RCA (8.6% and 11.4%) then LCX (7.4% and 8.6%) respectively. There was no significant difference between patients undergoing performed or deferred PCI in regard to either the value of FFR or Culprit vessel (p-value 0.157, 0.232). 87.7% of the patients were asymptomatic after six months, stable and had no MACE. Six patients were symptomatic with MACE 6 patients had target vessel revascularization (TVR) (2 in group 1 and 4 in group 2) with 3 myocardial infarction (MI) (1 post-procedure in group 1 and 2 spontaneous in group 2) and one patient died after 3 months (group 1).
No significant difference was found between patients undergoing performed or deferred PCI in regard either the clinical status, presentation & target coronary intervention, or MACE after three months (p-value 0.363) as well as after six months follow up (p-value 0.469).
Conclusions: Our study found that after 6 months follow-up period in patients with angiographically borderline coronary lesion with grey-zone FFR (0.75-0.8), either performing or deferring coronary intervention are effective and safe.
Coronary artery disease, Fraction flow reserve, Grey-zone, Coronary intervention
Coronary Artery Disease (CAD), the most important entity of Heart disease; occurs when atherosclerotic plaque builds up within walls of the coronary arteries leading to narrowing and appearance of the clinical manifestations of Acute Coronary Syndrome (ACS) that include angina and Myocardial Infarction (MI) [1]. Symptoms of CAD require ongoing monitoring and treatment to prevent further complications as MI and Heart Failure (HF) [2].
The overall rate of CVD deaths in low and middle-income countries collectively is 28% as compared to 58% in Eastern Europe and 10% in Sub Saharan Africa [3]. In Egypt, the National Hypertension Project (NHP) found an adjusted overall prevalence of CAD is 8.3% and was responsible for 32.4% of the deaths [4].
Coronary physiology is the collective term for a group of indexes aimed at directly measuring the intracoronary haemodynamic changes that occur across a stenosis in order to guide revascularization decision-making [5].
Fractional flow reserve (FFR) uses pharmacological dilatation and miniaturized pressure-wires to measure coronary pressure proximal and distal to a stenosis, thereby estimating flow reduction across a stenosis [6].
Several clinical trials have shown that FFR-guided revascularization improves clinical outcomes, and that deferring revascularization in patients shown by FFR to have non-hemodynamically significant lesions is safe [7-9].
Myocardial ischemia is a flow-based pathology. However, performing measurements of intracoronary flow is technically difficult and is, thus, largely confined to research settings. Attention has, therefore, turned to measuring intracoronary pressure (which is technically much simpler to measure), as a clinically applicable surrogate measure of flow. The basic principle of FFR is to eliminate the resistance of the microcirculation using pharmacological dilatation. This is termed maximal hyperaemia. Analogous to Ohm’s law (V = IR, where V is voltage difference, I is current and R is resistance), it can be assumed that when coronary resistance is stable and minimal (as occurs during maximal hyperemia), a direct relationship exists between coronary pressure and flow. As such, in the context of hyperemia, coronary pressure measurements can be used to assess the functional impact of a stenosis on the myocardium [10].
FFR was introduced as a means of determining coronary flow using pressure-only-based assessments during hyperemia. FFR is defined as the ratio of the pressure distal to a stenosis (Pd) relative to the pressure proximal to the stenosis (Pa) during maximal hyperemia. As such, a FFR value of 0.80 represents a pressure loss across the stenosis of 20% [11].
FFR expresses the maximum achievable blood flow to the myocardium supplied by a stenotic artery as a fraction of normal maximum flow. As such, it provides an objective measure of the haemodynamic significance of an epicardial stenosis. It can be measured during coronary angiography by passing a specialized guidewire with a specific solid-state sensor at its tip into the coronary vasculature. Once the sensor is advanced distal to the epicardial lesion in question, a pressure reading can be obtained from downstream to the lesion (Pd). A simultaneous pressure reading can be obtained from the tip of the guide catheter, which represents the pressure proximal to the lesion (Pa). By dividing the former by the latter, a ratio of pressures is obtained (Pd/Pa). It has been shown that a ratio of flows can be derived from this, provided that the pressures are measured during maximal hyperemia when resistance is at its lowest. Therefore, one of the most crucial steps in the assessment of FFR is appropriate use of pharmacological hyperemic stimuli. In order to achieve maximal hyperemia, vasodilatation of the epicardial and the microvascular circulation is necessary; a bolus of intracoronary nitrate and an intravenous infusion of adenosine respectively are the most commonly used measures [12].
Instantaneous wave-free ratio (iFR) is a novel technique that measures the ratio of distal coronary to aortic pressure during a specific period in diastole that obviates the need for pharmacological vasodilation and shown to be non-inferior to FFR with respect to major adverse cardiac events, while reducing adverse procedural symptoms and procedure duration [13].
Fractional flow reserve (FFR)-guided percutaneous coronary intervention (PCI) has shown better clinical outcomes than conventional angiography-guided PCI [7-9].
The optimal FFR cut-off value for revascularization is debated. With FFR ≤ 0.80, revascularization for coronary stenosis is associated with improved clinical outcomes, whereas with FFR ≥ 0.75, medical treatment has been shown to result in favorable long-term outcomes [9].
However, there has been controversy over revascularization decision-making for coronary stenosis with FFR between 0.75 and 0.80, the so-called grey zone. Several studies have reported the outcomes of revascularization vs. deferral for coronary stenosis with grey-zone FFR values, with conflicting results [14-18]. However, these studies were hampered by limited numbers of patients and short follow-up periods.
