Background: Acute coronary syndrome (ACS) is a major cardiovascular problem. According to the World Health Organization (WHO) in 2015, cardiovascular disease caused 17.5 million deaths, while ACS caused 7.4 million deaths. ACS is a condition when the plaques are accumulated in coronary arteries that supply oxygen to the heart muscles. The ST-Elevation Myocardial Infarction (STEMI) is an indicator of total coronary artery occlusion. This condition requires revascularization to restore blood flow and myocardial reperfusion using fibrinolytic agents or primary Percutaneous Coronary Intervention (PCI). Early reperfusion therapy can reduce in-hospital mortality and show better outcomes in ACS patients.
Objective: To determine the prevalence of ACS patients and the risk factors of in-hospital mortality of STEMI patients at Bekasi District General Hospital in 2021.
Methods: This research was a descriptive cross-sectional study using secondary data from medical records. The data were presented in diagrams and tables.
Results: There were 117 cases of ACS in 2021. They were 14% STEMI, 15% Non-ST Elevation Myocardial Infarction (NSTEMI), and 71% Unstable Angina Pectoris (UAP). Most patients were male (54%), and aged < 65-years-old (85%). The in-hospital mortality was 19% STEMI, 17% NSTEMI, and 12% UAP. Among 16 STEMI patients, 81% were male and 94% were aged < 65-years-old. There were 69% who came to the emergency room < 12 hours and only 50% underwent fibrinolytic.
Conclusion: The risk factors of in-hospital mortality of STEMI patients were 40% late onset, 23% anterior STEMI, 20% hypertension, 60% diabetes mellitus, 50% chronic kidney disease, 33% tachycardia, and 100% Killip III.
Acute coronary syndrome, ST-elevation myocardial infarction, In-hospital mortality
ACS: Acute Coronary Syndrome; WHO: World Health Organization; STEMI: ST-Elevation Myocardial Infarction; PCI: Percutaneous Coronary Intervention; NSTEMI: Non-ST Elevation Myocardial Infarction; UAP: Unstable Angina Pectoris; ECG: Electrocardiogram; CKMB: Creatine Kinase-MB; LVH: Left Ventricular Hypertrophy; LBBB: Left Bundle Branch Block; ER: Emergency Room; JAC: Jakarta Acute Coronary Syndrome
Coronary heart disease is a disease caused by plaque accumulation in the coronary arteries that supply oxygen to the heart muscles [1]. The acute coronary syndrome is also caused by increased oxygen demand, reduced blood oxygen transport, and is often caused by reduced coronary flow as a result of narrowing or obstruction of the arteries due to atherosclerosis [2]. The acute coronary syndrome consists of Unstable Angina Pectoris (UAP), non-ST elevation myocardial infarction (NSTEMI), and ST elevation myocardial infarction (STEMI) [1,3]. Angina pectoris is a clinical syndrome caused by an imbalance between demand and supply of coronary artery flow [3]. Non-ST Elevation Myocardial Infarction (NSTEMI) is an acute coronary syndrome with clinical symptoms of chest pain typical of infarction, electrocardiogram (ECG) without ST segment elevation, and elevated cardiac enzymes (CKMB, troponin T). NSTEMI can cause various complications, such as acute pulmonary edema, cardiac arrest, and even death [4].
Acute ST Elevation Myocardial Infarction (STEMI) is a clinical syndrome defined by myocardial ischemia symptoms related to persistent ST elevation and release of myocardial necrosis biomarkers [5]. Acute myocardial infarction is diagnosed based on the typical clinical symptoms of chest pain, increased cardiac biomarkers, and changes in electrocardiogram patterns [6]. Increased cardiac-specific markers found in acute myocardial infarction are MB isoenzyme of creatinine kinase (CKMB), troponin T, and troponin I. CKMB isoenzymes are plentiful in cardiac muscle cells. Increased levels of CKMB indicate the extent and severity of infarction in the heart muscle [6]. On the electrocardiogram, an assessment of ST elevation is performed at the J point and is found in two opposite leads. The ST segment elevation threshold value in the diagnosis of STEMI for males and females in most leads is 0.1 mV [7]. ST segment elevation without Left Ventricular Hypertrophy (LVH) or Left Bundle Branch Block (LBBB) is a new ST segment elevation at the J point > 2 mm (0.2 mV) in males or > 1.5 mm (1.5 mV) in females in leads V2-V3 and/or > 1 mm (0.1 mV) in another precordial lead or limb lead, in at least 2 contiguous leads [5,7].
