Thrombocytopenia, defined as a platelet count less than 150 × 109/L, has a broad differential of causes and can lead to life threatening complications. We present a case of rapid thrombocytopenia following an Aggrastat (tirofiban) bolus. The platelet count decreased from 195 × 109/L at the time of admission to 18 × 109/L. After discontinuing tirofiban, the platelet count increased to 95 × 109/L within several hours. PF-4 antibody and serotonin release assay testing for potential heparin induced thrombocytopenia were negative. This case highlights the importance of close monitoring of the platelet count with tirofiban administration. Medical professionals should remain aware of causes for acute thrombocytopenia in the coronary care unit and their management.
Tirofiban, Aggrastat, Thrombocytopenia, Percutaneous coronary intervention, NSTEMI
ECG: Electrocardiogram; NSTEMI: Non-ST Segment Elevation Myocardial Infarction; HIT: Heparin Induced Thrombocytopenia; DIT: Drug Induced Thrombocytopenia; DIC: Disseminated Intravascular Coagulation; TTP: Thrombotic Thrombocytopenic Purpura; INR: International Normalized Ratio; SRA: Serotonin Release Assay
A 61-year-old male presented to the emergency department with a two day history of intermittent, burning chest pain which became constant and radiated to the left arm. His past medical history was significant for coronary artery disease with two prior myocardial infarctions, three prior cardiac stenting procedures (in 1999, 2001, and 2006), tobacco use with more than a forty pack year history, hypertension, hyperlipidemia, gastroesophageal reflux, cluster headaches, and an early family history of coronary artery disease. He was visiting from another state and no longer followed with a cardiologist. Home medications included aspirin 81 mg daily, atenolol 25 mg daily, verapamil 120 mg twice a day, omeprazole 20 mg daily, montelukast 10 mg daily, fluoxetine 40 mg daily, and alprazolam as needed.
At the time of initial presentation, he was a febrile and hypertensive with a blood pressure of 187/116 mmHg which improved to 153/94 after administration of nitroglycerin. The physical exam was unremarkable. The initial electrocardiogram (ECG) showed sinus rhythm with a non-specific ST-T wave abnormality. Initial laboratory values included a white blood cell count of 10.2 × 109/L, hemoglobin of 15.2 g/dL, platelet count of 195 × 109/L, troponin I of 0.07 which subsequently increased to 0.24 ng/mL, and myoglobin of 231 ng/mL. Creatinine was 1.07 with a glomerular filtration rate over 60. He had ongoing chest pain, and repeat ECG showed dynamic changes with T-wave inversions in the anterolateral leads. He was diagnosed with NSTEMI, started on a heparin drip per acute coronary syndrome protocol, given aspirin, and brought to the angiography suite.
Coronary angiography revealed an acute 100% occlusion of the mid left circumflex artery, which was reduced to 0% with a 2.5 × 16 mm Synergy drug-eluting stent. In the angiography suite, he received 5000 units of heparin, 180 mg of Brilinta (ticagrelor), 400 mcg nitroglycerin, 100 mcg nitroprusside, a 25 mcg/kg Aggrastat (tirofiban) IV bolus followed by an IV infusion at 0.15 mcg/kg/min, fentanyl, and midazolam. The tirofiban bolus started at 9:10 PM followed by the infusion at 9:16 PM. He tolerated the procedure well and was transferred from the angiography suite to the cardiac intensive care unit for further monitoring.
Post-procedure lab values from 9:17 PM showed a significant, acute decrease in platelets to 18 × 109/L without a decrease in other cell lines. The platelet count was rechecked by microscopy, which confirmed a platelet count of 18 × 109/L at 10:16 PM. The patient did not have any signs of active bleeding, and the reduction in platelet count was discussed with interventional cardiology. After further discussion, the tirofiban infusion was discontinued by 11:22 PM, heparin products were discontinued, and Brilinta was held until the platelets recovered to above 50 × 109/L. Hematology was also contacted for recommendations.
The platelet counts were closely monitored until recovery (Table 1 and Figure 1), and no platelet transfusion was required. The patient reported a headache, so a head CT was obtained and showed no signs of intracranial hemorrhage. The patient's platelet count improved after discontinuing tirofiban, and the hemoglobin remained stable. Brilinta was restarted the following morning, and aspirin was continued. The patient was discharged with a platelet count of 126 × 109/L on hospital day four. Fibrin and fibrinogen fragment testing were normal with a normal international normalized ratio (INR). PF-4 antibody and serotonin release assay (SRA) testing for heparin induced thrombocytopenia returned negative.
