The burden of cardiovascular disease within the United States is profound, with large volumes of economic and academic resources being utilized to treat patients with cardiovascular diseases. Myocardial infarctions (MI) represent one of the most acute forms of cardiovascular pathology, with a profound mortality rate if prompt treatment and medical attention is not sought out after. While elements of changes in clinical practice and the spurring of new guidelines are responsible for improved health outcomes within year to year, the appraisal of trends in clinical outcomes allows for the scrutiny of methodology in approaching the patient with MI. Moreover, stratification of outcomes based on variables that have been shown to be associated with differential end outcomes in MI, such as age, sex, and type of institution allow for further partitioning of guidelines to meet more specific and tailored decision making guidelines or algorithms. For our dataset, a sampling of MI discharges between the years of 2000 and 2015 using the National Inpatient Sample (NIS), an open-access all-player database that features data on inpatient statistics represented in hospital admissions within institutions that participate within the NIS. Analyses regarding year-to-year length of stay and mortality outcomes of patients by age, sex, and type of institution was performed, showing a decrease in MI discharges, and a statistically significant difference in mean length of stay time at teaching institutions vs. non-teaching hospitals. These results can be compared with contemporary guidelines to assess whether current clinical practice is equipped to address these differential clinical outcomes.
Cardiovascular disease remains the leading cause of death in the United States, with myocardial infarctions representing an acute culmination of cardiovascular disease. According to the American College of Cardiology, an American will have a myocardial infarction roughly every 40 seconds [1]. Despite this grave statistic, trends in myocardial infarction deaths in the United States have decreased markedly over roughly the past two decades, as can be appreciated by a query of Centers of Disease Control and prevention(CDC) Wonder for mentions of myocardial infarction using ICD-9 code entries on death certificates (Figure 1). CDC Wonder is a public health information systems platform that can be digitally accessed and hosts data regarding quantitative datapoints with qualitative features regarding death certificates within the United States [2]. Even more encouraging is not only the notion that myocardial infarction deaths have been trended downwards between 1999 and 2018, but the observation that myocardial deaths as a proportion of total deaths per 100,000 individuals has also decreased as can be appreciated by Figure 2. However, myocardial infarction still represents a significant burden to the providers and institutions seeking to improve cardiovascular health outcomes amongst their populations. The economic impact of myocardial infarction has been estimated to be over $80 billion annually by some studies [3]. Moreover, there is an increase in the volume of patient visits centered around the diagnosis, mitigation, or control of underlying risk factors for myocardial infarction, such as hypertension and Type 2 diabetes mellitus [4-6]. Long-term outcomes of survivors still pose prospective challenges to maintaining adequate cardiovascular health even if mortality is initially thwarted. Mortality may be seen in up to 10% of survivors within the first year after an MI, and up to one-half of all MI patients may experience rehospitalization within this same year time span [7]. To better improve institutional capacities regarding decision making in myocardial infarction encounters, it is prudent to assess the flux of patients with myocardial infarctions. Moreover, insight into discharge trends may help providers better understand the characteristics of patients undergoing discharge. The aim of this project is to assess the progress of the prevention and management of myocardial infarction by using the NIS data.
 Figure 1: Age-adjusted deaths related to myocardial infarctions in the United States between 1999 and 2018.
View Figure 1
Figure 1: Age-adjusted deaths related to myocardial infarctions in the United States between 1999 and 2018.