Typical chest pain in STEMI located in the substernal, with > 20 minutes duration, accompanied by cold sweat, chest pain that is described as feeling like crushed and can spread to the left arm, back, jaw, or epigastrium. Risk factors for STEMI include diabetes, cholesterol, high blood pressure, chronic kidney disease, and heredity [3]. STEMI is an indicator of total coronary artery occlusion. This condition requires revascularization to restore blood flow and myocardial reperfusion as soon as possible, either medically using fibrinolytic agents or mechanically through primary percutaneous coronary intervention [7]. Several factors must be considered when choosing reperfusion therapy. Initiation of reperfusion management does not need to wait for the results of increased cardiac biomarkers [5,7].
Percutaneous coronary intervention (PCI) is a non-surgical intervention procedure using a catheter to dilate or open narrowed coronary arteries due to atherosclerosis or thrombosis with ballooning or deploying a stent. For STEMI patients who come to a hospital with PCI facilities, primary PCI must be performed within 90 minutes with the onset of complaints < 12 hours. While patients who come to a hospital without PCI facilities, fibrinolytic therapy should be initiated at < 12 hours of onset and if primary PCI cannot be performed within 120 minutes of first medical contact [3,5]. Early reperfusion therapy can reduce in-hospital mortality rates and show better outcomes in patients with acute myocardial infarction. However, STEMI still causes various complications, including myocardial dysfunction, heart failure, cardiogenic shock, arrhythmias, mechanical complications, and pericarditis [8].
Based on the background explanation above, the problem that can be concluded is how the distribution of acute coronary syndrome patients who were admitted through the emergency room and an overview of what risk factors can cause mortality of acute coronary syndrome patients during hospitalization in Bekasi District General Hospital during January to December 2021.
