Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease characterized by multisystem inflammation, and is a common cause of pericarditis and pericardial effusion, but significant pericardial effusion and cardiac tamponade are rare and even rarer as the first manifestation. We report the case of a young male who presented with fever, recurrent pericarditis and polyserositis with pericardial and bilateral pleural effusion. On examination he was hemodynamically unstable and the pericardial effusion had considerable dimensions (30-33 mm), and an urgent pericardiocentesis was performed. Antinuclear antibodies with a speckled pattern were positive and the remaining auto-immunity and infectious study was unremarkable. Considering the European League against Rheumatism/American College of Rheumatology (EULAR/acr) classification criteria for SLE a score of 11 points was obtained, confirming the diagnosis. This case report illustrates a rare form of presentation of SLE, in which the first manifestation was pericarditis with polyserositis and cardiac tamponade.
Systemic lupus erythematosus, Cardiac tamponade, Polyserositis
ANA: Antinuclear Antibody; CRP: C-Reactive Protein; ECG: Electrocardiogram; ICU: Intensive Care Unit, NSAIDs: Nonsteroidal Anti-Inflammatory Drugs, SLE: Systemic Lupus Erythematosus
Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease characterized by multisystem inflammation, and is a common cause of pericarditis and pericardial effusion, but significant pericardial effusion and cardiac tamponade are rare and even rarer as the first manifestation.
A 19-years-old male patient presented to the emergency department with acute anterior chest pain and fatigue and dyspnoea for two days. The patient had no other complaints including syncope, cough, gastrointestinal or urinary complaints and he had no relevant family or past medical history. On examination his blood pressure was 123/67 mmHg, heart rate 154 bpm, respiratory rate 22 breaths per minute, oxygen saturation 93% in room air and temperature 38.5 °C. Head, eyes, nose, throat and neck examinations were unremarkable. Breath sounds were decreased in the bases with fine crackles. Auscultation of the heart revealed muffled heart sounds. The abdomen was soft and non-tender. The extremities were well perfused with strong and symmetric pulses. No oedema or jugular venous distention was appreciated. Electrocardiogram (ECG) showed sinus rhythm, normal PQ interval, QRS with normal duration and elevation of the ST segment in leads V3-V6, aVL, LI and LII and ST segment depression in aVR (Figure 1A). Arterial blood gas showed mild hypoxemia pO 2 63.8 mmHg and hyperlactacidemia 2.9 mmol/L. Laboratory tests revealed normal haemoglobin Hb 13.6 g/dL, leukocytosis 11.949/uL and neutrophilia 10.500/uL, lymphocytopenia 890/uL and normal platelet count 135.000/uL, elevated C-reactive protein (CRP) 30 mg/dL, elevated procalcitonin 0.48 ng/mL and N-terminal-pro hormone BNP of 632 pg/mL and undetected troponin I. Renal function was normal. Chest radiography showed severe cardiomegaly, bilateral pleural effusion with large right sided pleural effusion and parabronchial cuffing and perihilar haze suggestive of congestion (Figure 1B). Echocardiogram showed normal size ventricles with preserved systolic function, valves with normal morphology and function and a large circumferential pericardial effusion (22-25 mm) without collapse of the cardiac chambers or hemodynamical instability.