View Figure 1
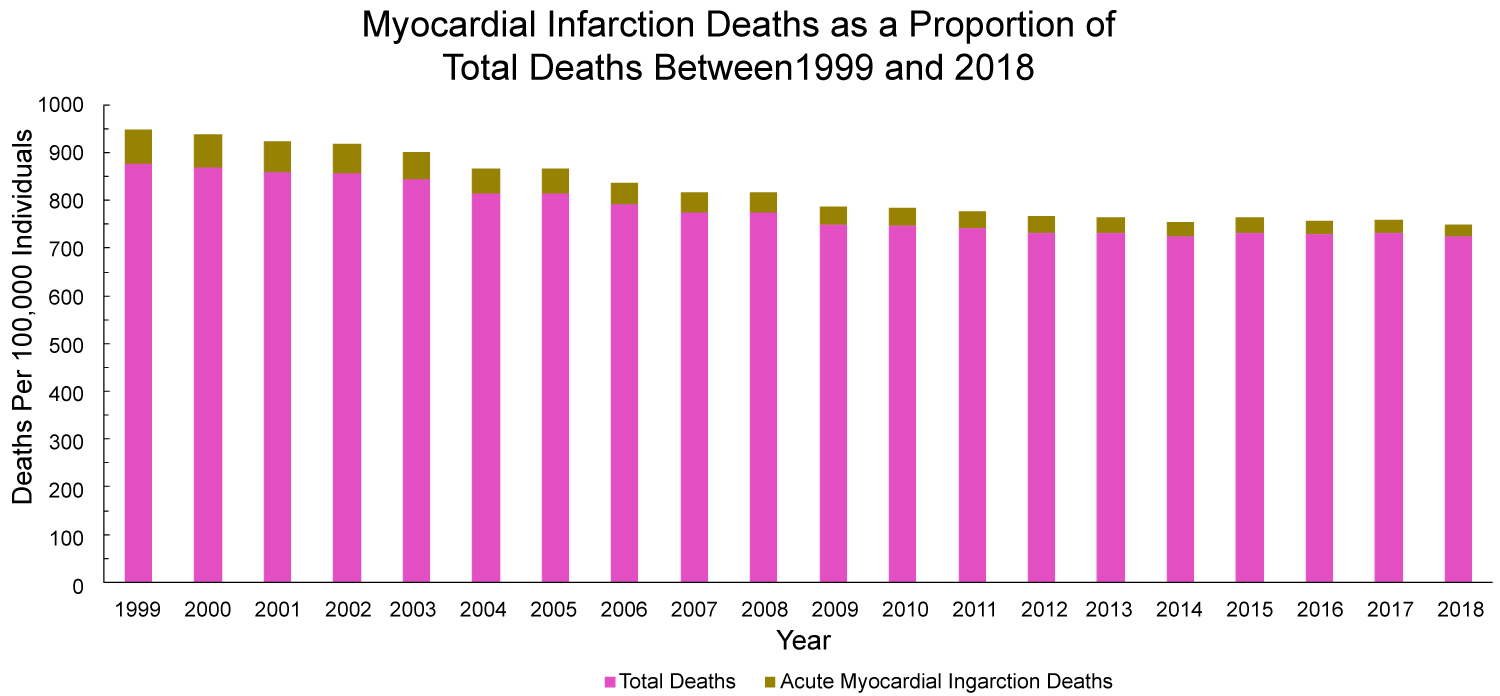 Figure 2: Age-Adjusted deaths related to myocardial infarctions as a proportion of total deaths in the United States between 1999 and 2018.
View Figure 2
Figure 2: Age-Adjusted deaths related to myocardial infarctions as a proportion of total deaths in the United States between 1999 and 2018.
View Figure 2
Data on myocardial infarction presentations to hospitalizations was assessed through a retrospective study utilizing The National Inpatient Sample (NIS) from 2000 through 2015. The NIS is a publicly available all-payer inpatient database that hosts data on hospital admissions for a wide array of clinical diagnoses and sequelae [8]. Myocardial infarction discharges from 2000 to 2015 were identified by using ICD-9 sorted by Clinical Classification Software (CCS). The rate of discharges per 100,000 persons, inpatient mortality, length of stay, and hospital cost were the variables trended. Inpatient mortality was further stratified by gender and by academic hospital status (teaching vs. non-teaching). Z-tests were implemented in order to elucidate statistical differences in the length of stay and mortality rate between teaching and non-teaching hospitals, as well as differences in the percentage of mortality between genders.
The rate of myocardial infarction discharges per 100,000 persons decreased in the years between 2000 and 2015 (Figure 3 and Figure 4). Similarly, inpatient mortality declined in both genders, but the female inpatient mortality rate was significantly higher over the 15-year period (P value < 0.001) (Figure 5). No change was noticed in the mean age for myocardial infarction of either gender over the studied time period (Figure 6). A visualization of the differences between genders and myocardial infarctions can be appreciated in Figure 4. The rates of myocardial infarction for each gender markedly decreases as an overall trend within the time period, however no significant decreases can be appreciated between 2010 and 2015. A comparison of academic and non-academic institutions revealed no significant difference in inpatient mortality rate (P value > 0.05) (Figure 7). A statistically significant difference in length of stay (P-value < 0.001) was noted when correlating differences in hospital cost (Figure 8 and Figure 9). The hospital cost has increased gradually overtime with teaching hospitals cost being higher than the non-teaching hospitals throughout the years of the study.