This study is a descriptive cross-sectional study using secondary data. The study subjects included all the patients aged over 35 that admitted through the ER in Bekasi District General Hospital from January to December 2021 with chest pain or shortness of breath and later hospitalized. The research is conducted from December 28 th , 2021 to March 28 th , 2022. This study used secondary data from the medical records of Bekasi District General Hospital.
The initial study was carried out by collecting register data for all patients with acute coronary syndrome who were admitted through the ER from January to December 2021. From the data register, there were 149 patients with acute coronary syndrome in the past year. Consequently, a search for medical record status was conducted to collect the necessary data. Out of the 149 statuses, 12 statuses could not be found and 20 statuses were not included in the inclusion criteria. Therefore, the final sample in this study is 117 statuses (Figure 1).
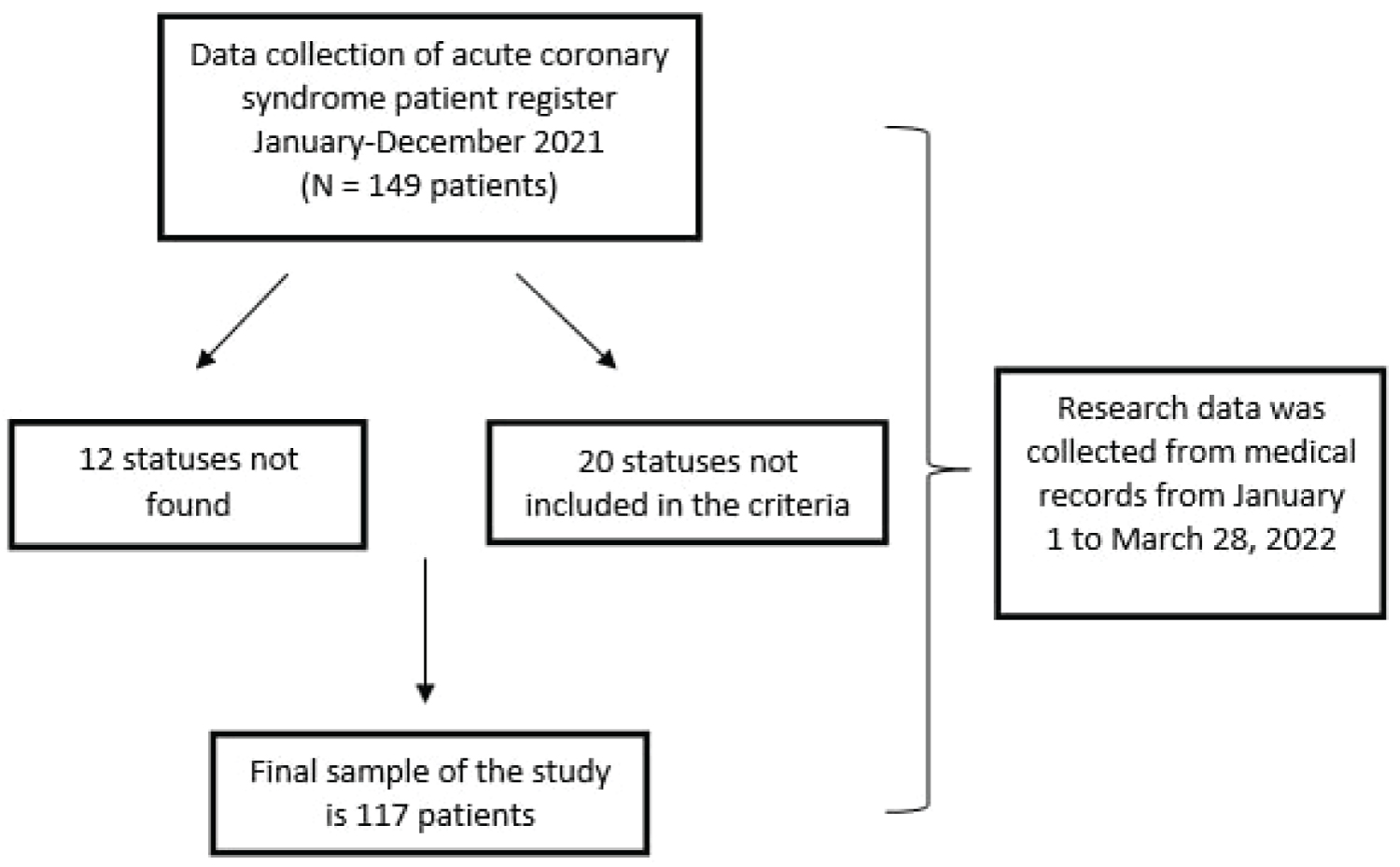 Figure 1: Sampling process.
View Figure 1
Figure 1: Sampling process.
View Figure 1
This study shows that the number of acute coronary syndrome cases admitted through the ER in the medical record data of Bekasi District General Hospital during the period January 1 to December 31, 2021 was 149 cases. Later, out of these 149 cases, 12 cases had no medical records, and 20 cases were not included in the inclusion criteria. Thus, the final sample of this study was 117 cases. Out of the 117 cases, there were 16 cases of STEMI (14%), 18 cases of NSTEMI (15%), and 83 cases of UAP (71%). The distribution of Acute Coronary Syndrome (ACS) patients in Bekasi District Hospital in 2021 can be seen in Figure 2.
