Coronary Artery Ectasia is a pathology effecting nearly 4.9% of the general population. This disease process can be found in any one of the coronary arteries and often presents in patients with comorbid conditions such as coronary artery atherosclerosis and hypertension. This combination of disease processes is often difficult to treat due to the lack of peer-reviewed data and treatment guidelines for coronary artery aneurysms. Additionally, there is currently no general consensus on the use of oral anticoagulation in these patients. Here we document the case of a 60-year-old male who presented with a non-ST segment elevation myocardial infarction and was later found to have coronary artery ectasia, which was successfully treated with oral anticoagulation.
Coronary artery ectasia, coronary artery aneurysm, oral anticoagulation
The Coronary Artery Surgery Study defines coronary artery ectasia (CAE), or aneurysm, as the dilation of a coronary artery more than 1.5 times the adjacent coronary artery [1]. CAE is present in ~4.9% of the general population. It is a poorly understood disease in terms of the pathogenesis, associated conditions, and treatment options [1]. While this phenomenon has been recorded in all of the coronary arteries, it is most commonly found in the right coronary artery (RCA) (68%), followed by the proximal left anterior descending coronary artery (LAD) (60%), and left circumflex coronary artery (LCx) (50%) [1,2]. The pathogenesis of this disease is likely secondary to exaggerated and expansive vascular remodeling as the result of atherosclerotic plaque formation [3,4]. Here we report a very interesting case of coronary artery ectasia presenting as an Acute Coronary Syndrome with 13 months of follow up history.
Our patient is a 60-year-old male with a pertinent past medical history of controlled hypertension, hyperlipidemia, and non-ST segment elevation myocardial infarction (N-STEMI). He had no known coronary artery disease (CAD). In January 2021 the patient was hospitalized for an N-STEMI. He presented to the emergency department with chest pain and shortness of breath. An initial electrocardiogram conducted in the emergency department showed a normal sinus rhythm, with 1st degree AV block, left axis deviation, left anterior hemiblock, and nonspecific ST-T wave changes. Following his admission to the hospital, a transthoracic echocardiogram demonstrated left ventricular ejection fraction of 55-60% with no regional wall movement abnormalities, valvular dysfunction, or pericardial effusion. Labs conducted in the hospital were normal with the exception of the patient's troponin, which peaked at 438 ng/ml (reference range: < 0.4 ng/ml). The patient underwent diagnostic cardiac catheterization which demonstrated a patent left main coronary artery (left main), proximal LAD with aneurysms and diffuse ecstasies up to the mid segment, mid-LAD with 40% stenosis. The circumflex artery was also abnormal with diffuse ectasia in the proximal and mid-segments. Similar findings were noted in the proximal, mid, and distal Right Coronary Artery (RCA). A 70% stenosis of the mid posterior descending artery (PDA) was also noted (Figure 1A, Figure 1B and Figure 1C). Due to the results of the heart catheterization no percutaneous intervention was performed and medical therapy was instituted. The patient was treated conservatively with aspirin 81 mg, atorvastatin calcium 40 mg, clopidogrel bisulfate 75 mg, metoprolol tartrate 25 mg BID, and valsartan-hydrochlorothiazide 160 mg/25 mg.
