Hypertrabeculation may be a dominant feature in the cardiac imaging of a newly diagnosed dilated non-ischaemic cardiomyopathy, highly suggestive of primary non-compaction cardiomyopathy. It does not necessarily exclude alternative pathologies however, and it is important to utilise a multimodal cardiac imaging approach even when these features are present on index echocardiographic imaging. The distinction between primary non-compaction cardiomyopathy and an alternative diagnosis such as cardiac sarcoidosis proved important in the consideration in our case for choice of device therapy for primary prevention of ventricular arrhythmias and highlights the importance of a multi-imaging modality approach to the work up of non-ischaemic cardiomyopathies.
A 34-year-old previously well woman presented for outpatient cardiology assessment with a four-week history of increasing exertional dyspnoea, palpitations and atypical chest pain. She presented on only the oral contraceptive pill. She had completed an uncomplicated pregnancy with vaginal delivery at term 10 years previously. She was an ex-smoker, drank no alcohol and had no history of recreational drug use. She had no family history of significant cardiac disease or sudden cardiac death. Originally assessed in our emergency department, a CT pulmonary angiogram was arranged demonstrating no pulmonary emboli, no parenchymal pathology, however, bilateral prominent mediastinal lymph nodes of uncertain significance. She was referred for further assessment in the outpatient setting.
On follow-up, she examined well with no features of decompensated cardiac failure. Her electrocardiograph was benign with no evidence of conduction disease. A transthoracic echo revealed an unexpected finding of a moderately dilated left ventricle with severe left ventricular dysfunction (ejection fraction 20%) and prominent apical trabeculations (Figure 1a and Video 1). She was referred for inpatient cardiology assessment, at which point a contrast transthoracic echocardiogram confirmed severe left ventricular dysfunction with a thinned mid to distal inferoseptum and hinge point (Figure 1b and Video 2). Prominent trabeculations were again noted in the apical and lateral left ventricular segments. She proceeded to have a cardiac MRI which fulfilled the diagnostic criteria for non-compaction cardiomyopathy of 2.3:1 in several segments (Figure 1c). Additionally and unexpectedly however, the cardiac MRI demonstrated gross transmural late gadolinium enhancement in a non-vascular distribution in the mid to distal inferoseptum, raising the possibility of alternative diagnoses including myocarditis and cardiac sarcoid (Figure 1d). Her troponins and inflammatory markers were negative on serial measurement throughout admission. Given her mediastinal lymph node prominence, a cardiac PET scan was arranged which demonstrated no features of active cardiac or systemic sarcoidosis (Figure 1e). Her serum ACE level was negative, as was the remainder of her infiltrative screen. CT coronary angiography was completed given her ongoing atypical chest pain and segmental wall motion abnormality and was negative for coronary artery disease, with features again supportive of a non-compaction cardiomyopathy (Figure 1f). No mediastinal lymph nodes were amenable to endobronchial ultrasound guided biopsy, and given the inactivity on PET, as well as only a focal pathologic segment on MRI, a cardiac biopsy was not pursued.
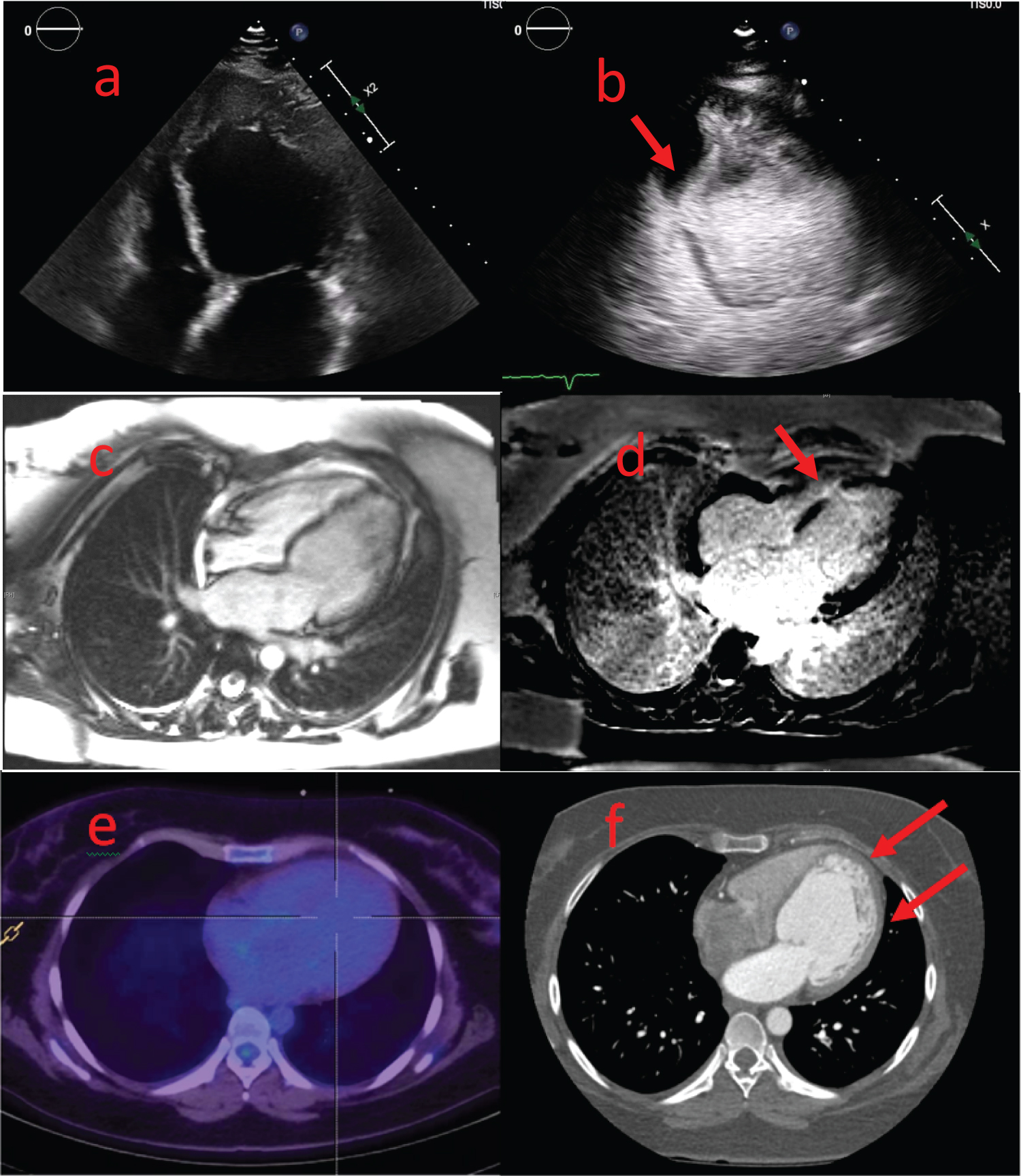 Figure 1: (a) Transthoracic echo four chamber view demonstrating prominent apical trabeculations; (b) Contrast transthoracic echo four chamber view demonstrating prominent apical and lateral wall trabeculations with focal wall motion abnormality at the mid inferoseptum (Red arrow); (c) Axial view of cMRI scan demonstrating a moderately dilated left ventricular with prominent trabeculations apically and laterally, fulfilling cMRI criteria for left ventricular non-compaction; (d) Axial cMRI view with marked late gadolinium enhancement in a non-vascular distribution in the mid to distal inferoseptum (Red arrow); (e) Axial cardiac PET scan with no abnormal uptake globally or in the distribution of the cMRI late gadolinium findings; (f) CTCA with no focal coronary artery disease detected, and again demonstrating prominent apical and lateral wall trabeculations with a normal appearance of the inferoseptal left ventricular wall.