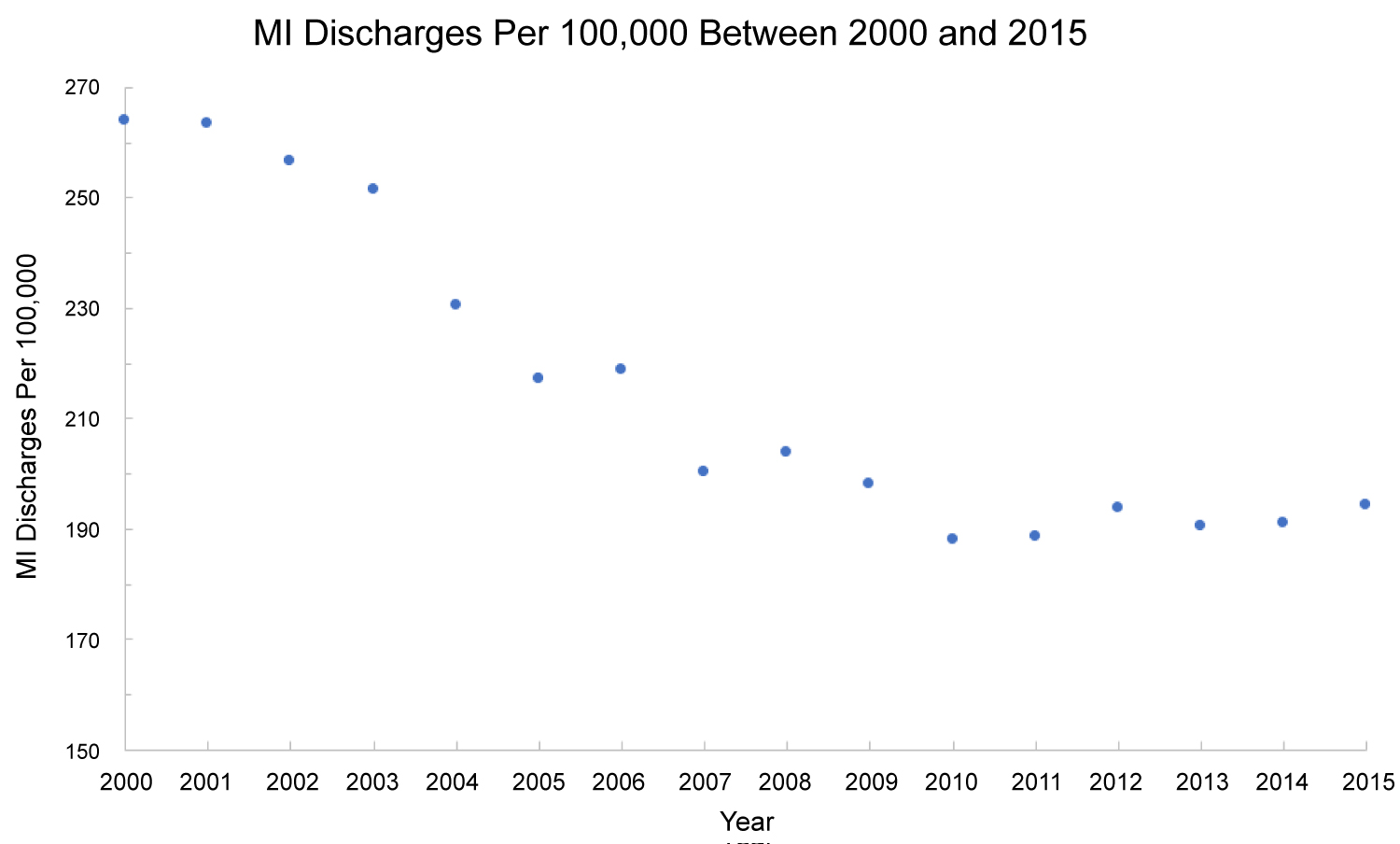 Figure 3: Myocardial infarction discharge rates per 100,000 individuals (aggregate) in the United States between 2000 and 2015.
View Figure 3
Figure 3: Myocardial infarction discharge rates per 100,000 individuals (aggregate) in the United States between 2000 and 2015.
