Emergency percutaneous coronary intervention (PCI) is a critically important reperfusion strategy for myocardial salvage in the event of acute ST elevation myocardial infarction (STEMI). However, it poses great challenges to the treating cardiologist if there is a simultaneous acute cerebral infarction because of potential intracranial complications. Particularly, the use of dual antiplatelet and high dose anticoagulants during PCI has been well documented to increase the risk for cerebral hemorrhagic conversion in the setting of acute ischemic stroke.
We hereby present three illustrative cases of "hyperacute simultaneous cardiocerebral infarction" that underwent emergency percutaneous coronary intervention due to cardiac hemodynamic instability.
Cardiocerebral infarction, ST elevation myocardial infarction, Percutaneous coronary intervention, Intracranial hemorrhage, Hemorrhagic conversion
This case series illustrates the efficacy and safety of primary percutaneous coronary intervention in improving the cardiovascular outcome without significant risk of intracranial complication among STEMI patients with simultaneous acute ischemic stroke.
Concurrent cardio-cerebral infarction (CCI), a term introduced by Omar, et al. in 2010 [1], is a rare but devastating clinical scenario. Both acute ST elevation myocardial infarction (STEMI) and acute ischemic stroke (AIS) are emergency life threatening conditions with narrow therapeutic time windows. The medical treatment decision is complex when they happen simultaneously as there is no clear guideline recommended management. The initial treatment of one condition will inevitably delay the other.
In the event of ST elevation myocardial infarction (STEMI) with clear evidence of cardiac instability, percutaneous coronary intervention usually takes precedence. However, the cardiology team is often hesitant due to the well-known risk of haemorrhagic conversion of acute ischemic brain tissue associated with the use of antiplatelets and high dose heparin. Therefore, early therapeutic rescue of the heart could potentially lead to harmful neurological outcome.
In this paper, we present 3 CCI cases that underwent primary PCI followed by a review of the contemporary evidence on the safety of acute PCI in this challenging condition.
A 53-year-old man presented to the emergency department with sudden dysphasia associated with left sided weakness. He was alert and able to follow commands. Collateral history from his family stated that he had persistent lower chest pain that started a few hours before the onset of dysphasia. His hemodynamic status was stable with blood pressure 133/79 mmHg and heart rate 85 bpm. Examination revealed left facial palsy, left sided limbs drift and expressive dysphasia. He had a National Institute of Health Stroke Scale of 1. Computed Tomography (CT) of the brain showed lacunar infarct in the anterior limb of the right internal capsule with no evidence of intracranial haemorrhage. Intracranial cerebral angiogram demonstrated mild luminal irregularities in the anterior posterior circulation with no large vessel occlusion. Meanwhile electrocardiogram (ECG) showed ST elevation in the inferior leads with reciprocal ST changes (Figure 1A, Figure 1B and Figure 1C). In view of persistent chest discomfort, emergency coronary angiogram was performed that revealed 99% subtotal occlusion at the mid right coronary artery (mRCA). Primary percutaneous coronary intervention (PCI) was performed to the mRCA with a drug eluting stent (Desyne 2.75 × 32). An echocardiogram showed left ventricular ejection fraction (LVEF) of 40%. He was commenced on dual antiplatelet therapy DAPT (aspirin and ticagrelor). During hospitalization, his initial neurological deficits had completely resolved. Follow up magnetic resonance imaging (MRI) brain performed on day 3 of admission showed acute infarcts in the right middle cerebral artery (MCA) territory with no evidence of hemorrhagic conversion. On day 4 of admission, he was discharged home on optimal medical therapy.
