Pulmonary arteriovenous malformations are commonly treated by embolization with coils or balloons to prevent cerebral complications and to raise the oxygenation of the blood. The Cera vascular plug (Lifetech Scientific, Shenzhen, China) is a new vascular device made of a self-expanding cylindrical nitinol mesh. Here we report a case of a 13-year-old boy who had presented with 4 year history of progressive exertional dyspnoea, cyanosis, and clubbing. Pulmonary arterio-venous malformation (multiple) was diagnosed which was arising from right pulmonary artery. Complete occlusion was achieved using two 12 mm Cera vascular plug, thereby reversing the cyanosis on catheterization table. On follow up at 9 months, clubbing also disappeared.
Pulmonary arteriovenous malformations, Cera vascular plug, Cyanosis, Clubbing
Pulmonary arteriovenous malformations (PAVM) are abnormal communications between the pulmonary arteries and veins without any intervening capillary beds. Most of them are syndromic (70-95%), seen in association with hereditary hemorrhagic telangiectasia (Osler-Weber Rendu-syndrome), characterized by recurrent epistaxis, mucocutaneous telangiectasia and visceral vascular involvement [1,2]. The sporadic types of PAVM are rare arteriovenous communications that may develop in virtually any organ and especially in the lungs. These may complicate into cyanosis, dyspnoea, massive haemoptysis, haemothorax, as well as neurologic complications, including transient ischemic attack, cerebral stroke and cerebral abscess due to the right-to-left shunting that facilitates the passage of septic emboli into the cerebral circulation [1]. Thus these warrant treatment treating even for asymptomatic one if technically feasible. These can be treated percutaneously by transcatheter embolization, using detachable balloons, coils, and vascular plugs [3]. Most of their closure have been reported using Amplatzer vascular plug [4,5]. Cera vascular plug (Lifetech Scientific, Shenzhen, China) is a relatively new device which has been used quite recently in few cases for arterial and venous embolization [6]. Simple investigation like contrast echocardiogram using agitated saline can be used to conclusively identify pulmonary AVMs. When treating pulmonary AVMs, embolization with arterio-venous plug (AVP) is a less time consuming and safe method [7].
A 13-year-old boy presented with 4 years history of progressive exertional dyspnoea. There was no history of squatting, cyanotic spells, recurrent lower respiratory tract infection, epistaxis and bleeding per rectum. There was no family history of bleeding disorders. Clinical examination showed central cyanosis (oxygen saturation- 89%), pan-digital clubbing, normal heart sounds and silent precordium. There was a short systolic bruit audible in right infra axillary area which was getting intensified with deep inspiration. Electrocardiogram was normal. Chest X-ray showed a homogenous opacity in the right lower zone (Figure 1). Trans-thoracic echocardiogram was otherwise normal. Contrast echocardiogram revealed dense opacification of left atrium and consequently left ventricle after 4 cardiac cycles following appearance of contrast in the right heart chambers on administering agitated saline contrast. Based on above findings, it was diagnosed as sporadic pulmonary AVM. Cardiac catheterization was done using 6F multipurpose catheter (MP) which was advanced into right pulmonary artery (RPA) showing two arterio-venous fistula which had restrictive diameter of 8.5 mm along the length of AVM (Figure 2).