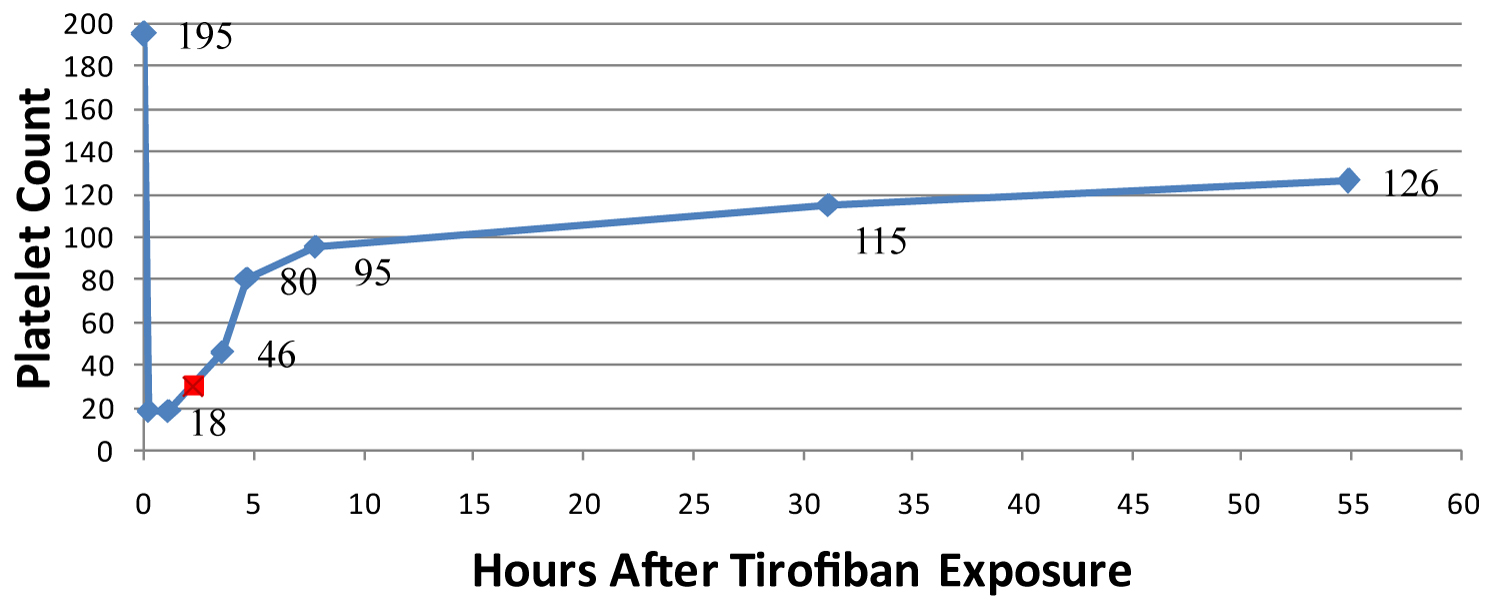 Figure 1: Platelet counts plotted over time after exposure to tirofiban. His initial platelet count was 195 on admission. The tirofiban bolus started at 9:10 PM on the first day of hospitalization (time zero) followed by the tirofiban infusion. The platelet counts at 9:17 PM and 10:16 PM during tirofiban infusion were18 × 109/L. Tirofiban was discontinued at 11:22 PM (red square), and his platelet counts recovered during his hospitalization to 126 × 109/L.
View Figure 1
Figure 1: Platelet counts plotted over time after exposure to tirofiban. His initial platelet count was 195 on admission. The tirofiban bolus started at 9:10 PM on the first day of hospitalization (time zero) followed by the tirofiban infusion. The platelet counts at 9:17 PM and 10:16 PM during tirofiban infusion were18 × 109/L. Tirofiban was discontinued at 11:22 PM (red square), and his platelet counts recovered during his hospitalization to 126 × 109/L.
View Figure 1
Table 1: Results from the patient's complete blood counts from hospital days one through four. The tirofiban bolus started at 9:10 PM on the first day. The 9:17 PM and 10:16 PM lab draws occurred while the patient was receiving tirofiban. Tirofiban was discontinued by 11:22 PM on hospital day one. View Table 1
Our patient developed rapid and profound thrombocytopenia with the platelet count decreasing from 195 × 109/L at the time of admission to 18 × 109/L after exposure to Aggrastat (tirofiban). Aggrastat was discontinued, and his platelet count subsequently recovered to a value above 50 × 109/L within several hours. Although there is no platelet count directly before the tirofiban bolus, we are confident that the initial platelet count is accurate. The platelet count significantly increased after discontinuing tirofiban, and the hemoglobin values remained relatively similar (Table 1). Bougie, et al. proposed that acute thrombocytopenia after tirofiban or eptifibatide is related to drug-dependent antibodies [1]. Our patient has a history of cardiac stents and may have been previously exposed to tirofiban. Antibodies from a possible prior tirofiban exposure could explain the rapid decrease in platelet counts as seen in this case.