View Figure 3
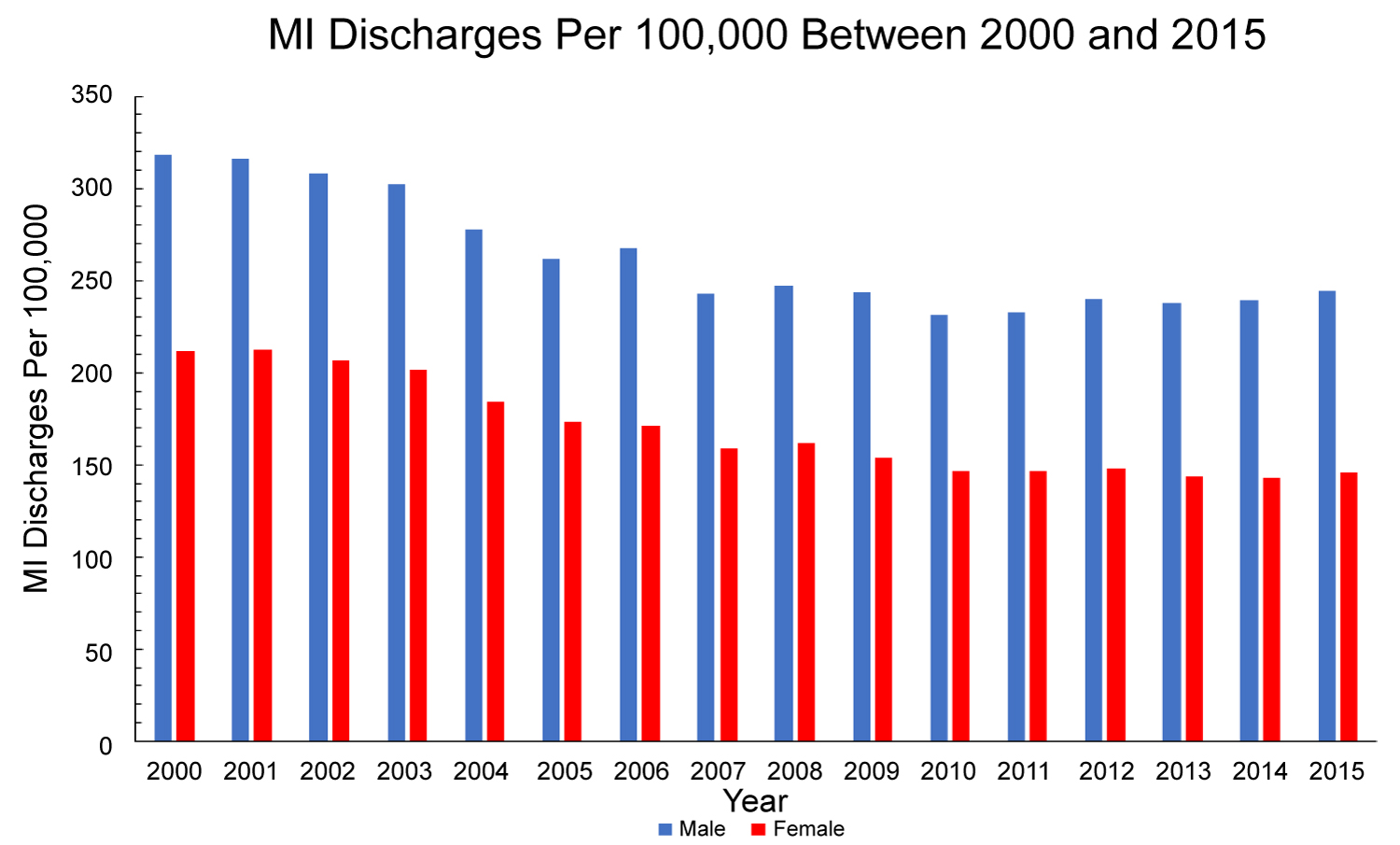 Figure 4: Myocardial infarction discharge rates per 100,000 individuals in the United States between 2000 and 2015 stratified by sex.
View Figure 4
Figure 4: Myocardial infarction discharge rates per 100,000 individuals in the United States between 2000 and 2015 stratified by sex.