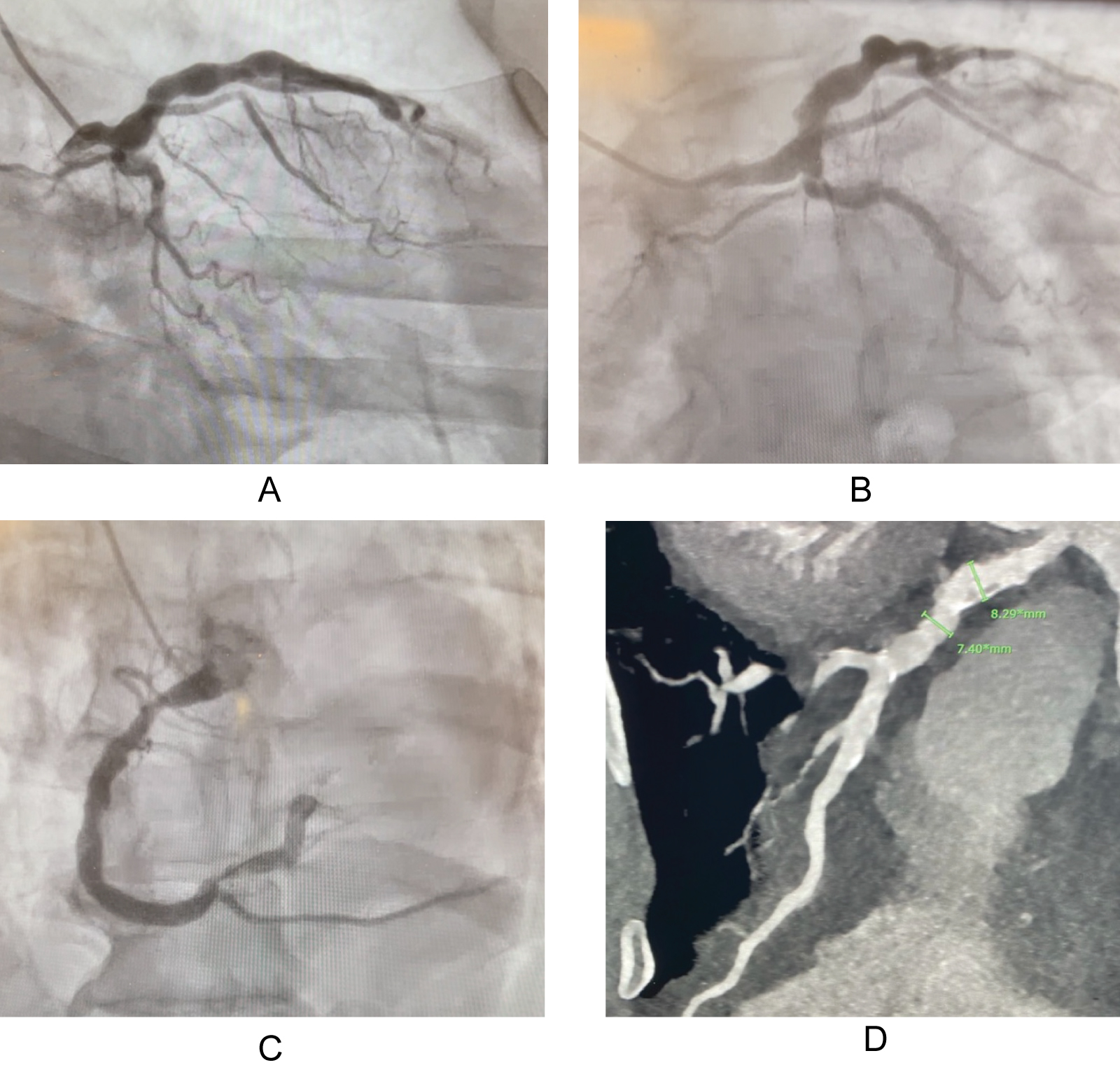 Figure 1: (A) Left anterior descending artery; (B) Left circumflex artery; (C) Right coronary artery; (D) Right coronary artery.
View Figure 1
Figure 1: (A) Left anterior descending artery; (B) Left circumflex artery; (C) Right coronary artery; (D) Right coronary artery.
View Figure 1
Two weeks following his hospital discharge, the patient was seen in cardiology clinic. He complained of fatigue since his NSTEMI, but he denied reoccurrence of chest pain, or shortness of breath. He also denied new-onset orthopnea, palpitations, blurred vision, dizziness, or lower extremity edema. A high resolution coronary computed tomography angiography (CCTA) was ordered to determine the size of the patient's aneurysms. He was started on isosorbide mononitrate extended-release 30 mg for angina-like symptoms if they were to occur. The possibility of starting oral anticoagulation depending on results of CCTA was also discussed.
The CCTA showed extensive atherosclerotic disease in all coronary vessels. The imaging showed significant atheroma and calcification of the PDA, 2 aneurysms in the proximal RCA (Figure 1D), extensive atheroma and calcification of the left main coronary artery and LAD, as well as 2 aneurysms, 7 mm and 8.3 mm, in the proximal and mid LAD, respectively. As a result of this study, the patient was instructed to stop taking aspirin 81 mg and start apixaban 5 mg BID in addition to his other cardiac medications. He continued to state he was symptom free since his hospitalization.
Thirteen months following his hospitalization, the patient continued to follow up on a regular basis for medical management. The patient continued to remain asymptomatic without any evidence of gastrointestinal bleeding or reoccurrence of ischemic chest pain with conservative management including medications and lifestyle modifications.
CAE is a rare condition with only a few studies completed to record the prevalence of this disease. Associated conditions appear to include significant atherosclerotic CAD as well as a history of prolonged, uncontrolled, hypertension [1]. Furthermore, the pathogenesis of CAE is quite complex and there is currently no one consensus as to the primary mechanism. But, overall, CAE is likely to occur as an exaggerated and expansive vascular modeling as the result of atherosclerotic plaque formation [3,4]. However, without a clear understanding of this disease's pathogenesis and a lack of prospective randomized trials, ideal and guideline directed medical therapy (GDMT) treatment modalities have not been introduced or agreed upon. Our patient had many of the comorbid conditions as described in the literature. The data however are often conflicting.
