Giant coronary artery aneurysm is an uncommon finding during coronary angiogram. There is limited data or consensus on the management of patients with giant coronary artery aneurysm in the setting of acute coronary syndrome.
We present a unique case of a recurrent thrombotic occlusion of the right coronary artery presenting as recurrent inferior wall ST segment elevation myocardial infarction (STEMI) requiring percutaneous coronary intervention. He had failed trial of novel anticoagulant with anti-platelet therapy and was switched to triple therapy of a vitamin K antagonist and dual anti-platelet regime after the second percutaneous coronary intervention. There is limited consensus on the optimal anti-thrombotic regime for patients with giant coronary artery aneurysm presenting with recurrent thrombosis. Further studies looking into optimal combination therapy are needed to fill this current gap in knowledge.
Thrombosis, Giant coronary artery aneurysm, Myocardial infarction, STEMI
We present a unique case of a 62-years-old gentleman who was admitted for recurrent acute inferior ST-segment myocardial infarction (STEMI) due to recurrent acute thrombosis of a giant right coronary artery aneurysm. Mr ABH had no known prior medical illnesses and he was a non-smoker. He presented to the Emergency Department with complaints of severe chest pressure. A 12 lead electrocardiogram (ECG) showed ST segment elevation in the inferior leads II, III and aVF (Figure 1).
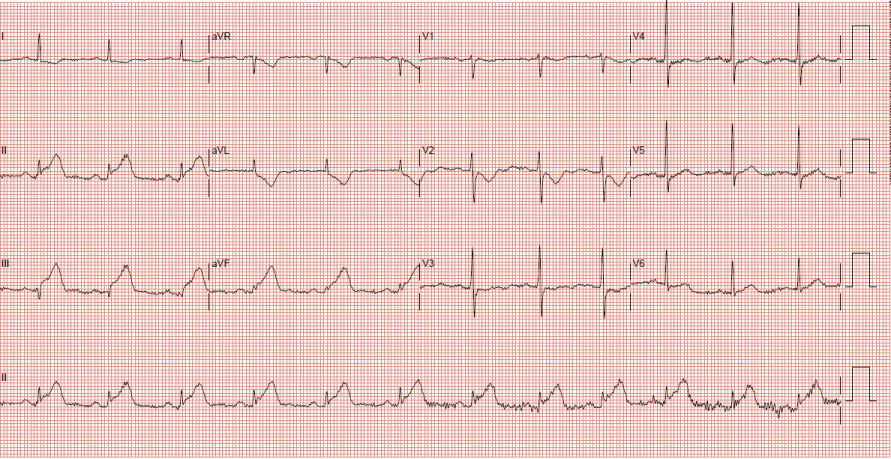 Figure 1: Showing inferior ST segment elevation on ECG.
View Figure 1
Figure 1: Showing inferior ST segment elevation on ECG.
View Figure 1
He was loaded with oral Aspirin 300 mg, Ticagrelor 180 mg and underwent an emergency percutaneous coronary intervention (PCI). A diagnostic coronary angiogram performed via the right radial artery approach showed huge aneurysmal coronary arteries with slow flow in the left coronary system as well as the right coronary artery (RCA) (See Figure 2a, Figure 2b, Figure 3a and Figure 3b). There was an acute thrombotic occlusion of the mid segment of a giant RCA aneurysm.
 Figure 2: a,b) Showing aneurysmal changes in the left coronary arteries.
View Figure 2
Figure 2: a,b) Showing aneurysmal changes in the left coronary arteries.