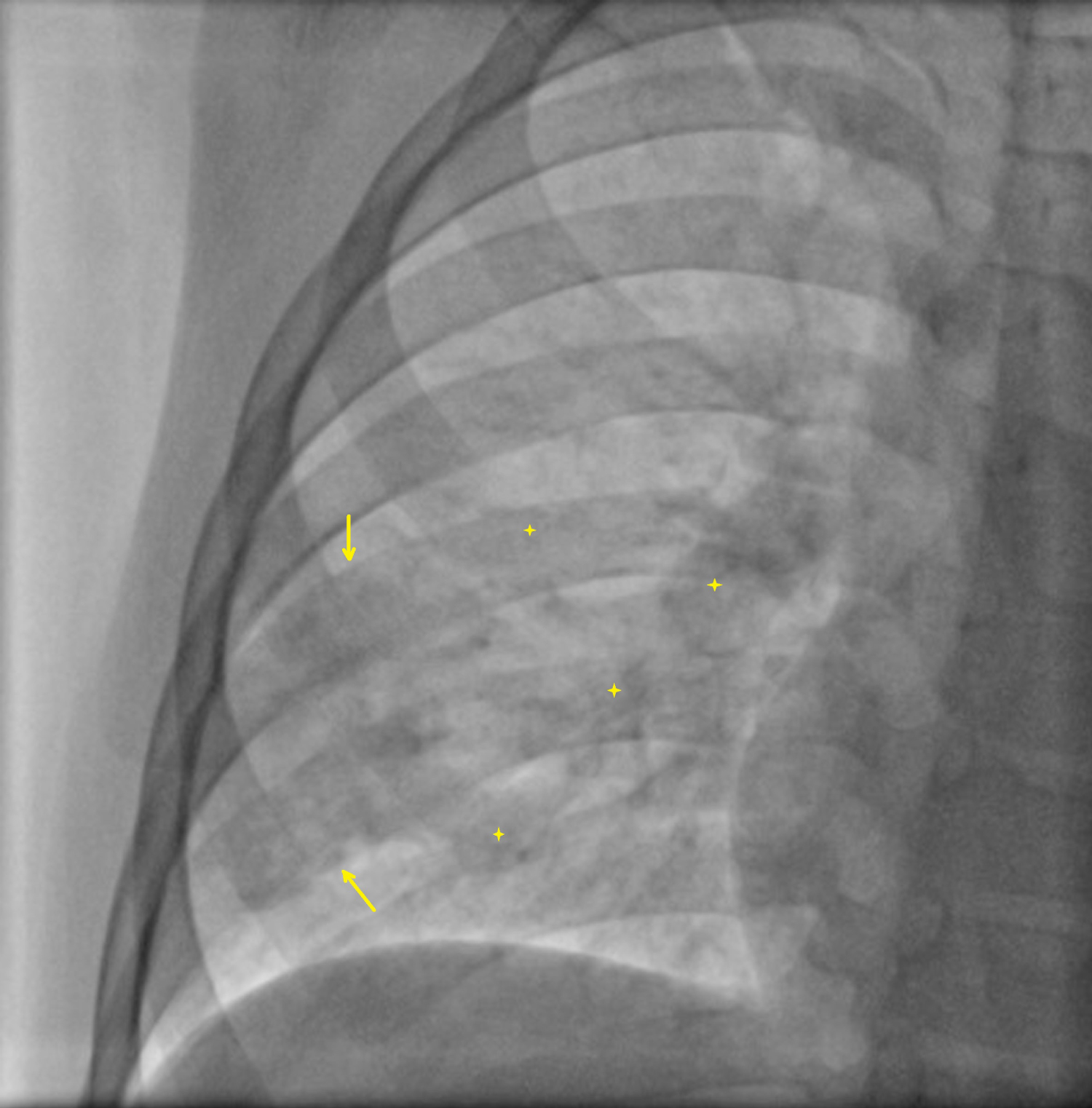 Figure 1: Chest X-ray showed a homogenous opacity in the right lower zone (yellow arrow and stars).
View Figure 1
Figure 1: Chest X-ray showed a homogenous opacity in the right lower zone (yellow arrow and stars).