Therefore, in this study, we compared the intermediate-term (six months) outcomes of patients undergoing deferral versus performed percutaneous coronary intervention for coronary stenosis with grey zone FFR (0.75-0.80) values included in a prospective non-randomized clinical trial.
This study aimed to compare intermediate-term outcomes of patients performed versus deferred Percutaneous Coronary Intervention in coronary stenosis with FFR values in the grey zone (0.75-0.80) and the primary outcome will be a major adverse cardiac event.
To assess effectiveness of performed Percutaneous Coronary Intervention for coronary stenosis with grey-zone fractional flow reserve values.
To assess effectiveness of deferred Percutaneous Coronary Intervention for coronary stenosis with grey-zone fractional flow reserve values.
To compare between effectiveness of deferred vs. performed Percutaneous Coronary Intervention for coronary stenosis with grey-zone fractional flow reserve values.
A non-randomized prospective clinical study was conducted between the period from January 2019 and January 2022.
Stable CAD patients with coronary lesions between 40-70% diameter stenosis who underwent FFR study using IC adenosine and had FFR values between 0.75-0.80 and was divided into two groups:
1. Coronary artery stenosis patients who have undergone evascularization.
2. Coronary artery stenosis patients undergoing deferred revascularization.
Exclusion criteria:
• Patients suffering from ACS.
• Patients with contraindications to IC adenosine.
• A graft vessel.
• Overt heart failure.
• A stenosis technically unsuitable for FFR evaluation.
Sample size was calculated according to the following formula [19].
Where:
n = sample size
Z α/2 = 1.96 (The critical value that divides the central 95% of the Z distribution from the 5% in the tail)
Z β = 0.84 (The critical value that separates the lower 20% of the Z distribution from the upper 80%)
P 1 = Target vessel revascularization (TVR) occurred in patients in the deferred group = 8.1%
P 2 = Target vessel revascularization (TVR) occurred in patients in the performed group = 8.4%
q = 1-P
Based on the previous calculations, and after accounting for a 10% drop-out rate, the required number of participants was 50 patients.
For this sub study, all patients with a 40-70% de novo native coronary artery stenosis with an FFR value in the grey zone (0.75-0.80) were enrolled. To eliminate the clustering effects of lesions within the same patient, one lesion per patient was selected, preferentially choosing those with lower FFR values, or left anterior descending arterial lesions when the FFR values are equal for two or more lesions.
Fractional flow reserve measurement: Fractional flow reserve was measured after coronary angiography with a commercially available coronary pressure wire, as previously described [16]. After the administration of intracoronary adenosine (100 mcg for the RCA and 200 mcg for the LCA), the pressure wire was positioned in the distal segment of the target vessel.
The proximal aortic pressure (Pa) and distal (Pd) was measured during sustained hyperemia, and FFR was calculated as the mean value of Pd/Pa. For FFR values between 0.75 and 0.80, the decision regarding revascularization was at the operator’s discretion. All the revascularization procedures for PCI were performed using standard techniques [7].
Abbott’s generation of the PressureWire™ X Guidewire was used during this study. The innovative PressureWire™ X Guidewire-can measure pressure and temperature to calculate Abbott's Resting Full-Cycle Ratio (RFR), Fractional Flow Reserve (FFR), Index of Microvascular Resistance (IMR), and Coronary Flow Reserve (CFR). The guidewire’s fully integrated & secure.
Measurements are integral to a cardiac catheter lab’s clinical physiology routine. Additionally, second-generation drug-eluting stents were routinely used. Routine follow-up angiography after the index procedure was highly discouraged.
Quantitative coronary angiography: Quantitative coronary angiography was performed using standard techniques and automated edge-detection algorithms (CAAS-5, Pie Medical, Maastricht, Netherlands). Diameter stenosis, minimal lumen diameter, lesion length, and reference lumen diameter were measured [19]. The target lesions were coronary lesions between 40-70% diameter stenosis.
Outcomes and definitions: The primary outcomes were:
1. Cardiovascular death.
2. Myocardial infarction (either spontaneous or peri-procedural):
Periprocedural MI is defined as follows: within the first 48 h of the index revascularization procedure, ischemic symptoms and signs, with the cardiac troponin (cTn) elevation to more than five times of the 99 th percentile upper reference limit (URL) after the procedure that related to the FFR-measured vessels, accompanied by ischemic symptoms (Type 4a MI).
Spontaneous MI is defined as ischemia caused by primary coronary event associated with an elevation of the cardiac troponin above the upper reference limit (URL) with evidence of ischemia (Type I MI) [20].
3. Target vessel revascularization: which was defined as any percutaneous coronary intervention or bypass surgery of the index vessel?
The data was collected using a web-based dedicated case report form. Clinical follow-ups were conducted during hospitalization, 3 and 6 months after the index procedure. The patients’ clinical status, interventions, and adverse events were recorded at each visit.
• Baseline characteristics are presented as a number (%) for categorical variables and mean ± standard deviation for continuous variables.
• Differences between groups were analyzed using the student’s t-test or the Mann–Whitney U-test for continuous variables and the v2 test or the Fisher’s exact test for categorical variables, as appropriate.
• Additional adjustments were made with propensity score matching and weighted Cox proportional hazards regression models with inverse probability of treatment weighting (IPTW).
• The statistical analyses were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY, USA) and R version 3.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
• P-values < 0.05 were considered statistically significant.
The study protocol got approval from the research ethics committee of faculty of medicine Suez Canal University.
An informed written consent was taken from all patients or from their relatives before taking any data or doing any investigations.