View Figure 2
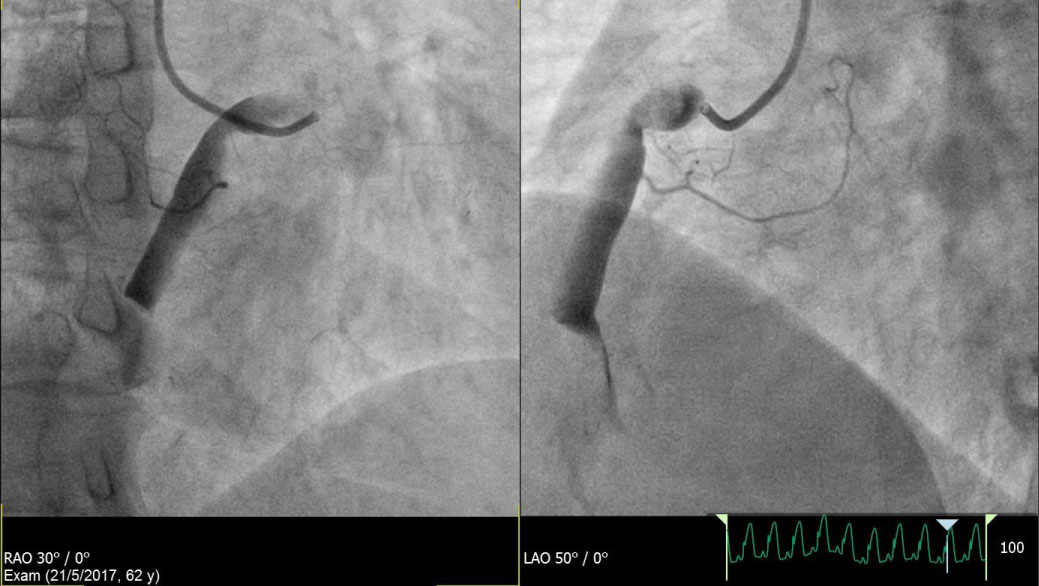 Figure 3: a,b) Showing acute thrombotic occlusion of the mid segment of the giant RCA aneurysm.
View Figure 3
Figure 3: a,b) Showing acute thrombotic occlusion of the mid segment of the giant RCA aneurysm.
View Figure 3
We proceeded with PCI to the culprit lesion at the mid segment of the RCA. A trial of manual aspiration thrombectomy using a Thrombuster™ (Kaneka Medix Corp) was attempted to no avail. Rheolytic thrombectomy was then performed using Angiojet™ (Boston Scientific) and TIMI 3 flow was achieved at the end of the procedure. However, there was a visible residual thrombus noted at the mid segment of the RCA. There was no coronary stent deployed as we did not have any available stents to match the size of the coronary artery aneurysm. There was resolution of chest pain symptoms and improvement in the ST segment elevation by the end of the procedure.
Mr ABH was started on an infusion of intravenous Eptifibatide (glycoprotein IIb/IIIa inhibitor) for 24 hours post PCI. Mr ABH was subsequently discharged with oral Clopidogrel 75 mg and Rivaroxaban 20 mg once daily. His left ventricular ejection fraction was 45%. There was no atrial fibrillation documented during his hospitalization.
Unfortunately, Mr ABH presented again 4 months later with a recurrent inferior STEMI. He was brought to the cardiac catheterization laboratory for emergency PCI. Again, there was a total thrombotic occlusion at the aneurysmal segment of the mid RCA.
Rheolytic thrombectomy was again performed using the Angiojet™ (Boston Scientific). There was a residual thrombus despite multiple attempts at balloon dilatation and thrombectomy. Further PCI attempt was not attempted as TIMI3 flow was achieved and the patient had resolution of chest pain symptoms. He was started on an infusion of intravenous Eptifibatide (glycoprotein IIb/IIIa inhibitor) for 24 hours post PCI (Figure 4a and Figure 4b).
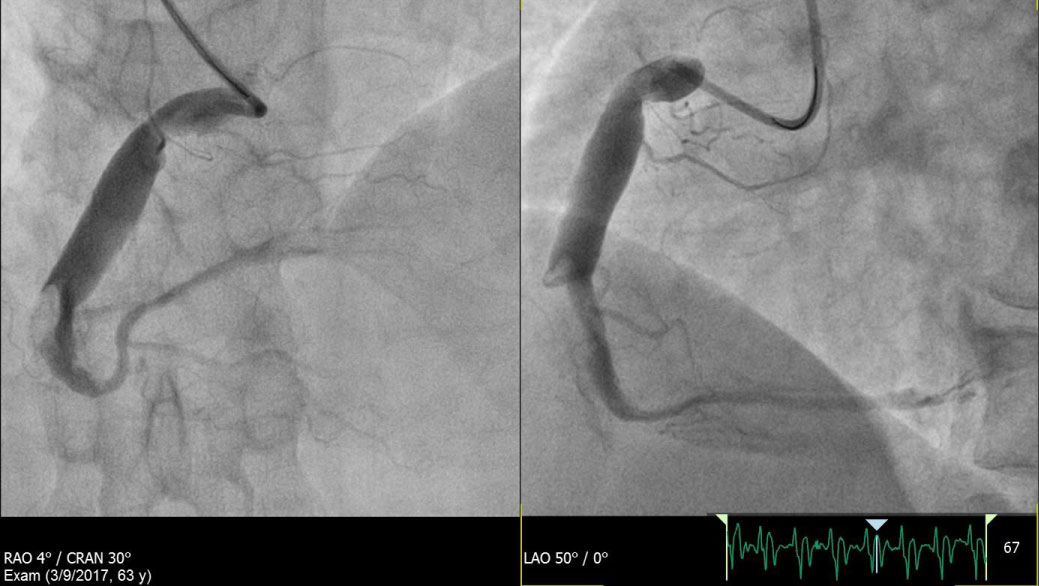 Figure 4: a,b) Showing final result post PCI.