View Figure 1
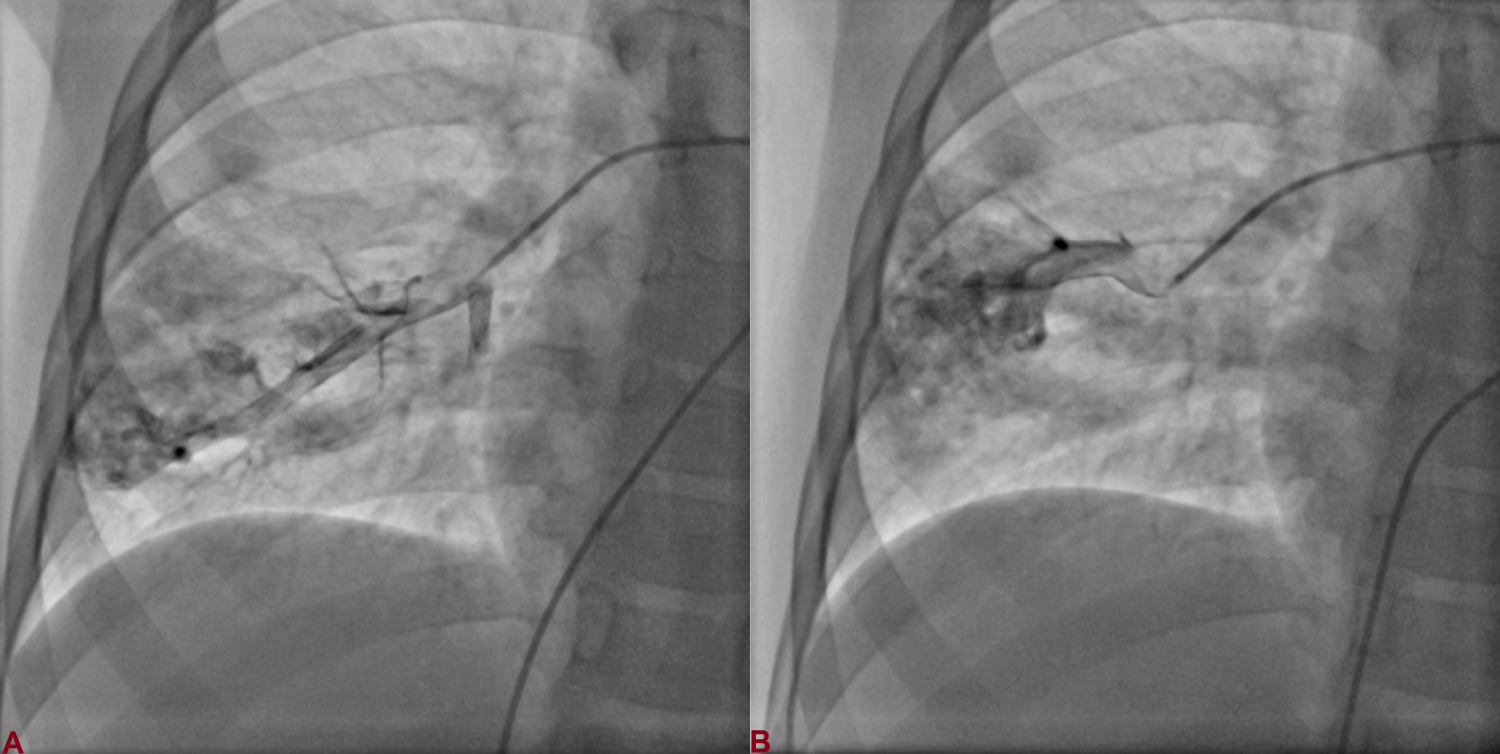 Figure 2: Cardiac catheterization revealed two arteriovenous fistulas arising from right pulmonary artery.
View Figure 2
Figure 2: Cardiac catheterization revealed two arteriovenous fistulas arising from right pulmonary artery.