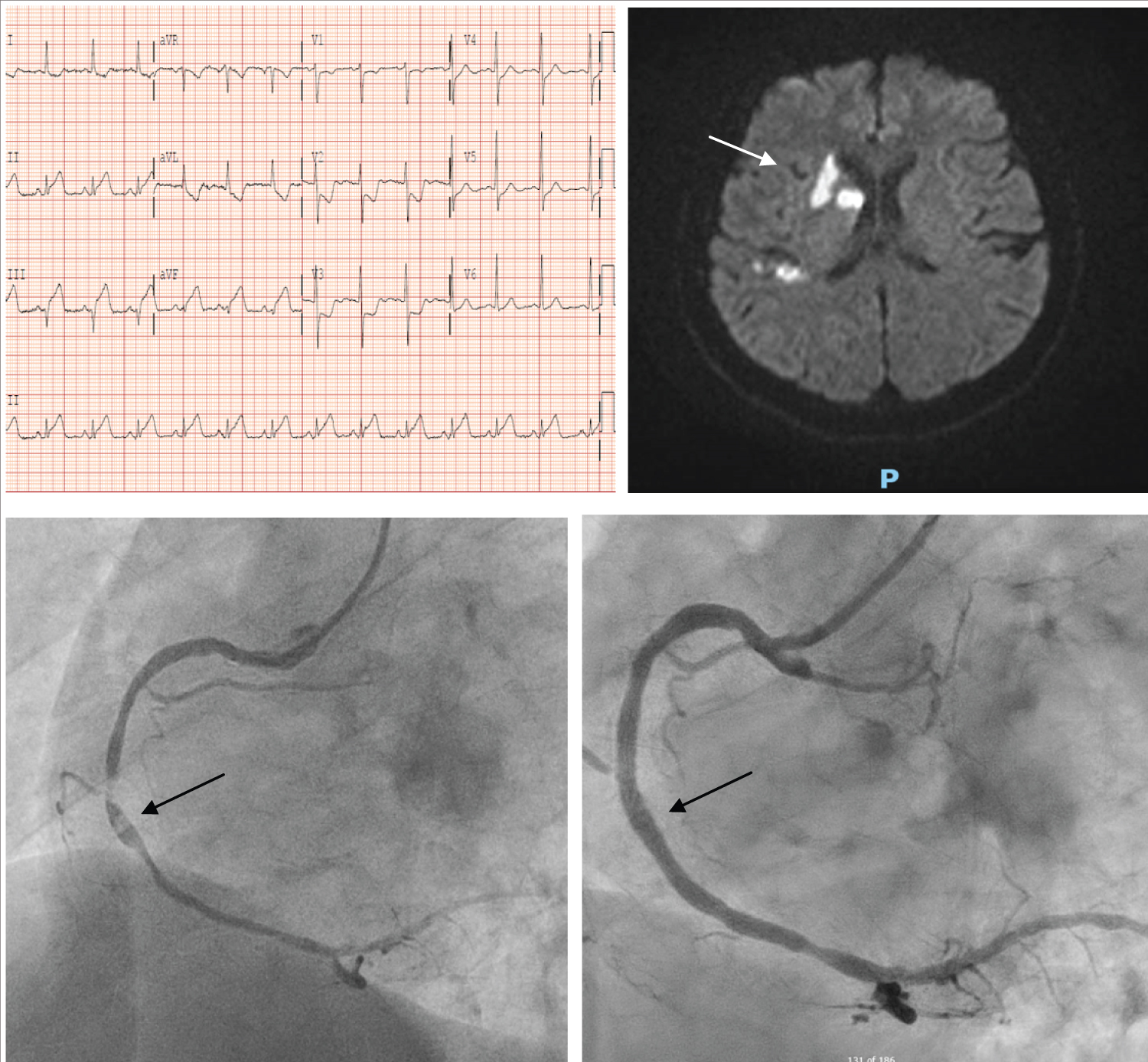 Figure 1: (A) ECG showed inferior ST elevation with reciprocal ST depression; (B) MRI brain showed acute right middle cerebral artery (MCA) territory infarcts without haemorrhagic transformation; (C) Angiographic findings of before and after mid right coronary artery stenting.
View Figure 1
Figure 1: (A) ECG showed inferior ST elevation with reciprocal ST depression; (B) MRI brain showed acute right middle cerebral artery (MCA) territory infarcts without haemorrhagic transformation; (C) Angiographic findings of before and after mid right coronary artery stenting.