View Figure 4
Figure 4: a,b) Showing final result post PCI.
View Figure 4
This time, Mr ABH was treated with dual anti-platelets (Aspirin 100 mg and Clopidogrel 75 mg once daily) as well as oral warfarin (with a target international normalized ration (INR) of 2-3). His left ventricular ejection fraction remained at 45% on discharge. He was switched from the triple therapy to just oral Clopidogrel 75 mg and warfarin once daily after 6 months. Mr ABH has remained well on follow up in the outpatient clinic for the past 18 months with no recurrence of chest symptoms.
Coronary artery aneurysms are uncommon and are described as a gross dilatation of a coronary artery by more than 1.5 times the diameter of a normal reference segment [1]. The incidence of coronary artery aneurysms are ranges from 0.2%-10%. Giant coronary artery aneurysm is defined as such when the diameter exceeds 8 mm [2-5]. The prevalence of giant coronary artery aneurysms is reported to be around 0.02% and with a predilection for the right coronary artery [6-8].
Patients with giant coronary artery aneurysms can suffer from complications such as myocardial ischaemia/infarction or even rupture of the aneurysmal coronary artery. There is limited data to address the management of acute coronary thrombosis in coronary artery aneurysm. Systemic anticoagulation had been proposed by Swanton, et al. [9] to mitigate the risk of coronary artery aneurysm thrombosis. The use of Warfarin and aspirin combination had shown reduction in rates of myocardial infarctions and coronary artery occlusions in a meta-analysis by Su, et al. [10].
Common strategies involve the use of anti-platelet or anti-coagulant therapies although this is lacking in evidence [11]. In this case where the patient initially presented with acute thrombotic occlusion of the giant coronary artery aneurysm, he was treated with a combination of single antiplatelet therapy (Clopidogrel 75 mg once daily) and a novel anti-coagulant Rivaroxaban 20 mg once daily (Xarelto™, Bayer). Unfortunately, the patient developed a recurrent thrombotic occlusion again 4 months later. Following a repeat emergent PCI, he was treated with a combination of dual anti-platelet therapy consisting of Aspirin, Clopidogrel as well as a vitamin K antagonist Warfarin. This regime appeared to be more successful. He was changed to single anti-platelet Clopidogrel and Warfarin after 6 months. He had remained well for over 18 months with no recurrence of ischaemic events. There are limited options for therapies directed at the giant coronary artery aneurysm as there are no available coronary stents to match the diameter of the aneurysm. Unfortunately we do not have any large sized covered stents, vascular stents in our cardiac catheterization laboratory facility. The use of covered stents is an alternative in selected cases depending on the size of the aneurysmal segment [3,12]. In this case of gross coronary aneurysm (measuring at least 9-10 mm in diameter), we had no available stents to match the size of the vessel. Best attempts have been made to reduce the thrombus burden as much as possible with the use of aspiration thrombectomy devices. The management strategy that will likely have the greatest impact will be the use of combination of anti-thrombotics.
This case demonstrated the failure of the combination of novel anticoagulant with single antiplatelet regime. However, we must bear in mind that the failure of treatment in this case relates only specifically to only one of the few available novel anticoagulants. The optimal anti-thrombotic regime remains unclear due to the limited clinical experience. It is also important to be cognizant of the possibility of other complications such as rupture. Surgical ligation remains a possible treatment option should the patient present with further ischaemic events.
Further studies will be needed to provide more evidence to guide the management of this uncommon and challenging condition.
The authors have no conflicts of interest to declare.