View Figure 2
Percutaneous device closure of AVM was planned after taking written informed consent from his parents and approval from institutional review board regarding the usage of the device. Few of the large AVM had already been closed using Amplatz vascular plug and septal duct occluder at our centre but this was the first one with Cera vascular plug. 6F venous sheath was exchanged with 9F sheath. 6F MP catheter was parked into RPA over 0.35 inch Terumo wire (Terumo, Japan). Wire was exchanged with another super-stiff and long (0.035", 260 cm) terumo wire. Keeping wire into lower RPA, multipurpose catheter was exchanged with 9F Cook delivery sheath (Cook Medical, USA). After repeated de-airing the vascular plug by immersing into saline, it was screwed over the delivery cable by clockwise rotation. It is recommended that a device is chosen that is at least 30-50% larger than the size of the native vessel. Therefore, 12 mm Cera vascular plug (Figure 3) was introduced through sheath using a loader and deployed in lower division of RPA by unscrewing it in counter-clockwise direction (Figure 4). Repeat angiogram was done to check position of first plug and to assess landing zone of second plug (Figure 5A). Another 12 mm vascular plug was positioned (Figure 5B) and deployed in similar fashion adjacent to first one to occlude the remaining feeder (Figure 6A). Angiogram, obtained after 10 min of deployment, demonstrated complete closure feeders of both AVMs and perfectly placed plugs (Figure 6B). His oxygen saturation (SpO2) improved to 98%, thereby reversing the cyanosis on catheterization table. On follow up at 9 months, clubbing had disappeared (Figure 7).