Figure 1: (a) Transthoracic echo four chamber view demonstrating prominent apical trabeculations; (b) Contrast transthoracic echo four chamber view demonstrating prominent apical and lateral wall trabeculations with focal wall motion abnormality at the mid inferoseptum (Red arrow); (c) Axial view of cMRI scan demonstrating a moderately dilated left ventricular with prominent trabeculations apically and laterally, fulfilling cMRI criteria for left ventricular non-compaction; (d) Axial cMRI view with marked late gadolinium enhancement in a non-vascular distribution in the mid to distal inferoseptum (Red arrow); (e) Axial cardiac PET scan with no abnormal uptake globally or in the distribution of the cMRI late gadolinium findings; (f) CTCA with no focal coronary artery disease detected, and again demonstrating prominent apical and lateral wall trabeculations with a normal appearance of the inferoseptal left ventricular wall.
cMRI: Cardiac Magnetic Resonance Imaging; PET: Positron Emission Tomography; CTCA: Computed Tomography Coronary Angiogram
View Figure 1
Video 1: Transthoracic echo four chamber view demonstrating prominent apical trabeculations. View Video 1
Video 2: Contrast transthoracic echo four chamber view demonstrating prominent apical and lateral wall trabeculations with focal wall motion abnormality at the mid inferoseptum. View Video 2
During her inpatient admission, she recorded multiple episodes of symptomatic non-sustained ventricular tachycardia without haemodynamic compromise. She was established on appropriate guideline supported heart failure therapy, and a decision for an upfront automated implantable cardiac defibrillator was made. Although the likely diagnosis of non-compaction cardiomyopathy was established, the septal late gadolinium enhancement raised a possibility of an alternate infiltrative diagnosis. For this reason, a transvenous defibrillating system was recommended over subcutaneous system in the event of developing conduction abnormality.
While late gadolinium enhancement on cardiac MRI is a well-established feature of cardiac sarcoidosis, it is not typical of the congenital syndrome of non-compaction cardiomyopathy [1]. A single case report of apical hypertrabeculation with active cardiac sarcoidosis has been described with little other literature supporting an association between the two rare conditions [2]. In establishing the diagnostic criteria for non-compaction cardiomyopathy on both echocardiography and MRI, authors have attempted to introduce quantitative criteria for differentiating left ventricular non-compaction from other dilated cardiomyopathies. The use of a trabeculated ventricular mass criteria greater than 20-25% of the global LV mass has been suggested as a more specific method, however, again has had limitations due to the overestimation of trabeculated mass secondary to inclusion of intertrabecular blood volume [3,4].
Although diagnostic criteria for non-compaction may be met at index imaging, a multi-modality approach including cMRI and cardiac PET remains essential to consider given a potential for alternative reversible pathology such as active sarcoidosis. Our lady, while meeting a compacted to non-compacted ratio for non-compaction cardiomyopathy, has features to suggest a secondary pathology such as 'burnt out' cardiac sarcoidosis. These distinctions in diagnosis are particularly important to consider in a new diagnosis of a dilated cardiomyopathy so as to ensure all appropriate treatment options can be offered.
We have no conflicts of interest or funding contributions to disclose.
I can confirm that all authors contributed equally to this submission.