View Figure 4
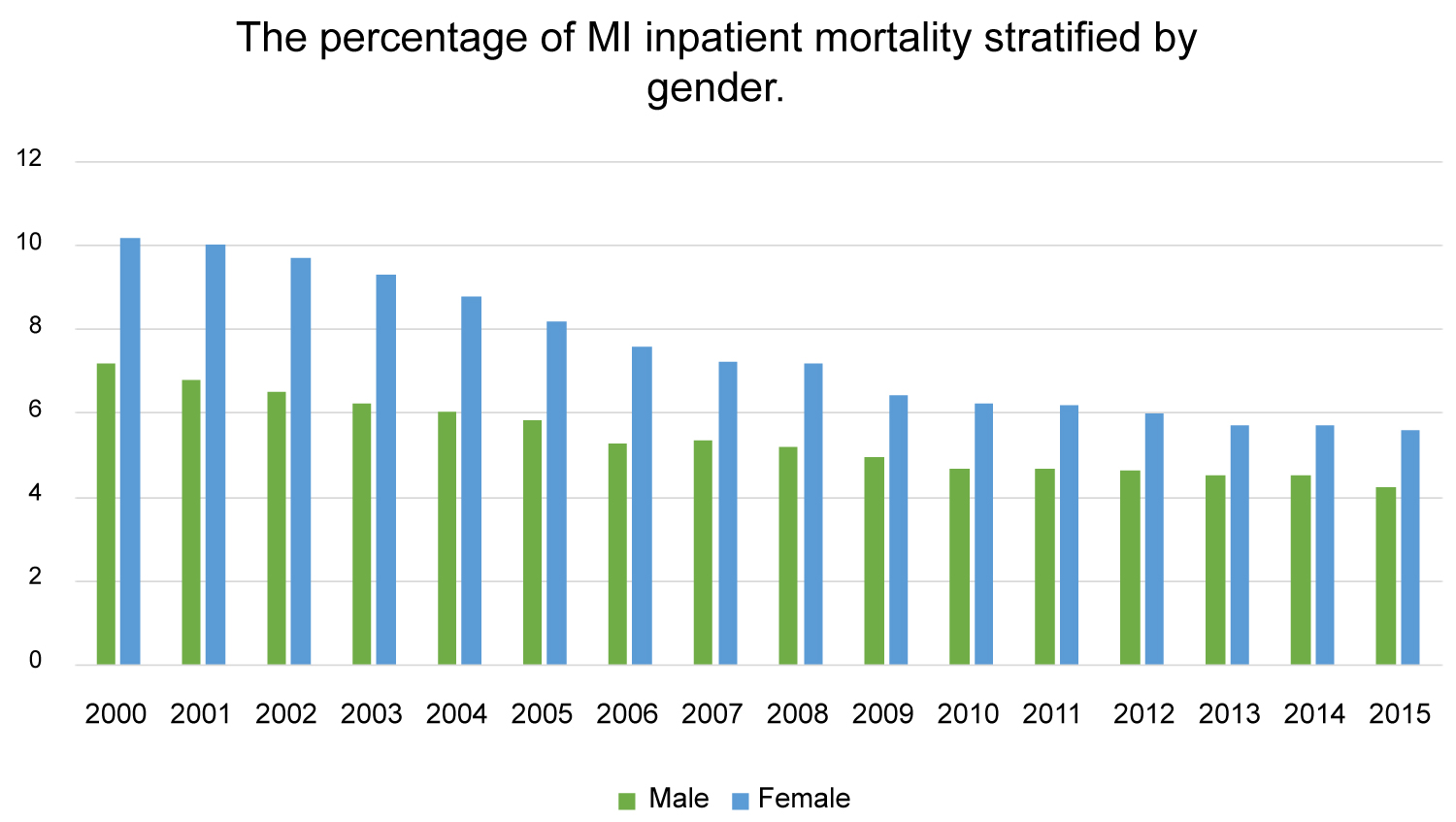 Figure 5: Percentage of myocardial infarction inpatient mortality stratified by gender (P value < 0.001).
View Figure 5
Figure 5: Percentage of myocardial infarction inpatient mortality stratified by gender (P value < 0.001).
View Figure 5
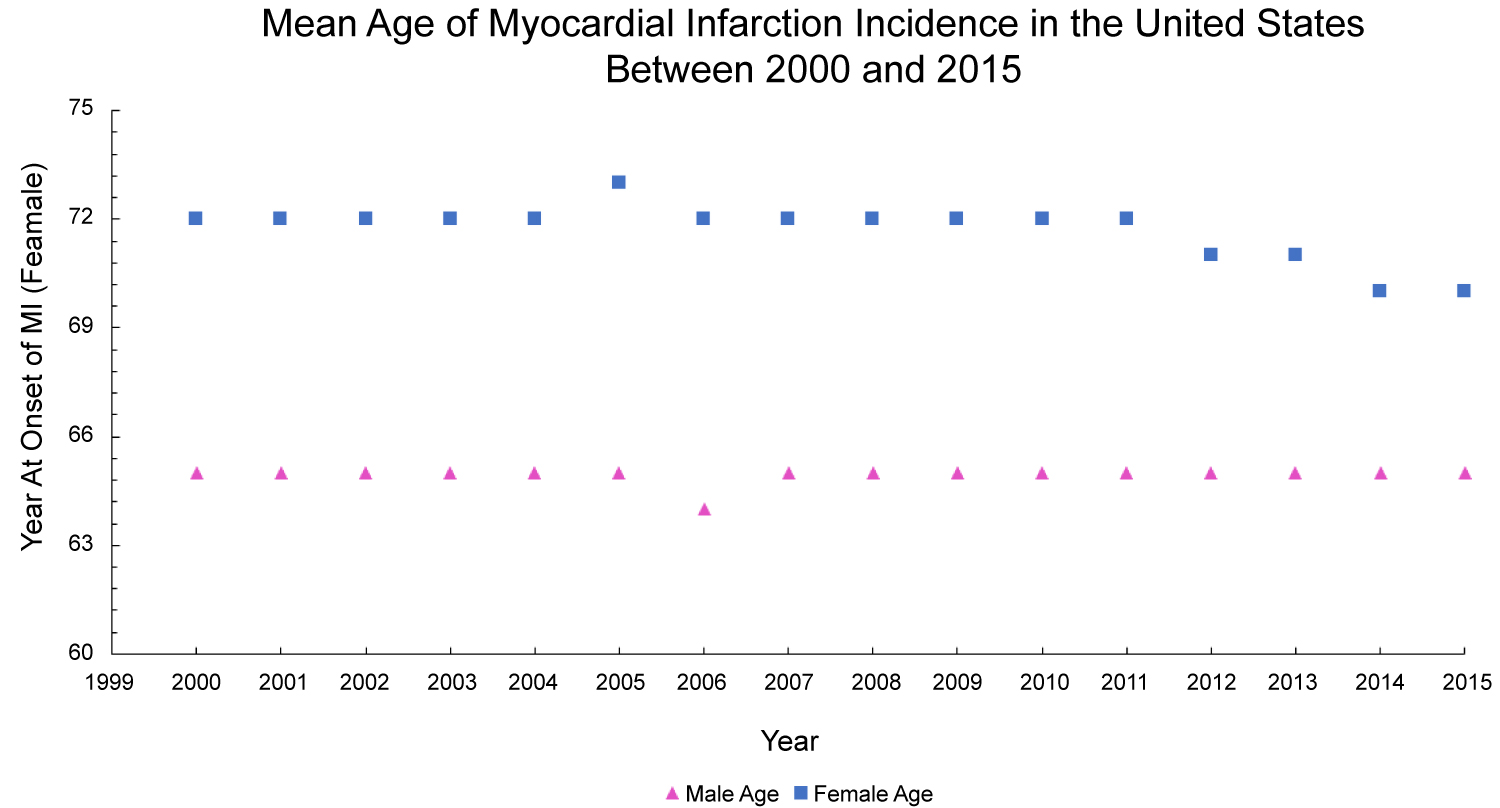 Figure 6: Differences in onset of myocardial infarction by age in the United States between 2000 and 2015.
View Figure 6
Figure 6: Differences in onset of myocardial infarction by age in the United States between 2000 and 2015.
View Figure 6
 Figure 7: Myocardial infarction mortality per 100,000 individuals in the United States between 2000 and 2015 stratified by institutional setting (P value > 0.05).
View Figure 7
Figure 7: Myocardial infarction mortality per 100,000 individuals in the United States between 2000 and 2015 stratified by institutional setting (P value > 0.05).
View Figure 7
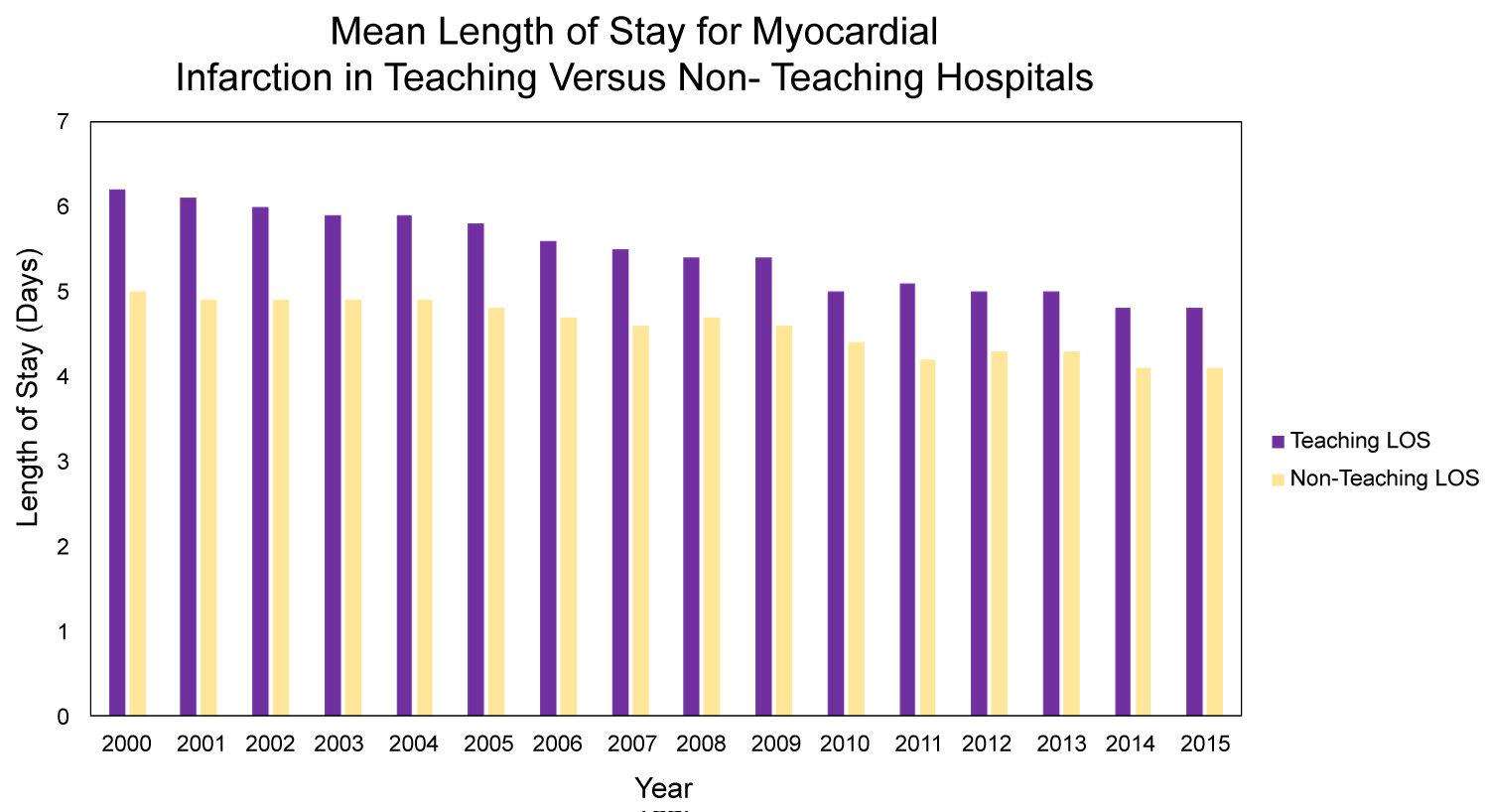 Figure 8: Myocardial infarction length of stay per 100,000 individuals in the United States between 2000 and 2015 stratified by institutional setting (P value < 0.001).
View Figure 8
Figure 8: Myocardial infarction length of stay per 100,000 individuals in the United States between 2000 and 2015 stratified by institutional setting (P value < 0.001).