This study was conducted on 50 patients with moderate coronary artery stenosis with an FFR value in the grey zone undergoing performed or deferred revascularization. The age of the studied group ranged from 38-67 (mean of 53.16 ± 7.83) years. The studied group included 12 females (24%) and 38 males (76%) (Table 1). Table 2 shows that the mean age of patients undergoing performed PCI is significantly higher than that of those who are undergoing deferred PCI (p-value 0.046). While there is no significant difference as regard gender (p-value 0.094). In regard to the risk factors, 72% of the patients have DM, 70% hypertension, 94% dyslipidemia and 52% among them are smokers (Table 1). There was no significant difference between patients undergoing performed or deferred PCI as regard the risk factors (p-value 0.697) (Table 3). 54% of the patients have undergone performed PCI while 46% have undergone deferred PCI (Table 4 and Figure 1). The most common culprit vessel is the left anterior descending (64%) followed by right coronary artery (20%) then left circumflex (16%) (Table 4 and Figure 2).
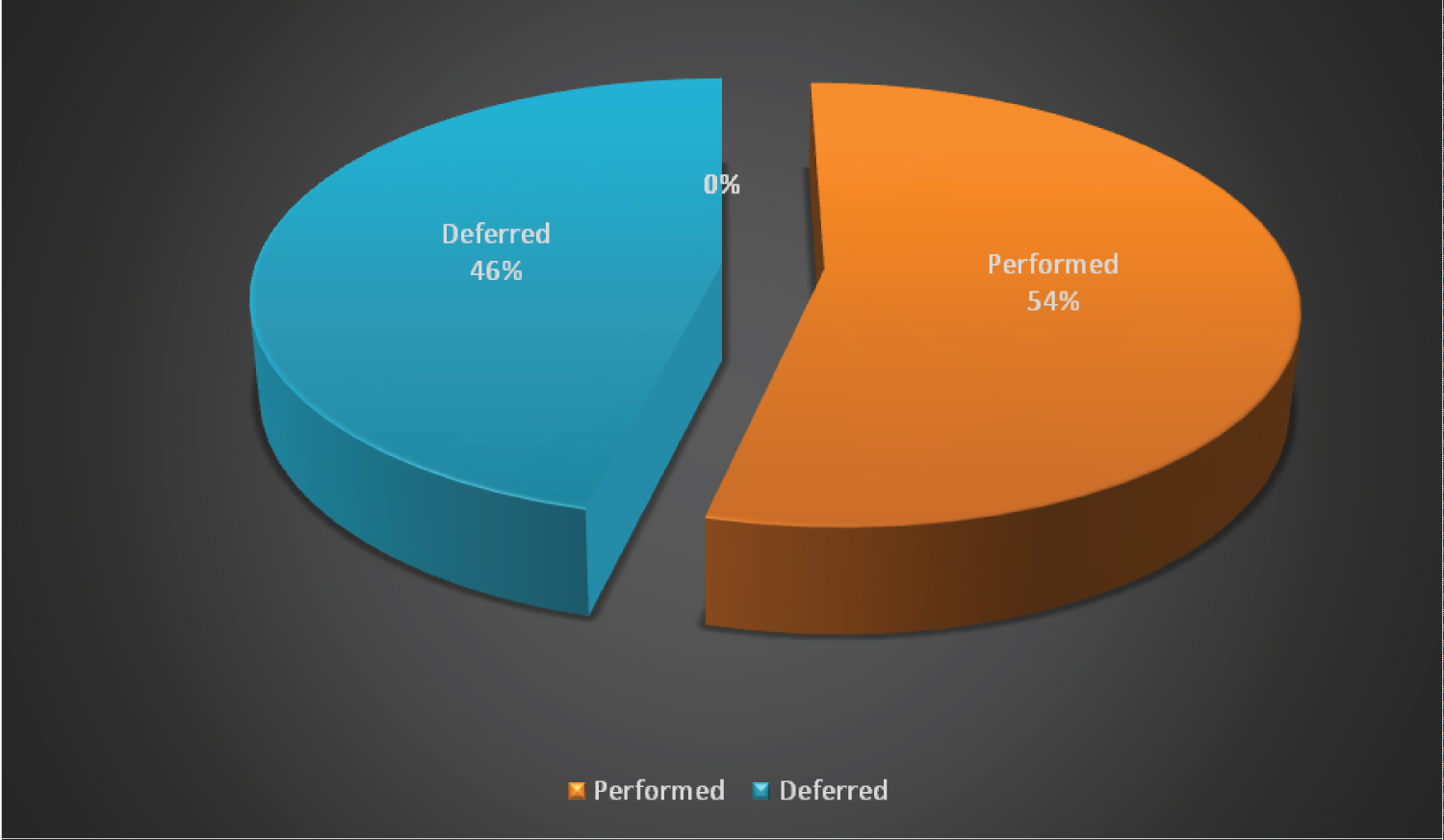 Figure 1: Pie chart displaying the type of PCI among the studied group (n = 50).
View Figure 1
Figure 1: Pie chart displaying the type of PCI among the studied group (n = 50).