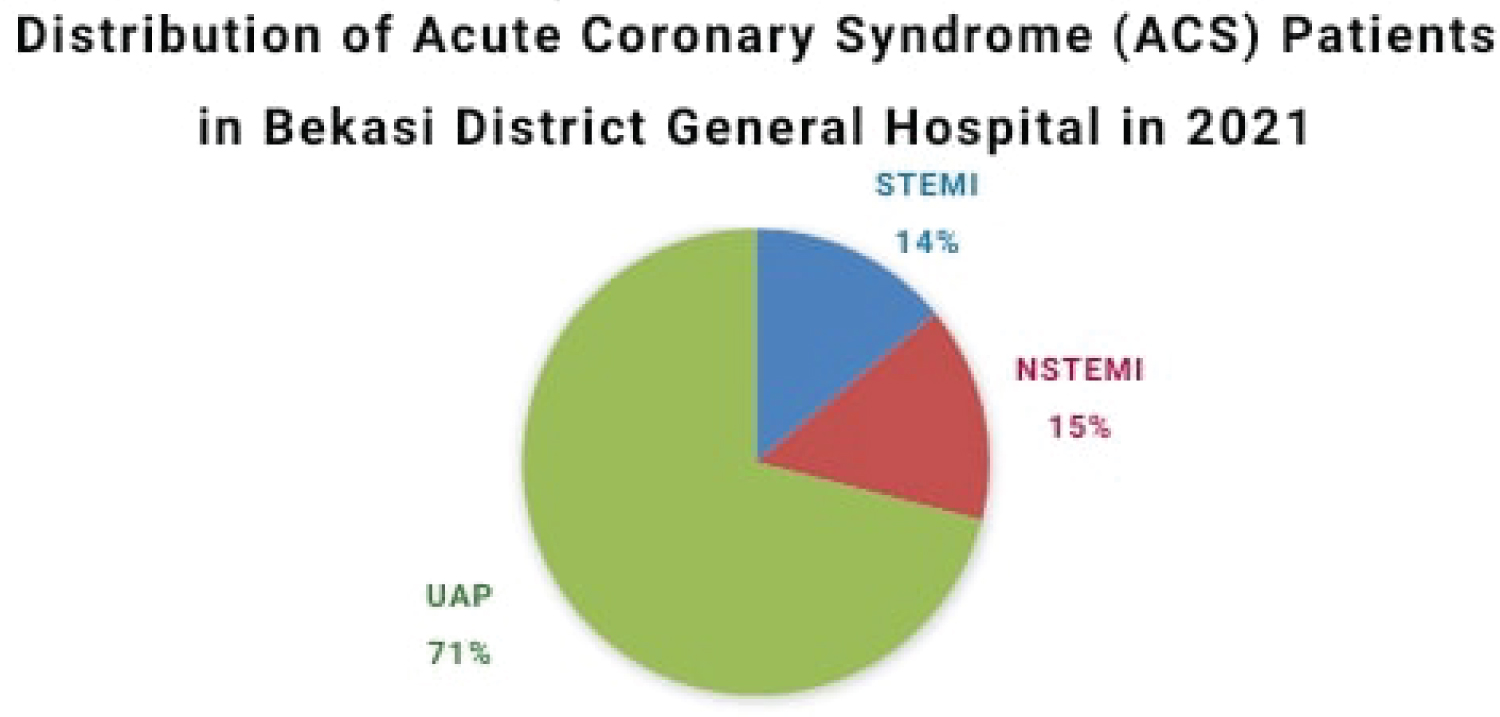 Figure 2: Distribution of Acute Coronary Syndrome (ACS) patients in Bekasi District General Hospital in 2021.
View Figure 2
Figure 2: Distribution of Acute Coronary Syndrome (ACS) patients in Bekasi District General Hospital in 2021.
View Figure 2
This study found that more than half of acute coronary syndrome patients are male patients (54%), while the rests are female patients (46%). Age is a part of the risk factor for acute coronary syndrome. This study classified the patients’ age into the under 65-years-old age group and the over 65-years-old age group. Out of 117 patients, 99 patients are under 65-years-old (85%), and 18 patients are over 65-years-old (15%).
Patients’ comorbidities were dominated by hypertension (85%) with 99 patients, 46 patients suffering from diabetes mellitus (39%), and 36 patients suffering from chronic kidney disease (31%). Out of 117 acute coronary syndrome cases in Bekasi District General Hospital during the period of 1 January to December 31, 2021, 16 of these cases died during in-hospital treatment at the hospital. The dead cases were 3 STEMI cases (19%), 3 NSTEMI cases (17%), and 10 UAP cases (12%). Among the 16 acute coronary syndrome patients that died, 7 of them are male (11%) and 9 of them are female (17%). Based on the age group, the majority of acute coronary syndrome patients that were died from the under 65-years-old age group (15%), while there was only 1 patient over 65-years-old that died (6%). Comorbidities among the patients that died included hypertension; 11 patients (11%), diabetes mellitus; 9 patients (20%), and chronic kidney disease; 9 patients (25%) (Table 1).
Table 1: Acute coronary syndrome patient characteristics. View Table 1
Clinical and demographic data of STEMI patients in Bekasi District General Hospital in 2021 is summarized in Table 2. Out of 16 STEMI patients, the majority of them are under 65-years-old, which were 15 patients (94%) and 13 male patients (81%). Out of these 16 STEMI patients, three of them died (20%) during in-hospital treatment and three of them were under 65-years-old. The majority of the patients that died were male, which were 2 patients (15%).