View Figure 8
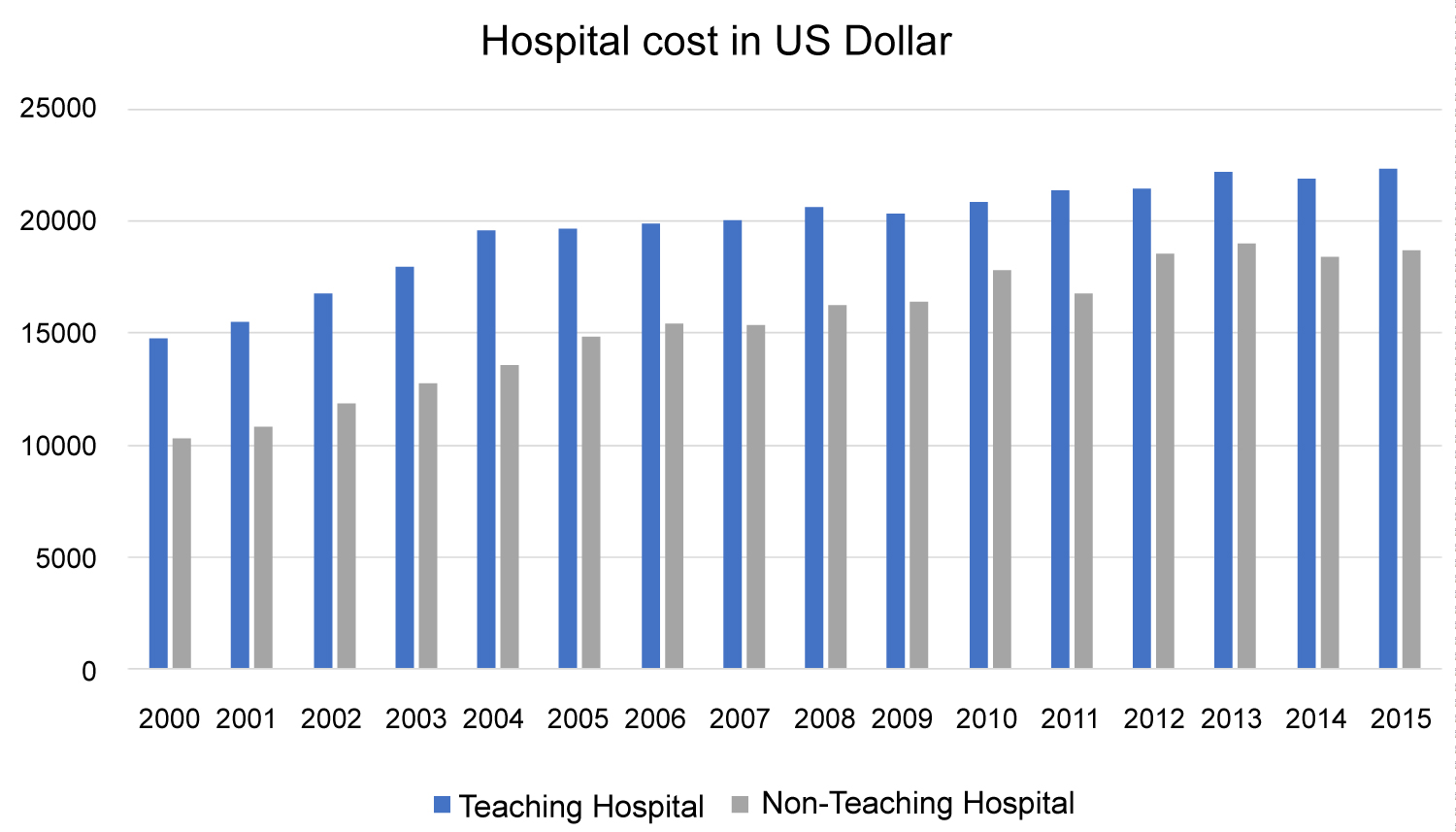 Figure 9: Trend of hospital cost per discharge comparing teaching and non-teaching hospitals.
View Figure 9
Figure 9: Trend of hospital cost per discharge comparing teaching and non-teaching hospitals.
View Figure 9
The decrease in the rate of discharges reflects improvement in preventative measures and the role of primary and secondary prevention. Moreover, decreases in overall inpatient mortality secondary to myocardial infarctions is a testament to innovations in the medical and interventional management of myocardial infarction. However, this improvement in the management has led to a significant increase in hospital costs, and while may not rival the fiscal burden of death related to myocardial infarctions, it still represents an avenue for improvement in providing patients and institutions alike with long-term sustainability when fighting the battle against cardiovascular disease. The length of stay in teaching hospitals is longer than non-teaching hospitals per Figure 8, and the difference is statistically significant (P value < 0.001). However, there was no significant difference in inpatient mortality (P value > 0.05) (Figure 