View Figure 1
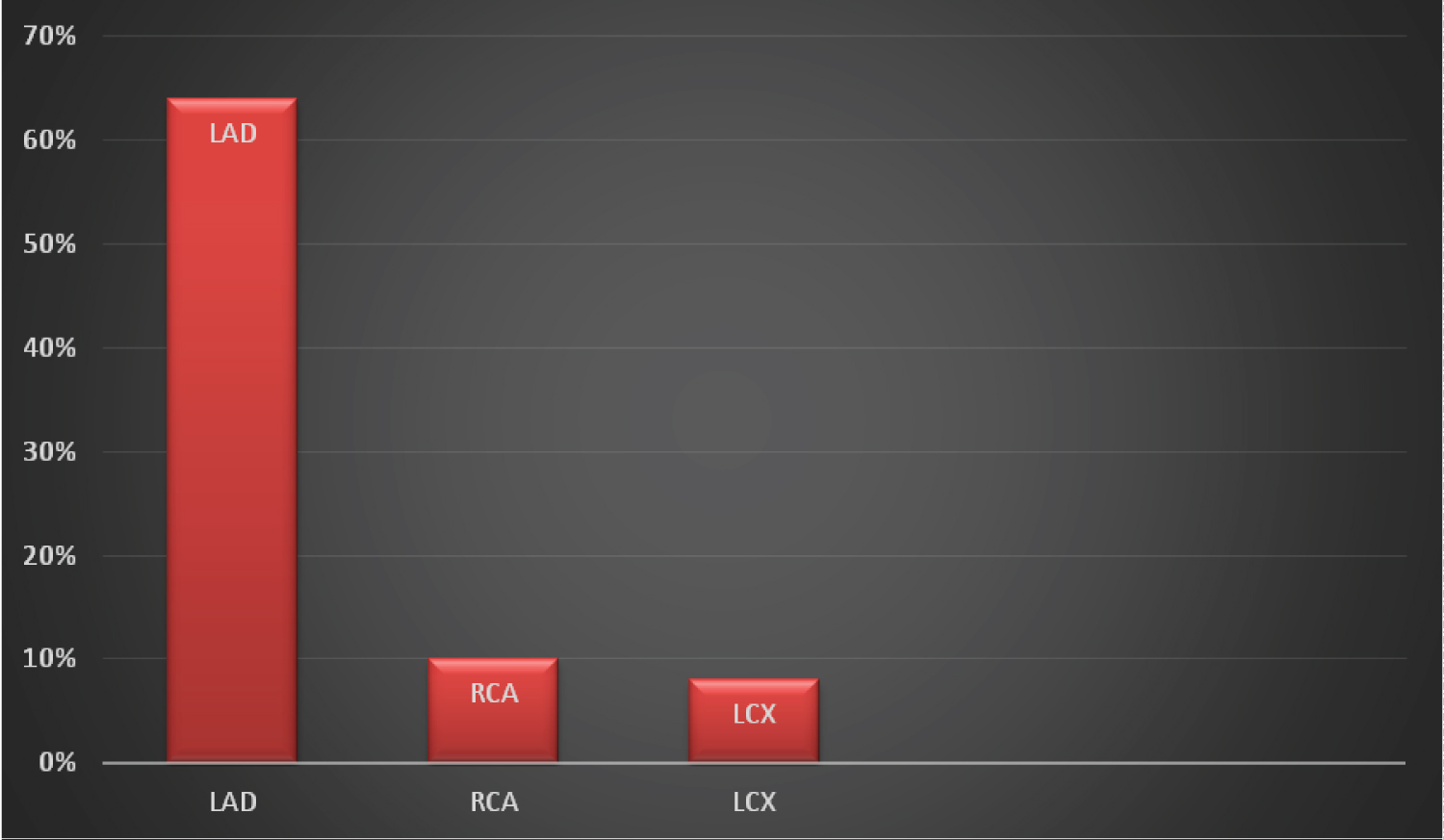 Figure 2: Bar chart displaying the culprit vessel among the studied group (n = 50).
View Figure 2
Figure 2: Bar chart displaying the culprit vessel among the studied group (n = 50).
View Figure 2
Table 1: Baseline demographic data. View Table 1
Table 2: Comparison between performed and deferred PCI demographic data. View Table 2
Table 3: Comparison of risk factors between performed and deferred PCI. View Table 3
Table 4: Angiographic data of the studied patients. View Table 4
There was no significant difference between patients undergoing performed or deferred PCI as regard either the value of FFR or the Culprit vessel (p-value 0.157, 0.232) (Table 5). The distribution of the patients in both groups based on the degree of culprit vessel stenosis at baseline assessment revealed that most of the patients in both groups had 70% stenosis in the LAD vessel (33.3% and 26.0% respectively), while 7.4% of patients in the performed group had RCA 70% stenosis and equal percentage of patients in the deferred group had RCA 70%, 50%, and 40% stenosis (8.6%). Finally, 7.4% of the patients in the performed group had 70% and 60% stenosis in the LCX vessel, compared to 8.6% in the deferred group. These differences were statistically insignificant (Table 6).
Table 5: Comparison between performed and deferred PCI as regard to target vessel. View Table 5
Table 6: Comparison between performed and deferred PCI as regard the basic angiographic stenosis data. View Table 6
One patient in the deferred group died after 3 months and so the total number of patients remaining was 49. 87.7% of the patients were asymptomatic after six months, stable and had no MACE. Six patients were symptomatic with TVR (Table 7 and Figure 3). Six patients had TVR, 3 patients had MI; 2 spontaneous and one patient had peri-procedural MI (Table 8).