Table 2: STEMI patient characteristics. View Table 2
STEMI patients that come to the ER of Bekasi District General Hospital complained about chest pain with onset of attack < 12 hours, which were 11 patients (69%). Only five patients (31%) come to the ER with the onset of attack > 12 hours. Out of 11 patients with initial onset < 12 hours, only 8 of them received fibrinolytic therapy, 2 patients did not receive it due to fibrinolytic contraindications, while the other one rejected the fibrinolytic therapy. Most of the acute myocardial infarctions were located in the anterior part of the heart, with 13 patients (81%), while three patients (19%) were in the non-anterior part of the heart. All three patients that died had a myocardial infarction in the anterior part of the heart.
Risk factors of STEMI patients are hypertension (94%), diabetes mellitus (31%), and chronic kidney disease (13%). Symptoms and clinical signs, of the patients, when they arrived were low systolic blood pressure (31%), high pulse rate (19%), and no arrhythmia (0%). Killip classifications when the patient arrives are Killip I (13%), Killip II (44%), Killip (13%), and Killip IV (31%) (Table 2).
Acute coronary syndrome is classified into three types, acute ST elevation myocardial infarction with (STEMI), acute non-ST elevation myocardial infarction (NSTEMI), and unstable angina pectoris (UAP). Unstable angina pectoris and NSTEMI can be distinguished from cardiac biomarkers. If a significant increase is found, the diagnosis is NSTEMI and if there is no significant increase, the diagnosis is UAP [7]. The result in Figure 2 is in line with the data register from the Jakarta Acute Coronary Syndrome (JAC) in 2008-2009 where there were more UAP patients than STEMI and NSTEMI patients [9].
The result is also in line with the study finding in 2014 which stated that the 41-60 age groups is the most affected age group [10]. The risk of developing acute coronary syndrome is increasing in men who are over 45-years-old and women who are over 55-years-old [10]. Patients’ comorbidities can also be a risk factor for acute coronary syndrome. This is explained by the result in Figure 2 which was in line with a study finding in 2018 that found that hypertension is the most common risk factor for acute coronary syndrome patients [11]. Increased systemic blood pressure in hypertension causes resistance to the blood pump from the left ventricle and causes ventricular hypertrophy. Ventricular hypertrophy causes an increase in myocardial oxygen demand thus increasing the workload of the heart. Ultimately, this can trigger angina and myocardial infarction. The incidence of acute coronary syndrome in patients with hypertension is five times greater than in normotensive patients. This shows that hypertension is a major risk factor for acute coronary syndrome [11].
The second most common risk factor is diabetes mellitus. Patients with diabetes mellitus have a 200% greater risk of experiencing acute coronary syndrome than patients without diabetes mellitus. Another study states that male patients with diabetes mellitus have a 50% greater risk of experiencing acute coronary syndrome, while female patients with diabetes mellitus have twice the risk compared to patients without diabetes mellitus [11].
According to the 2018 Handbook of Management of Acute Coronary Syndrome- Buku Pedoman Tata Laksana Sindrom Koroner Akut , the prevalence of NSTEMI and UAP is greater than STEMI. NSTEMI patients’ initial mortality is lower than STEMI patients, however, after 6 months, the mortality of both is comparable. In the long term, NSTEMI patients’ mortality will be greater subsequently [7]. Gender, age, and comorbid risk factors for acute coronary syndrome patients affect mortality. The results in Table 1 is in line with a study finding in 2017 which found that the causes of cardiogenic shock after acute coronary syndrome can be exacerbated by old age, diabetes mellitus, previous myocardial infarction, chronic occlusion of the ascending left coronary artery, and decreased ejection fraction which led to death [12].
According to a research finding in 2017, the number of mortalities in acute coronary syndrome patients that were not treated properly is 40% and the majority of the death occurred in the first two hours since the initial onset (Table 2). The mortality and morbidity that occurs in STEMI patients increases with age. Besides, STEMI has a high mortality number, oftentimes due to complications. The predictors of STEMI patient mortality include Killip III and IV, arrhythmia, anterior STEMI, non-reperfusion, chronic kidney disease, tachycardia, STEMI onset > 12 hours, and diabetes mellitus [12].