View Figure 1
A 61-year-old man with no significant cardiovascular risk factors was brought in by ambulance for new onset of altered mental state. Pre-hospital ECG showed inferior leads ST elevation. Upon arrival, he was found to be drowsy with right sided limb weakness. Blood pressure was low with new findings of complete heart block. Examination revealed dense right hemiplegia with a NIHSS of 20. CT brain showed acute left MCA territorial infarcts in the lentiform nucleus and right posterior parietal region with no haemorrhagic conversion. There was a complete thrombosis of the left internal carotid artery. He was assessed by the stroke team with a decision made not for neurointervention in view of hemodynamic instability. After counselling for the risk of intracerebral hemorrhagic conversion, we proceeded with emergency coronary angiogram. Full dose dual antiplatelets were loaded. He was found to have complete occlusion of a large dominant left circumflex artery (LCx). Emergency PCI was done using a DES (Ultimaster 2.5 × 38 mm). Subsequent echocardiogram showed LVEF of 45%. He remained clinically stable throughout his hospitalization, but without improvement of his neurological deficits. Follow up MRI brain showed multi territorial infarcts likely due to cardioembolic events with petechial foci of hemorrhagic conversion. After 1 month of hospitalisation, he was transferred to community hospital for continuation of rehabilitation (Figure 2A, Figure 2B and Figure 2C).
 Figure 2: (A) ECG showed inferior ST elevation with reciprocal ST depression; (B) MRI brain showed multiple acute left MCA territory infarcts with petechial foci of hemorrhagic conversion and multifocal acute lacunar infarcts scattered in the right cerebral hemisphere; (C) Angiogram findings of before and after left circumflex artery stenting.
View Figure 2
Figure 2: (A) ECG showed inferior ST elevation with reciprocal ST depression; (B) MRI brain showed multiple acute left MCA territory infarcts with petechial foci of hemorrhagic conversion and multifocal acute lacunar infarcts scattered in the right cerebral hemisphere; (C) Angiogram findings of before and after left circumflex artery stenting.
View Figure 2
An 80-year-old man was admitted for persistent vertigo. He had past medical history of diabetes, hypertension and hyperlipidemia. Examination revealed weakness in his left sided limbs. Urgent CT brain showed possible acute infarct in the right precentral gyrus. MRI brain showed small, scattered acute infarcts in the bilateral frontal lobes with mild petechial haemorrhagic conversion. On the same day evening, he complained of new onset chest discomfort with breathlessness. ECG showed inferior posterior STEMI. There was a new finding of bibasal lungs crepitation. After discussion with the patient and medical team, a decision was made to proceed with emergency coronary angiogram keeping in mind the risk of worsening hemorrhagic conversion. Successful PCI was performed to an occluded right coronary artery with a single DES (Resolute Onyx 3.5 × 38). In addition, he was found to have atrial fibrillation and therefore started on short term 1 month triple therapy (DAPT + NOAC) with plan for down titration to long term dual therapy (clopidogrel + NOAC). His echocardiogram showed LVEF of 35%. His initial neurological deficits gradually resolved during his hospital stay without clinical findings to suggest deterioration of initial cerebral haemorrhagic conversion. He was discharged from hospital on day 8 of hospitalisation (Figure 3A, Figure 3B and Figure 3C).
 Figure 3: (A) ECG showed inferior ST elevation with reciprocal ST depression; (B) MRI brain showed mild petechial haemorrhagic conversion within one of the infarcts in the right frontal operculum; (C) Angiographic findings of before and after proximal right coronary artery stenting.
View Figure 3
Figure 3: (A) ECG showed inferior ST elevation with reciprocal ST depression; (B) MRI brain showed mild petechial haemorrhagic conversion within one of the infarcts in the right frontal operculum; (C) Angiographic findings of before and after proximal right coronary artery stenting.
View Figure 3
Primary PCI is the guideline-recommended coronary reperfusion strategy for patients who present with STEMI [2]. It is to be delivered in a timely fashion in order to attain maximal morbidity and mortality benefit by limiting infarct size, promoting favourable remodelling of the myocardial segments, and preventing deterioration of hemodynamic status. During PCI, it is crucial to administer adequate antiplatelet and anticoagulant to reduce the risk of peri-procedural and post-procedural ischemic events. In addition, they help to prevent acute procedure-related thrombotic complications. Majority of STEMI patients would continue taking dual antiplatelets (DAPT) for a recommended period of up to 12 months.