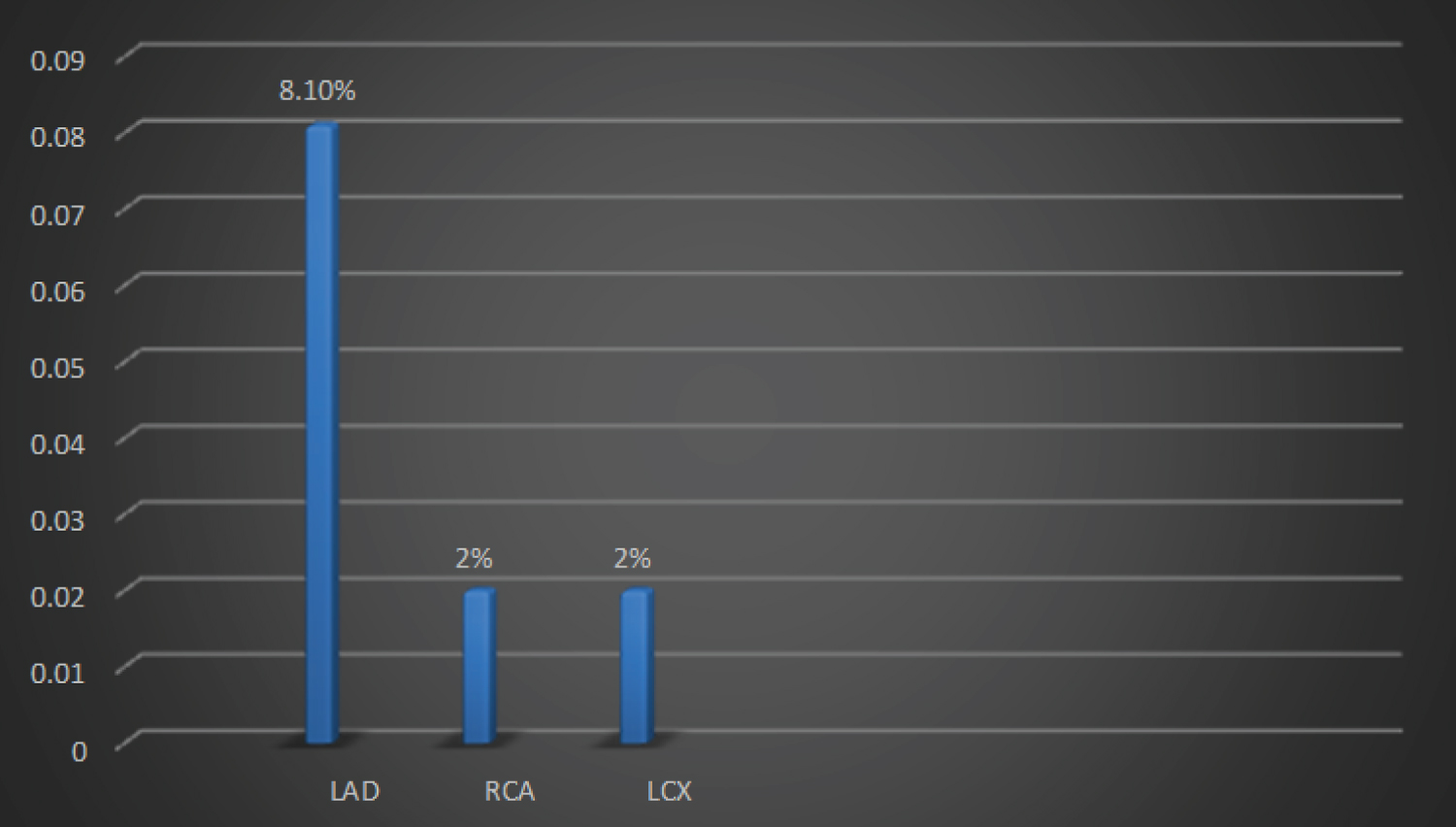 Figure 3: Bar chart displaying the Target vessel revascularization among the studied group.
View Figure 3
Figure 3: Bar chart displaying the Target vessel revascularization among the studied group.
View Figure 3
Table 7: Six months follow up clinical and TVR. View Table 7
Table 8: Six months Major adverse cardiac events (MACE). View Table 8
There was no significant difference between patients undergoing performed or deferred PCI in regard to either the clinical status or coronary intervention after six months follow up duration (p-value 0.469, 0.622) (Table 9 and Figure 4). Finally, there was no significant difference between patients undergoing performed or deferred PCI in regard to MACE after six months follow up duration (p-value 0.488) (Table 10 and Figure 5).