 Figure 3: Cera vascular plug with delivery cable.
View Figure 3
Figure 3: Cera vascular plug with delivery cable.
View Figure 3
 Figure 4: A) A 12 mm vascular plug was introduced through the sheath and positioned in the lower division of RPA; B) Deployed by unscrewing in counter-clockwise rotation.
View Figure 4
Figure 4: A) A 12 mm vascular plug was introduced through the sheath and positioned in the lower division of RPA; B) Deployed by unscrewing in counter-clockwise rotation.
View Figure 4
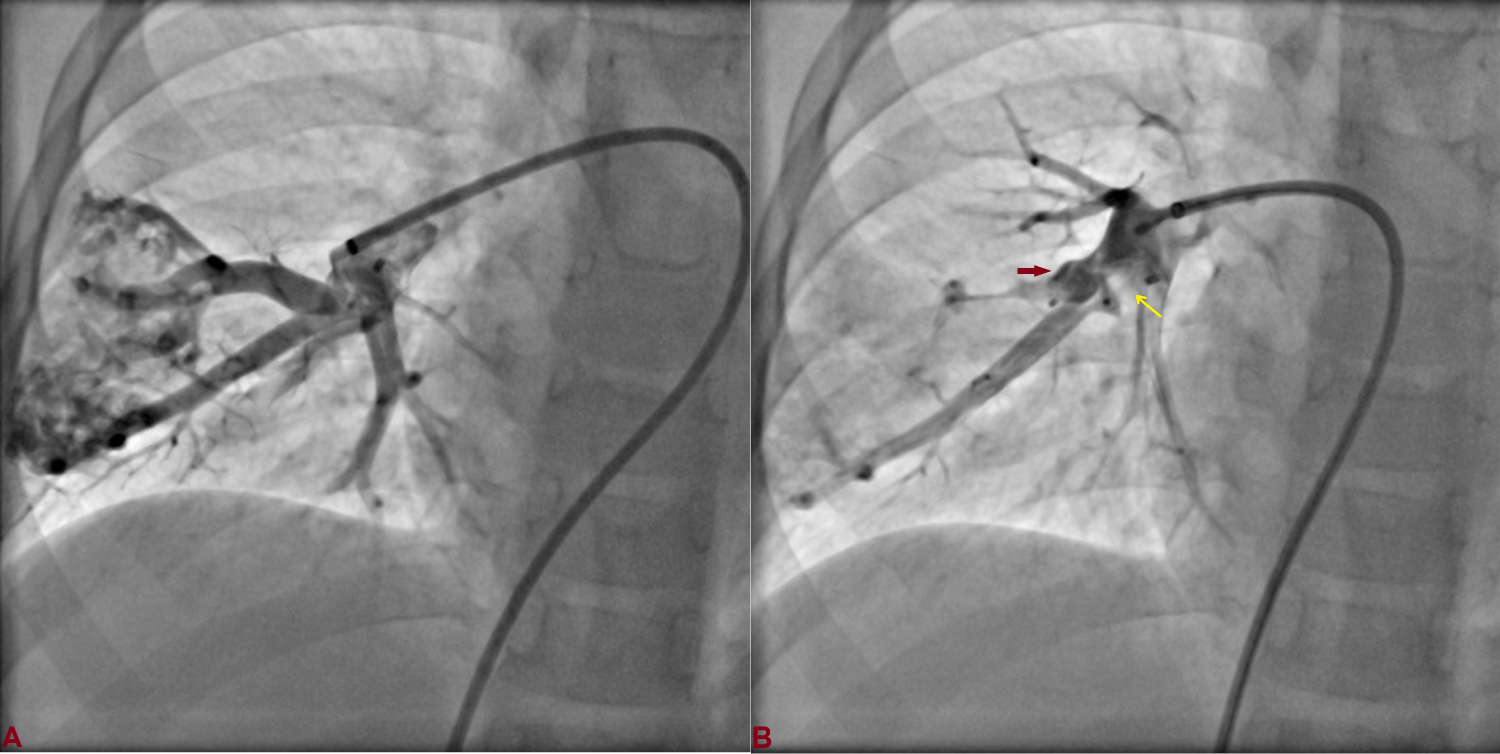 Figure 5: A) Repeat angiogram showing neck of second AVM; B) The second plug (red arrow) was positioned adjacent to first plug (yellow arrow).
View Figure 5
Figure 5: A) Repeat angiogram showing neck of second AVM; B) The second plug (red arrow) was positioned adjacent to first plug (yellow arrow).
View Figure 5
 Figure 6: A) Second plug was deployed; B) Final angiogram, obtained after 10 min of deployment, demonstrated complete occlusion of both AVM and perfectly placed plugs.
View Figure 6
Figure 6: A) Second plug was deployed; B) Final angiogram, obtained after 10 min of deployment, demonstrated complete occlusion of both AVM and perfectly placed plugs.
View Figure 6
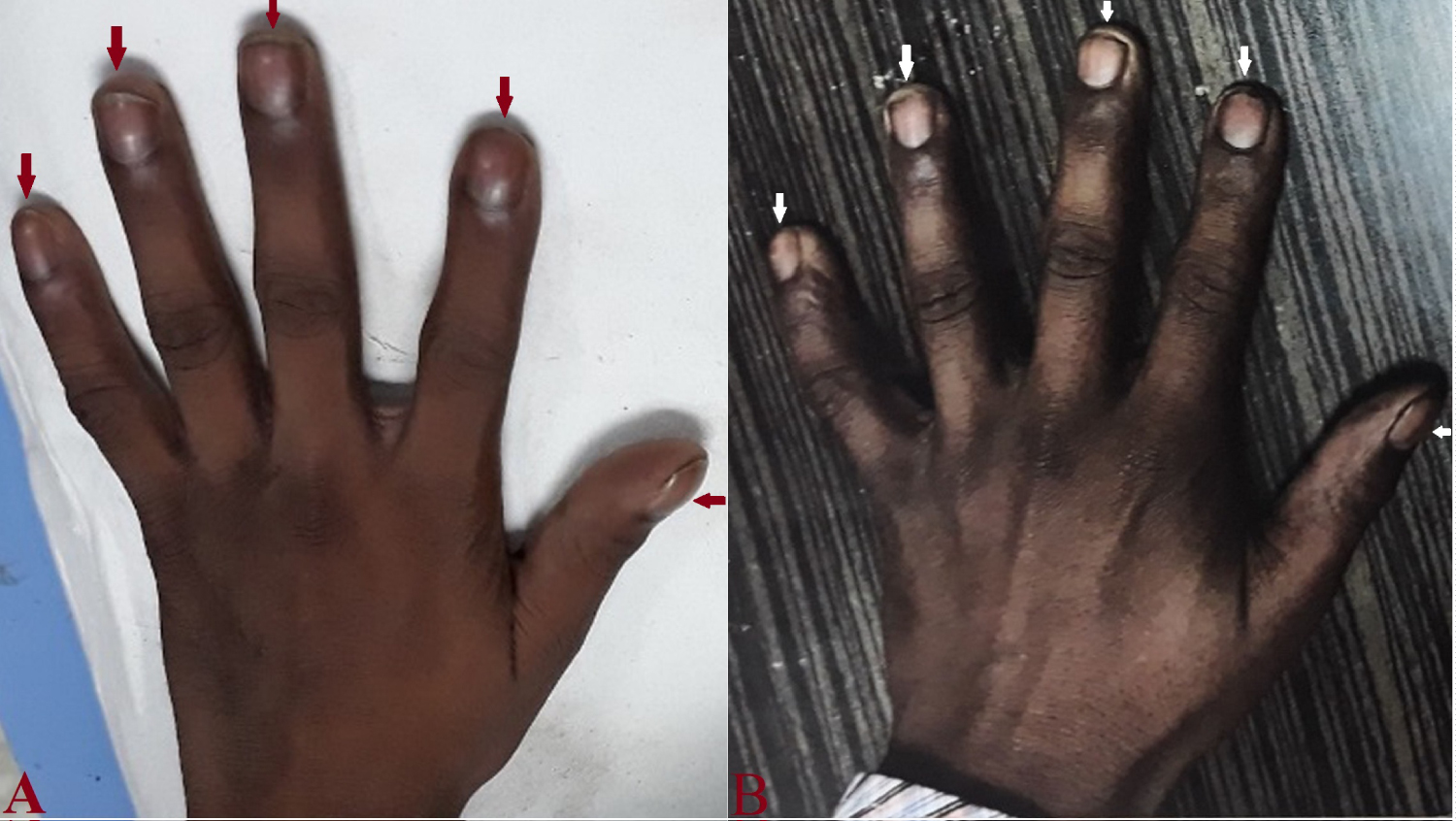 Figure 7: A) Clubbing of fingers (red arrow) in right hand on presentation; B) Complete reversal of clubbing at follow up at 9-months.
View Figure 7
Figure 7: A) Clubbing of fingers (red arrow) in right hand on presentation; B) Complete reversal of clubbing at follow up at 9-months.
View Figure 7