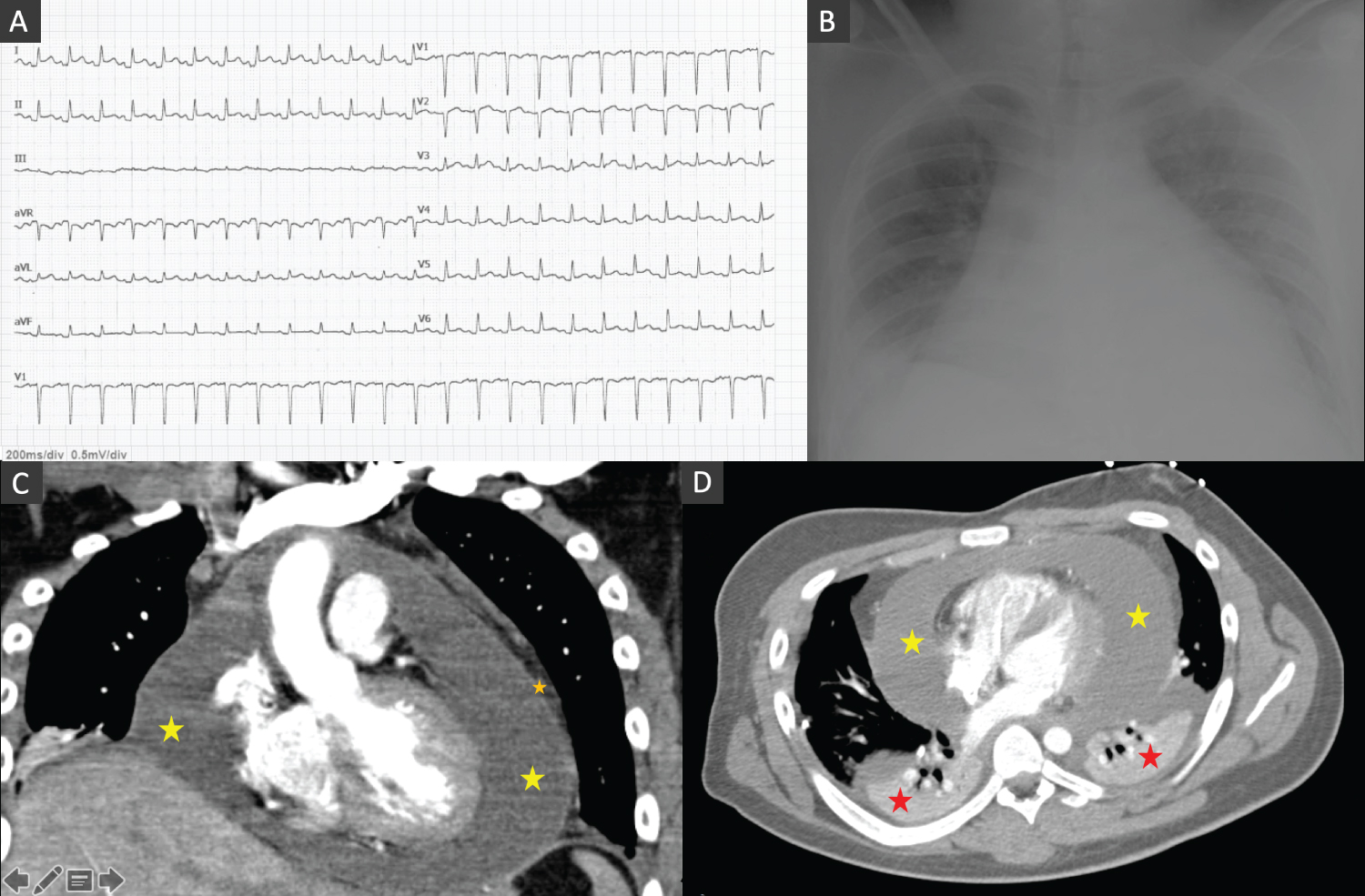 Figure 1: (A) ECG showing sinus rhythm, normal PQ interval, QRS with normal duration and elevation of the ST segment in leads V3-V6, aVL, LI and LII and ST segment depression in aVR; (B) Chest radiography showing severe cardiomegaly, bilateral pleural effusion with large right sided pleural effusion and parabronchial cuffing and perihilar haze; (C and D) Thorax-computed tomography confirmed a circumferential pericardial effusion (yellow star) with maximum dimension of 40 mm with a thick pericardium (orange star) and bilateral pleural effusion (red star) (with chest tube inserted in the right fifth intercostal space) in coronal (C) and axial (soft-tissue) view (D).
View Figure 1
Figure 1: (A) ECG showing sinus rhythm, normal PQ interval, QRS with normal duration and elevation of the ST segment in leads V3-V6, aVL, LI and LII and ST segment depression in aVR; (B) Chest radiography showing severe cardiomegaly, bilateral pleural effusion with large right sided pleural effusion and parabronchial cuffing and perihilar haze; (C and D) Thorax-computed tomography confirmed a circumferential pericardial effusion (yellow star) with maximum dimension of 40 mm with a thick pericardium (orange star) and bilateral pleural effusion (red star) (with chest tube inserted in the right fifth intercostal space) in coronal (C) and axial (soft-tissue) view (D).
View Figure 1
The patient was admitted to the Intensive Care Unit (ICU) and a right thoracentesis was performed with insertion of a chest drain in the right fifth intercostal space and a total of 600 cc of fluid were drained. Pleural fluid culture was negative and immunohistochemical analysis was compatible with exudate. A thorax-computed tomography confirmed a circumferential pericardial effusion with maximum dimension of 40 mm with a thick pericardium and bilateral pleural effusion (with chest tube inserted in the right fifth intercostal space) (Figure 1B, Figure 1C and Figure 1D). Despite the absence of hemodynamically instability considering the size of the pericardial effusion of unknown etiology a diagnostic and therapeutic pericardiocentesis was executed with draining of a total of 700 cc of sero-hematic fluid. Immunohistochemical analysis was compatible with exudates with inflammatory cells. Autoimmunity laboratory tests were requested. The patient received treatment with empirical antibiotic with amoxicillin, nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine and remained hemodynamically stable with normalization of the heart rate and resolution of the fever. Lung congestion improved and the chest tube was removed after three days. Two weeks after he was admitted, he was discharged with resolution of the pericardial and pleural effusion and resolution of the inflammatory parameters.