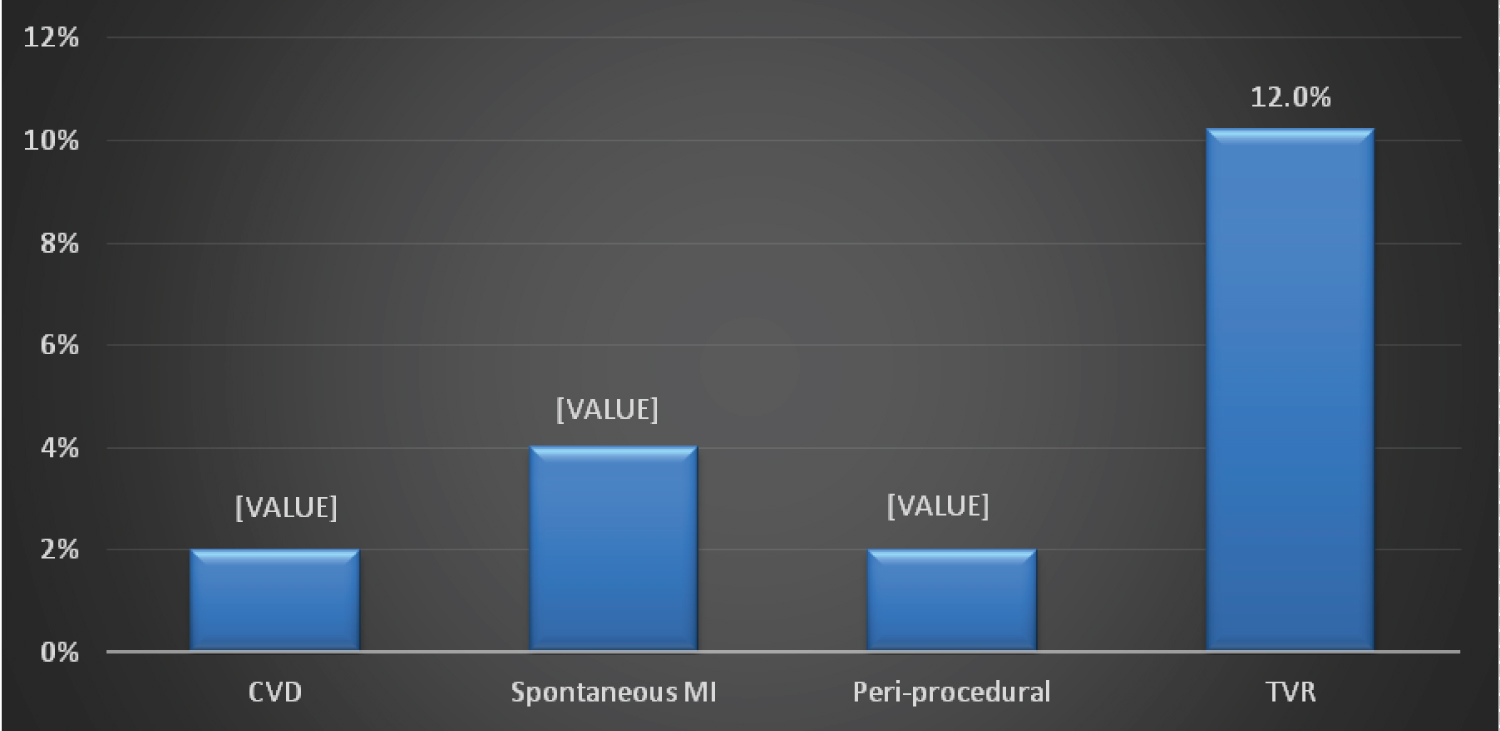 Figure 4: Bar chart displaying the MACE after 6 months follow up.
View Figure 4
Figure 4: Bar chart displaying the MACE after 6 months follow up.
View Figure 4
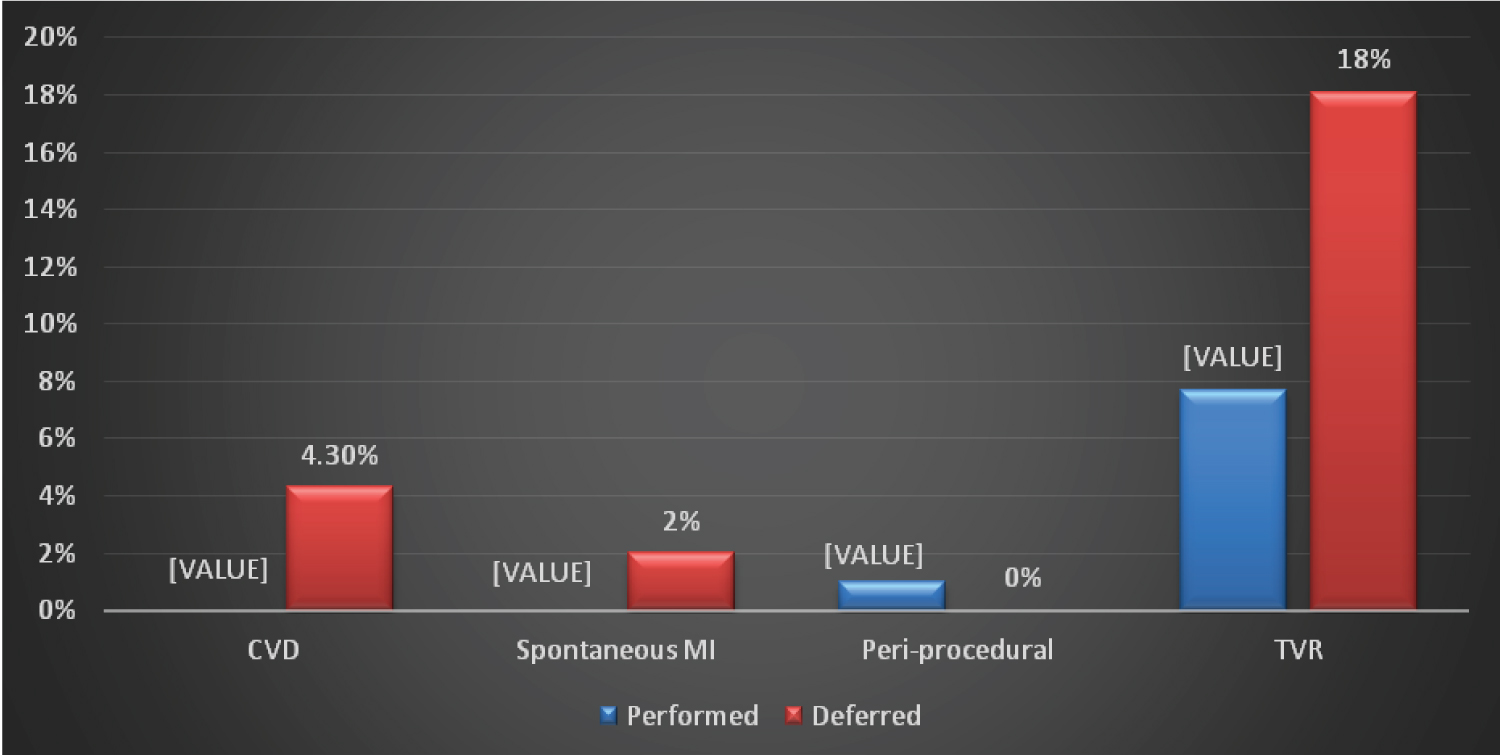 Figure 5: Bar chart displaying the MACE among the studied group after 6 months follow-up.