The cause of death in myocardial infarction is multifactorial and depends on elapsed time duration since the initial attack. Sudden death is commonly caused by ischemia precipitating ventricular arrhythmias during the acute phase of myocardial infarction. Other complications that commonly occur are ventricular tachycardia/ventricular fibrillation (13%), left ventricular dysfunction (11.9%), cardiogenic shock (10.7%), atrial tachycardia/atrial fibrillation (7.1%), and right ventricular infarction (7.1%). Mortality in patients who did not receive reperfusion therapy was 13.2%. The purpose of reperfusion is not only for restoration of arterial patency but also for restoration of coronary flow which has been shown to be associated with reduced heart wall motion abnormalities and improved clinical outcomes [12].
Patients with a previous acute myocardial infarction had the same hospital outcomes as patients without a previous acute myocardial infarction but had a higher recurrence rate at 6 months. Refractory ischemia or recurrent ischemia is symptomatic ischemia within 10 minutes with ST segment deviation or definitive T-wave inversion, and/or hypotension, pulmonary edema, or a heart murmur representing myocardial ischemia (despite the use of nitrates and beta-blockers or calcium channel blockers), occurs in up to 20% of ischemic patients. Refractory ischemia has mortality within 30 days two times greater than patients with ST segment elevation and even greater mortality risk than patients without ST segment elevation [12].
Based on the study and discussions, it can be concluded that:
1. The number of acute coronary syndrome patient that admitted through the ER of Bekasi District General Hospital in 2021 is 149 cases. There are 12 cases without medical records and 20 cases excluded from the inclusion criteria. Thus, the final sample in this study is 117 cases.
2. Acute coronary syndrome patients are classified into 16 STEMI patients (14%), 18 NSTEMI patients (15%), and 83 UAP patients (71%).
3. Most patients of acute coronary syndrome were male, with a total of 63 patients (54%) while the others were female, with a total of 54 patients (46%).
4. Most patients with acute coronary syndrome were under 65-years-old, with a total of 99 patients (85%), and the rest were under the age of 65, with a total of 18 patients (15%).
5. The risk factor for acute coronary syndrome patients were 99 hypertension patients (85%), 46 diabetes mellitus patients (39%), and 36 chronic kidney disease patients (31%).
6. The number of acute coronary syndrome patients that died during in-hospital treatment was 16 patients, including three STEMI patients (19%), three NSTEMI patients (17%), and ten UAP patients (12%). There were 7 male patients (11%) and nine female patients (17%). The number of patients under the age of 65 is 15 patients (15%), while the other patient over the age of 65 is only one patient (6%). The risks factor included 11 hypertension patients (11%), nine diabetes mellitus patients (20%), and nine chronic kidney disease patients (25%).
7. Out of 117 cases, the number of STEMI patients is 16, and three of them have died during in-hospital treatment.
8. Most STEMI patients are under the age of 65-years-old, with a total of 15 patients (94%), while there was only one patient over the age of 65 (6%).
9. Most STEMI patients were male patients, with a total of 13 patients (81%) and the other were female patients with a total of three patients (19%).
10. STEMI patients that come through the ER with clinical symptoms of chest pain with < 12 hours onset are 11 patients (69%), while patients with > 12 hours onset are five patients (31%).
11. STEMI patients that received fibrinolytic therapy are eight patients (50%) and only patients with initial onset < 12 hours received the therapy. There were two patients who did not receive the fibrinolytic due to contraindications and there was one patient that rejected the fibrinolytic therapy.
12. Most of the acute myocardial infarctions were located in the anterior part of the heart with a total of 13 patients (81%), while the rest were located in the non-anterior part of the heart with a total of three patients (19%).
13. STEMI risk factors were 15 hypertension patients (94%), five diabetes mellitus patients (31%), and two chronic kidney disease patients (13%).
14. Symptoms and clinical signs when STEMI patients arrived including 5 low systolic blood pressure (31%), high pulse rate (19%), and no arrhythmia (0%).
15. Killip classifications when STEMI patients arrived are 2 Killip I patients (13%), seven Killip II patients (44%), two Killip III patients (13%), and five Killip IV patients (31%).
1. Using analytical research methods to study the correlation between the risk factors with acute coronary syndrome condition.
2. Using patient data that received PCI procedure.
3 .Using this study as a basis for further research with a wider period of acute coronary syndrome patient registers.