One week later he returned to the emergency department with acute dyspnea and recurrence of fever. On examination he was hypotensive 89/46 mmHg, tachycardic 147 bpm, respiratory rate was 24 breaths per minute, oxygen saturation 93% in room air and he was febrile with temperature of 38.2 º C. On echocardiogram the pericardial effusion had large dimensions (30-33 mm) with collapse of the right cavities and significant tricuspid inflow variation and an urgent pericardiocentesis was performed with success with hemodynamically normalization of the blood pressure and heart rate (Figure 2). Laboratory results were similar to the first episode with leukocytosis, neutrophilia, lymphopenia and elevated C-reactive protein with undetected troponin I. Chest radiography revealed recurrence of bilateral pleural effusion. Pericardial and pleural cultures were negative. Antinuclear antibody (ANA) with a speckled pattern was positive 1:320. Anti-neutrophil cytoplasmic antibody, Anti-mitochondrial antibodies, Anti-dsDNA was all negative. Interferon-Gamma Release Assay, atypical and serology screen including herpesviruses, enterovirus, adenovirus, Epstein-Barr virus, coxsacki A and B, viral hepatitis, Cytomegalovirus, Human immunodeficiency virus, and Aspergillus were unremarkable. Complement C4 levels were mildly low 7.6 mg/dL and C3 was normal. Considering the European League against Rheumatism/American College of Rheumatology (EULAR/acr) classification criteria for SLE a score of 11 points was obtained confirming SLE. The patient was treated with high doses of NSAIDs, colchicine and high dose corticosteroids. He remained stable and was discharged 7 days after.
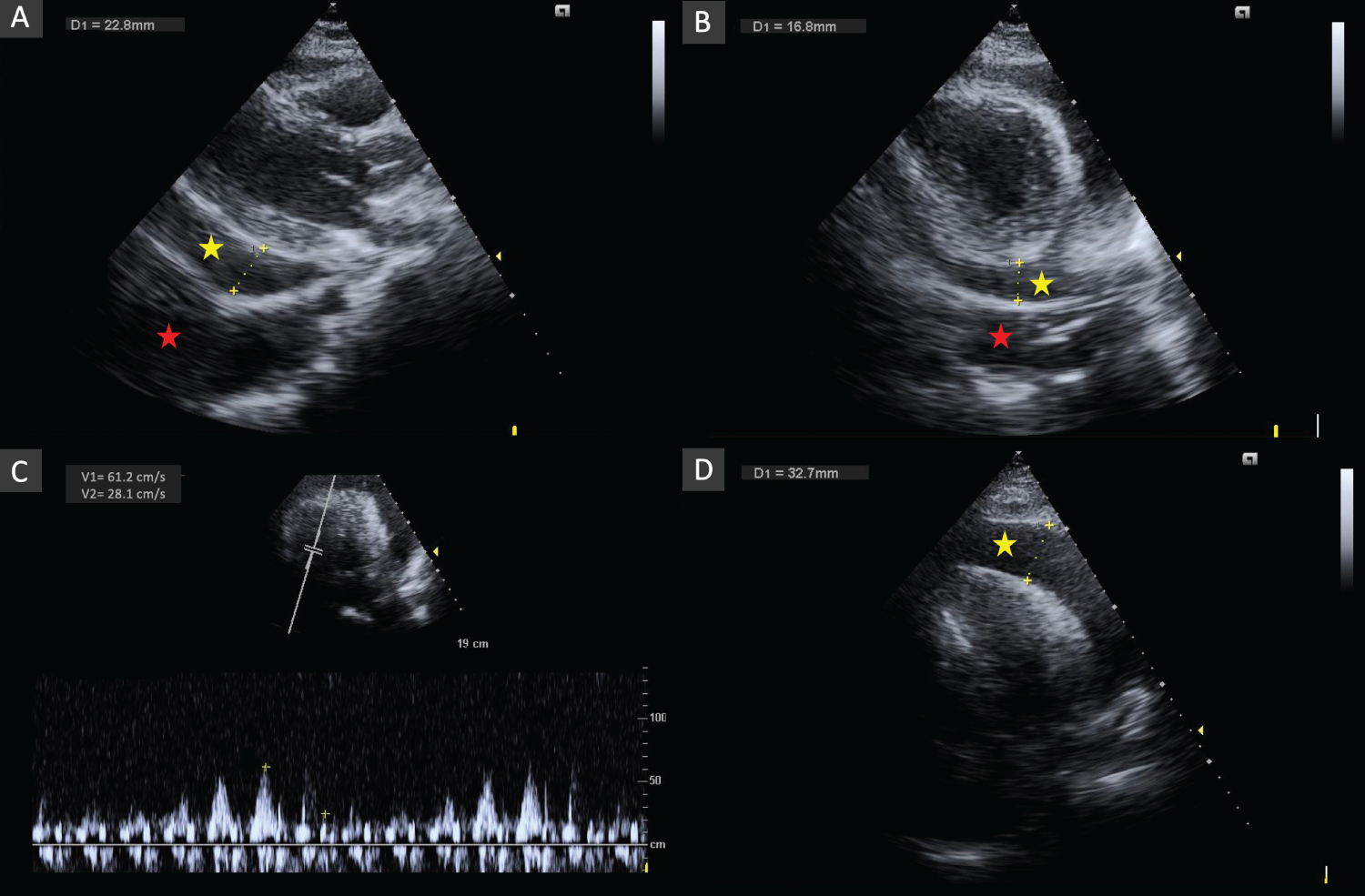 Figure 2: A) Echocardiography in parasternal long-axis; B) Parasternal short-axis and apical 4-chamber (C and D) Views showing pericardial effusion with large dimensions (30-33 mm) (yellow star) with collapse of the right cavities and significant tricuspid inflow variation (46%) and pleural effusion (red star).
View Figure 2
Figure 2: A) Echocardiography in parasternal long-axis; B) Parasternal short-axis and apical 4-chamber (C and D) Views showing pericardial effusion with large dimensions (30-33 mm) (yellow star) with collapse of the right cavities and significant tricuspid inflow variation (46%) and pleural effusion (red star).
View Figure 2
One month later the patient had another recurrence with polyserositis but with smaller pleural and pericardial effusion without hemodynamically instability. Diuretic and corticosteroids were titrated and the patient improved without the need for thoracentesis or pericardiocentesis and was discharged after 4 days.