Tirofiban is an antagonist of the platelet glycoprotein IIb/IIIa receptor, which inhibits platelet aggregation [2]. Clinical trials demonstrating benefit of tirofiban include PRISM for unstable angina [3], PRISM-PLUS for unstable angina and non-Q wave myocardial infarction [4], and ADVANCE for high risk percutaneous intervention [5]. Recommended dosing for Aggrastat per the manufacturer is a 25 mcg/kg bolus within five minutes followed by 0.15 mcg/kg/min for up to eighteen hours [2]. At this dosing, more than ninety percent inhibition of platelet aggregation is achieved within ten minutes [2]. Bleeding is the most common complication, and platelet inhibition is reversible after the discontinuation of Aggrastat [2]. Contraindications listed by the manufacturer include severe hypersensitivity reactions, a history of thrombocytopenia following prior exposure, active internal bleeding, and major surgical procedures or physical trauma in the past month [2].
Glycoprotein IIb/IIIa inhibitors can cause drug induced thrombocytopenia, and previous case reports have been published [6-10]. Platelet counts less than 100 × 109/L occurred in 1.1 to 1.9% of patients in clinical trials of tirofiban, and counts less than 50 × 109/L occurred in 0.2% to 0.5% of patients [11]. Thrombocytopenia typically occurs within twenty-four hours but can occasionally occur within thirty minutes to several hours [6]. These case reports did not document a platelet count shortly after the initiation of tirofiban, so it is unknown how quickly the platelet count can decrease. In our case, a decreased platelet count was detected minutes after starting tirofiban with an acute fall in platelet counts from 195 × 109/L to 18 × 109/L. Within several hours after discontinuing tirofiban, the platelet count increased to 95 × 109/L and gradually recovered to 126 × 109/L before hospital discharge. Thrombocytopenia secondary to tirofiban is thought to be related to drug-dependent antibodies that cause platelet destruction [11,12]. The antibodies can naturally occur before exposure or are induced by prior exposure to the drug [1].
Patients in the angiography suite are exposed to medications which may cause thrombocytopenia. HIT was initially considered because of the patient's exposure to heparin and acute thrombocytopenia. Type 1 HIT is a non-immune, mild reaction from the direct effects of heparin on platelet activation [13]. Type 2 HIT is immune mediated with the development of antibodies and thrombotic complications [13]. The 4Ts scoring system can be used to predict the probability of HIT, and treatment includes non-heparin anticoagulation and discontinuing all heparin products [13]. The serotonin release assay and PF4 antibody testing for HIT were both negative in our patient. Other causes for thrombocytopenia were also considered.
Disseminated intravascular coagulation (DIC) involves thrombocytopenia, schistocytes, and systemic activation of the coagulation system [14]. The PT and a PTT are prolonged from coagulation factor consumption, fibrinogen is low, and the D-dimer is elevated [14]. Our patient's lab values for fibrinogen and fibrinogen degradation products were within normal limits. Thrombotic thrombocytopenic purpura (TTP) is rare and has five typical features: Micro-angiopathic hemolytic anemia, thrombocytopenia, neurologic symptoms, fever, and renal dysfunction [14]. Our patient had thrombocytopenia but none of the other characteristic findings.
Pseudothrombocytopenia is a laboratory artifact that results in a falsely low platelet count [14]. The platelets clump when exposed to EDTA in vitro [14]. There was no evidence of platelet clumping upon review of the peripheral blood smear by the hematologist. After evaluation for other possible causes for thrombocytopenia, our patient's presentation is most consistent with thrombocytopenia from tirofiban.
Patients in the coronary care unit and angiography suite can be exposed to medications which may result in acute thrombocytopenia. In our case, the patient developed rapid thrombocytopenia minutes after receiving a tirofiban bolus dose, and the platelet count improved several hours after discontinuing tirofiban. Based on the timeline of events, rapid development of thrombocytopenia, and negative work-up for other potential causes, our patient's presentation is most consistent with thrombocytopenia associated with tirofiban. Patients who receive tirofiban should have close monitoring of their platelet count. If thrombocytopenia occurs, tirofiban can be discontinued with recovery of the platelet count. Future use of tirofiban with a history of thrombocytopenia on exposure should subsequently be considered contraindicated.
All authors declare that there are no conflicts of interest.
None.
None.
All authors' had equal contribution.