View Figure 5
Figure 5: Bar chart displaying the MACE among the studied group after 6 months follow-up.
View Figure 5
Table 9: Six months follow up clinical and TVR between performed and deferred PCI groups. View Table 9
Table 10: Six months Major adverse cardiac events (MACE) between performed and deferred PCI groups. View Table 10
Coronary pressure-derived fractional flow reserve (FFR) is the current gold standard for hemodynamic assessment of patients with intermediate stenosis without evidence of ischemia and is a useful guide for complete functional myocardial revascularization in patients with multivessel coronary artery disease (CAD) [21,22].
It has been a solid finding that coronary stenosis with an FFR value < 0.75 had a 100% positive predictive value for inducible myocardial ischemia, whereas an FFR value > 0.80 was associated with a negative predictive value of > 95% [23].
As shown in the deferral of percutaneous coronary intervention (PCI) trial with 5 years of follow-up, and even up to 15 years, PCI can be safely deferred for stenosis with an FFR > 0.80 [9]. However, several studies have reported that a small group of patients with FFR between 0.75 and 0.80, the so-called grey zone FFR, were associated with reversible myocardial ischemia [24,25].
Since the concept of grey zone FFR was firstly introduced by European Society of Cardiology Guidelines for PCI in 2005, the findings of several studies that tried to determine the optimal treatment strategies for patient with FFR within the grey zone was conflicting [26-28].
Therefore, the aim of this study was to compare intermediate-term outcomes of patients performed versus deferred Percutaneous Coronary Intervention in coronary stenosis with FFR values in the grey zone (0.75-0.80) through conducting a non-randomized controlled trial among patients recruited in 2 years period from January 2019 to January 2022.
This study included 50 coronary artery stenosis patients with an FFR value in the grey zone undergoing performed or deferred revascularization. The age of the studied group ranged from 38-67 years with mean of 53.16 (± 7.83 years). The study included 12 females (24%) and 38 males (76%). After baseline assessment of the patients, they were divided into 2 groups: Group one which had deferred PCI (46%), while the other group included patients that performed the PCI (54%).
Our study examined the prevalence of CAD risk factors among our study participants and we found that 72% of them had diabetes mellitus (DM), 70% had hypertension (HTN), 94% suffered from dyslipidemia, while 52% of the patients were smokers.
Our results were consistent with previous studies reporting the increased prevalence of these cardiac risk factors among CAD patients [23,24,29]. Nevertheless, these studies differed from ours regarding the DM prevalence (< 40%) as compared to ours > 70%. The reason for this difference is firstly the difference in the study setting, where the DM prevalence reported in these previous studies agrees with the nationally reported prevalence of DM in each of their corresponding countries.
Secondly, in our study, the majority of the participants were males (76%), and it is previously illustrated that males are almost twice as likely to develop type 2 diabetes as women [30].
Furthermore, when we examined the difference in these risk factors across both our study groups; the performed and the Deferred PCI groups, we found no statistically significant difference (p value = 0.697).
This also agrees with what both Andreou, et al. [31] and Shin, et al. [32] reported. This finding is reasonable since the recruited patients were similar in their clinical data upon which they were chosen and with similar FFR ratios and so it is expected that they would possess similar cardiac risk factors with no significant difference.
Our study examined the clinical data of the recruited patients on three timeline points: at admission with hospital course, after three months, and after six months. Regarding the baseline clinical findings, the mean FFR value was 0.771 (± 0.017). As for the culprit vessel, the majority of the patients (64%) had left anterior descending artery stenosis, while the least reported culprit vessel was the left circumflex artery (16%).
In agreement with our results, the systematic review by Du, et al. [23] showed that the median FFR ratio at baseline was 0.77 in some of their included studies, and 0.78 in the other studies. Similarly, Shin, et al. [32] reported that the median FFR at baseline was 0.75.
In terms of the distribution of the culprit vessel, previous studies also agreed with our results, where the most commonly affected coronary vessel was the left anterior descending artery, followed by the right coronary artery, and the least affected vessel was the left circumflex artery [27,32,33].
This is an expected finding since the susceptibility of the coronary arteries for occlusion was previously investigated and lately proved that the LAD artery was the most commonly occluded artery among the coronary arteries (42.4%), followed by the right coronary artery (26.8%) then the left circumflex artery (19.1%) [34-36]. Furthermore, lesions were reported to be rare in the right atrial branch, left atrial branch, and posterior left ventricular.
Additionally, our study investigated the difference in the mean FFR ratio between both our study groups, the highest mean was observed in the deferred group (0.78 ± 0.016). This difference was not statistically significant (P value = 0.157).
Likewise, no statistically significant difference was observed between either of our groups regarding the culprit vessel (P value = 0.232). These findings are also supported by previous studies [23,32].
The prevalence of major adverse cardiovascular events (MACE) among our patients at hospital course post intervention was minimal; where only 2% of the patients had target vessel myocardial infarction (one patient had peri-procedural MI).
Moreover, on comparing both groups at hospital course, all of the patients that were deferred did not present with any MACE, while 3.7% of the group that underwent performed PCI had TVMI. Nevertheless, this difference was not statistically significant (P value = 0.099).