To the date the patient remains asymptomatic and NSAIDs, colchicine and corticosteroids have been tapered and suspended without recurrence. Follow-up echocardiogram showed a very mild pericardial effusion without hemodynamically compromise or constriction.
SLE is a chronic autoimmune disease characterized by multisystem inflammation. Cardiac involvement is common and often presents as pericarditis and may be present in up to 25% of the patients throughout the course of the disease [1,2]. Pleuritis with pleural effusion is common and has been describe in up to 30-50% of the cases, but it is usually low volume and rarely needs invasive procedures to drain [2]. Pericardial effusion can be present in up to 2% of the patients and significant pericardial effusion or cardiac tamponade are present in less than 1% of the cases of SLE and are even rare as the first manifestation [1]. One study reported incidence of up to 22% of tamponade but usually years after the diagnosis of SLE [3]. Symptomatic polyserositis with pleural, pericardial and/or ascites has been identified in 12 to 30% of the patients with SLE [4,5]. Although SLE is more common in female patients some studies have reported a higher incidence of pericardial serositis in male patients [1].
The diagnosis of SLE encompasses a clinical challenge and requires a high clinical suspicion. In this case after positive ANA with a speckled pattern were found the EULAR/acr classification criteria were assessed and a score of 11 points was obtained confirming the diagnosis (acute pericarditis, fever and low complement C4 level) [6]. A positive ANA test is a nonspecific finding, but in this case the presence of recurrent pericarditis with large pericardial effusion and the presence of other findings as lymphopenia were red flags that raise the suspicion of an underlying auto-immune disease. No sign of peritonitis or ascites was identified as well as other typical signs of SLE as cutaneous, arthritis, renal or neurological criteria.
The prognosis of polyserositis associated with SLE is usually good as long as it is identified and appropriate and attempted treatment is started [4]. Relapse of serositis is rare and often responded to NSAIDs and corticosteroids as it happened in this case [4].
This case report illustrates a rare form of presentation of SLE, in a young male, in which the first manifestation was recurrent pericarditis with polyserositis and cardiac tamponade.
The authors have nothing to disclose.
Self finance.
Maria Inês Barradas wrote the clinical case. Fabiana Duarte and Inês Coutinho dos Santos edited the manuscript. Anavela Tavares and Dinis Martins supervised and corrected the manuscript.