7). Also, there is no change in the mean age for myocardial infarction for either gender throughout the course of this analysis interval, per Figure 6. Female sex status appears to be a non-modifiable risk factor for inpatient mortality. This is consistent with previous literature findings exhibiting a predilection for cardiovascular disease and sex secondary to differences in sex hormones and subsequent physiological differences as a result of these sex hormones which include, but are not limited to, increased hematocrit, lipid metabolism, and modifiability of vasculature [9-15]. While males generally have an increased risk for myocardial infarction and heart disease, studies show that delays in diagnoses are more prominent in women, especially in the setting of lack of chest pain in females presenting with MI that can delay in time to intervention, hence increasing female mortality than that of males. Besides, some studies noticed that the average age of women admitted with MI is higher than that of men which can help explain higher female death rate [16,17]. The notion that women typically present with "atypical" MI symptoms has been recently challenged [18-20]. While this leads to downstream differential changes in hospital experience is yet to be fully elucidated.
In general, the results suggest a trend in more aggressive prevention, medical, and interventional management of myocardial infarction at the expense of increasing hospital costs. Additionally, our analyses may illustrate avenues for improvement at the institutional level in teaching hospitals in terms of reducing length of stay while maintaining similar outcomes in order to decrease hospital costs incurred, in an effort to match the costs of non-teaching hospitals. This phenomenon is also concerning in the context that previous analyses have demonstrated that academic institutions, while offering an increased amount of patient services, may be associated with higher readmission rate for myocardial infarctions [21]. Further goals may be applying the contemporary lessons learned from the NIS data trends in designating how each type of acute myocardial infarction affects patient outcomes and cost (e.g., STEMI vs. NSTEMI), as was done in a similar dataset spanning from 2001 to 2011 [22]. However, it is important to distinguish the populous of patients that arrive in teaching hospitals versus non-teaching hospitals to mitigate covariance that these patients may bring in the admission data for each respective type of institution.
None.