This too was similar to what Andreou, et al. [31] and Hennigan, et al. [27] reported in their studies, where Andreou, et al. reported that after a 2.4 years follow-up period, the relative risk for MACE was 1.33 but no statistical significance was found (p value = 0.35). Likewise, Hennigan, et al. found that equal number of patients in each of the performed and the deferred groups had cerebrovascular diseases and accordingly no statistical difference was detected.
After performing a baseline assessment of our participants, they were divided into two study groups, then followed for three and six months, where we re-evaluated the patients at these two points to assess our study outcomes.
Regarding the post-three months follow up evaluation, on examining the patients as a whole, 96% of them were stable, and showed no MACE, while only one case died (deferred group).
When examining the differences between both of our study groups, more patients were asymptomatic in the performed group compared to the deferred group (96.3% vs. 95.7%). This difference, however, was not statistically significant (p value = 0.363).
Furthermore, upon examining the coronary outcomes, no major difference was noticed between both groups, where 96.3% of the patients in performed PCI were stable versus 95.7% of the patients in the deferred group. One patient in performed PCI had periprocedural MI and the affected artery was the left anterior descending, while one patient in the deferred group showed cardiovascular mortality. Nevertheless, these findings did not differ significantly between both groups (p value = 0.448).
These findings remained somewhat similar after another three months follow-up (total of six months follow-up), since we found that more patients in the deferred group were symptomatic (17.3%) compared to the group of patients who underwent PCI (7.7%). However, this difference was statistically insignificant (p value = 0.469).
Likewise, we found that the clinical outcomes remained favorable among the group of patients who performed PCI compared to the deferred group after another three months follow-up, where in the performed group only one patient was symptomatic and had an elective PCI to the RCA. On the contrary in the deferred group, 4 patients were symptomatic, where two patients suffered spontaneous MI and both had PCI to the LAD, while the other two patients had an elective PCI to the LAD & LCX. Nevertheless, no statistically significant difference was observed (p value = 0.622).
So, the majority of the patients during first three months follow-up in both our groups had no MACE, only one patient in performed PCI had TVR, and one patient in the deferred group died.
On the contrary, these findings changed slightly after another three months, were 7.7% of the patients who performed PCI had TVR, compared to 17.3% in the deferral group. The difference noticed between both groups was statistically insignificant (p value = 0.469).
In agreement with our results, Kang, et al. [37] found that the overall mortality and spontaneous MI did not differ between the groups after a mean of 2.9 years follow-up.
Compared to our results, Shin, et al. [32] found that more patients who performed PCI died compared to the deferred group after a follow- up period of 3.5 years, where 7 all cause death events were noticed in the PCI group compared to 5 events in the deferred group. This difference was statistically insignificant (p value = 0.448). Nevertheless, these results differed from our results in our six-month follow-up period.
This difference may be attributed to the difference in the follow up period between our study and theirs, since Shin, et al. [32] followed their patients for 3.5 years. Also, the mean age of the participants in the study by Shin, et al. was 64.3 and 65.1 years in the performed and the deferral group respectively, while the mean age of our participants in the PCI group was 55.1 years and 50.7 in the deferral group. This explains the difference in the death rate between both studies since older patients suffer more from post-procedure complications and may even suffer from recurrent MACE on the long term.
Similar to our results, Kubo, et al. [28] found that the death rates and adverse cardiac outcomes were more among the deferral group. But this may be attributed to the major difference in the number of patients categorized in both their groups, where 185 patients were deferred, while only 78 patients underwent PCI. Accordingly, the number of cumulative incidences differed between both their groups.
Likewise, Qin, et al. [33] stated that the major adverse cardiovascular and cerebrovascular events among the deferral patients were higher than the patients who underwent PCI (37.1% vs. 22.2% respectively). This difference in the findings may be attributed to two reasons, firstly, the different age group recruited by their study, where the mean age of their PCI group was 60.9 years and that of the deferral group was 64.4 years. Secondly, more patients in the deferral group were current smokers (40.2%) and this predisposes to recurrent MACE when combined with the risk factor of older age.
In summary, our study reveals no significant difference between patients undergoing performed or deferred PCI in regard to MACE (p-value 0.099). No significant difference was found between patients undergoing performed or deferred PCI in regard to either the clinical status & target coronary intervention, or MACE after three months follows up duration (p-value 0.363). There was no significant difference between patients undergoing performed or deferred PCI in regard to either the clinical status, presentation & target coronary intervention, or MACE after six months follow up duration (p-value 0.469).
Our study found that after the follow-up period in patients with angiographically borderline coronary lesion with grey-zone FFR (0.75-0.8), either performing or deferring coronary intervention are effective and safe.
Our study included the following limitations:
• Non- Randomization.
• Small sample size.
• Short follow-up period.
• Further studies on larger sample size to emphasize our conclusion.
• Randomization.
• Increasing the follow-up period.
No conflict of interest.
Fractional flow reserve (FFR)-guided percutaneous coronary intervention (PCI) has shown better clinical outcomes than conventional angiography-guided PCI. The optimal FFR cut-off value for revascularization is debated.
With FFR ≤ 0.75, revascularization for coronary stenosis is associated with improved clinical outcomes, whereas with FFR ≥ 0.8, medical treatment has been shown to result in favorable long-term outcomes. However, there has been controversy over revascularization decision-making for coronary stenosis with FFR between 0.75 and 0.80, the so-called grey zone.
Therefore, in this prospective non-randomized study, we compared the outcomes of patients six months after undergoing deferral versus performed percutaneous coronary intervention for coronary stenosis with grey zone FFR (0.75-0.80) values.