However, long term DAPT comes with the higher risk of bleeding. In the Stent Anticoagulation Restenosis Study [3], the risk of major haemorrhagic complications was 1.8%, 5.5% and 6.2% in patients on aspirin, aspirin-ticlopidine and aspirin-warfarin, respectively. In particular, intracranial haemorrhage (ICH) is a major concern as it is associated with significant morbidity and mortality. In the PLATO trial [4], the incidence of ICH was 0.34% for ticagrelor-treated patients and 0.19% for clopidogrel-treated patients.
In the event of CCI, the ICH risk would undoubtedly be greater and thereby further complicating the decision making process. Following acute stroke, the cerebral vasculature is friable due to a breakdown of the blood brain barrier resulting in a higher risk of haemorrhagic conversion.
Despite various stroke studies [5,6] showing that dual antiplatelets therapy (aspirin plus clopidogrel) does not significantly increase the risk of intracranial haemorrhagic events, anticoagulant agent use remains a huge concern. The International Stroke Trial [7] demonstrated low but increased risk of haemorrhagic conversion associated with heparin use as compared to aspirin (1.2%). Meanwhile, TOAST study reported 2.2% of serious central nervous system haemorrhage among danaparoid treated patients as compared to 1.1% of control group [8]. Pil Hyung Lee and colleagues [9] observed that clinical risk factors such as age ≥ 75 years, hypertension, atrial fibrillation, end-stage renal disease, history of stroke or transient ischemic attack and use of vitamin K antagonists, were associated with an increased risk of post PCI ICH.
Till date, recommendations for optimal reperfusion strategy in CCI are still lacking. The American Heart Association/American Stroke Association [10] recommended treatment with IV-tPA at the dose appropriate for acute ischemic stroke, followed by percutaneous coronary angioplasty and stenting if indicated (Class IIa, Level of Evidence C). However, it did not provide the specific management regarding the acute myocardial infarction subtypes and severity. Moreover, the different dose requirements and timing of fibrinolysis therapies after onset hinder its use as definitive treatment.
This paper highlights the clinical dilemma in CCI patients presenting with cardiovascular instability: Is it safe to perform primary PCI and its associated risk of ICH?
We conducted a comprehensive literature search but there was no randomised trial evidence to support its safety. There are several reports of simultaneous CCI with varying approach to management. Case series by Tobias, et al. [11] concluded that PCI is safe in patients with stroke/TIA and concomitant acute coronary syndrome with numerically lower ICH event in patients undergoing PCI. Another case report by Yeo LLL, et al. [12] described a 53-year-old male that presented with acute ischemic stroke due to left proximal middle cerebral artery (MCA) occlusion and also found to have new onset atrial fibrillation and ST elevations in V2-V5. PCI and stenting of the mid left anterior descending artery was done followed by endovascular embolectomy of MCA with solitaire device. The patient was wheelchair bound with expressive aphasia at 3 months. Our findings are in accordance with these previous studies. All our three patients successfully underwent primary PCI with good cardiovascular outcome. Post PCI close observation and follow up MRI did not show any evidence of hemorrhagic transformation or worsening haemorrhagic conversion. Furthermore, our case 3 was commenced on short term triple therapy (DAPT + NOAC) in view of concurrent atrial fibrillation. At 6 months, we reported 100% survival with variable neurological recovery.
The ideal management of simultaneous CCI is a treatment strategy that benefits both vascular territories. Despite knowing antithrombotics used in coronary intervention for AMI increase the risk for haemorrhagic conversion of acute stroke, our findings highlight the need to individualize treatment in patients presenting with concurrent CCI. Primary PCI could potentially draw a huge clinical benefit among suitable CCI STEMI patients without a substantial risk of clinically significant ICH. Therefore we would propose primary PCI for CCI patients who presented with STEMI or unstable hemodynamic status. This is in keeping with the suggested CCI management algorithm by Kijpaisalratana and colleagues [13]. Nevertheless, a multi-disciplinary team approach is always crucial in determining the best treatment for each individual CCI patient. Further research is much warranted to risk stratify and identify the optimal treatment for CCI.
Although concurrent CCI is rare, it is a devastating clinical scenario that imposes huge decision making dilemmas among managing physicians. In our series, primary PCI as an initial life saving strategy appeared to be safe and efficacious for STEMI patients who presented with hyperacute simultaneous CCI.
None.
None.