Right-to-left shunt due to pulmonary arteriovenous malformation is usually well tolerated. Dyspnoea is the most common symptom and clinical presentation depends on the number and size of PAVM. The most sinister sequlae are paradoxical embolism and cerebral abscess due to unobstructed passage of bacteria and thrombi through the AVM [5]. The plug size is decided according to the narrowest diameter of neck, vessel length and landing zone [6]. Vascular plugs are ideally suited to embolized vessels with high flow, which can be achieved using single plug which would otherwise have required multiple coils, thus making it efficient and cost-effective. It also cuts down procedure time, cost, and radiation exposure.
Cera™ vascular plug is a new device manufactured by Lifetech (Lifetech Scientific Corp., China). It is a self-expandable cylindrical nitinol wire-mesh occlusion device with ceramic coating [4,8]. Titanium Nitride coating prevents thrombosis and improves endothelialisation. It has a single lobe and multi-layered nitinol mesh makes the plug faster to occlude [9]. It has a lower recanalization rates and negligible risk of device embolization. Micro screw connection helps in its easy and precise placement. The delivery wire in the vascular plug is more flexible, which makes delivery easier and safer [9]. Accurate placement even in large high flowing vascular structures can be readily achieved with Cera vascular plug compared to coils [9]. The size and the shape of the vascular plug provide radial strength and stable adhesion to the vessel wall and over sizing of the plug also contributes toward preventing migration after deployment [10].
None.
None.
All authors made equal contribution.