A study conducted in 1983 found CAE to be present in 4.9% of individuals (patient population of 20,067), while another study conducted 2 years later found the prevalence to be 1.4% (patient population of 4993) [1,5]. Likewise, several undertakings have been made to discover which the most are commonly found comorbid conditions associated to patients with CAE. A 2004 study conducted in a Singapore hospital analyzed 8641 cases of CAE and found the most common comorbid conditions to be coronary artery disease (82% of patients), hyperlipidemia (63% of population), hypertension (59% of patients), and type II diabetes mellitus (31% of patients) [6]. The prevalence of these comorbid conditions were reaffirmed 2 years later by another similar sized investigation which found coexistent coronary artery disease in 59% of patients, hyperlipidemia (54.9% of patients), hypertension (47.5% of patients), and type II diabetes mellitus (16.4% of patients) as the most common comorbid conditions in a patient with CAE [7].
CAE can be classified into 4 major subtypes depending on the degree of coronary artery involvement. Type 1 CAE describes diffuse ectasias with aneurysmal lesions in 2 vessels. Type 2 CAE involves diffuse ectasias in 1 vessel and discrete ectasias in another. Type 3 CAE is diffuse ectasias in only 1 vessel and Type 4 is classified by discrete ectasia in only 1 vessel [8]. The most common arteries which are involved, in order of descending prevalence, are the RCA, proximal LAD, and LCx. Involvement of the left main coronary artery is by far the least common presentation of CAE, only occurring in 0.1% of the population [1,2].
As previously mentioned, the pathogenesis of CAE is not fully understood. The current understanding of this disease process is that of exaggerated vascular remolding secondary to severe atherosclerotic plaque or atheroma formation [3,4]. However, the predominant mechanism and various pathways leading to exaggerated vascular remodeling is still a mystery. One research study concluded that proteolytic enzymes, such as metalloproteases, play a significant role in breaking down the intima of the blood vessel to allow for expansion [3,4].
Other suspected mechanisms include hyperinsulinism interfering with extracellular matrix production, nitric oxide production causing the breakdown of blood vessel walls, and chlamydia pneumoniae producing heat shock proteins and metal metalloproteases which reduce blood vessel integrity [9,10]. Currently, the most predominant theory is that which points to proteolytic enzymes causing degeneration of the media. In fact, histological analysis of these blood vessels demonstrates cystic medial degeneration and lymphohistiocytic infiltration into the tunica media without evidence of the degeneration outside of the aneurysm in the adjacent blood vessel [11]. Furthermore, specific genetic anomalies have been studied and seem to predispose an individual to developing CAE. These genetic factors include the presence of angiotensin converting enzyme DD genotype, metal metalloprotease-3 allele, and mutation of the low density lipoprotein receptor [12-14].
The clinical presentation of patients with symptomatic CAE is very similar to that of patients with symptomatic CAD. Symptoms consist of typical ischemic chest pain with or without exertion, with radiation to the mandible or arms, and associated shortness of breath. However, due to the increased prevalence of coronary atherosclerosis in patients with symptomatic CAE, the incidence of STEMI or N-STEMI are increased due to risk of thrombus formation or distal embolization of plaque as well as microvascular dysfunction [15-18].
Considering that CAE is often an incidental finding at cardiac catheterization and frequently the initial study demonstrating the disease, cardiac angiography is the most commonly used method of diagnose by default. Fluoroscopy will often show abnormalities in blood flow filling and washout, in addition to pooling of contrast dye within the ecstatic segments themselves [19]. Other methods which can be used to identify and determine the size of the aneurysms include less invasive coronary MRA or CCTA, or more invasive intravascular ultrasound during cardiac catheterization [19].
While there are many modalities for diagnosing CAE, deciding on treatment is more difficult and frequently empirical. This is likely due to the lack of prospective randomized trials involving medical therapies or procedural intervention. Thus, there are currently no standardized treatment guidelines. As a result, the medications used to treat CAE are based upon their ability to theoretically combat progression of the ectasia and prevent occurrence of acute coronary syndrome (ACS). Aspirin is often used as a first line treatment in patients due to the high prevalence of concomitant CAD [20]. Studies recommending the use of anti-platelet therapy such at P2Y12 inhibitors have not been conducted. One study suggested the use of warfarin due to the presence of regional flow abnormalities [21]. Additionally, statins have been recommended due to the suspected role of metal metalloproteases in the pathogenesis of CAE [22,23]. Similarly, the use of nitrates is not recommended due to the hypothesis that nitric oxide could play a potential role in the develop of coronary aneurysms [24]. Following the failure of medical therapy, treatment using percutaneous coronary intervention with a polytetrafluoroethylene covered balloon-expandable stent has been shown to be an effective treatment in ecstatic areas in which a side branch of the treated artery is not covered [25].
However, percutaneous approaches have been complicated by decreased procedural success and increased risk of no-reflows as well as distal embolization, stent thrombosis, and repeat revascularization procedures. Lastly, if percutaneous coronary intervention is not an option, coronary artery by-pass grafting is a viable method with positive outcomes [26-28].
Further studies need to be completed to advance not only our understanding of the comorbidities associated with CAE, but also the pathogenesis and potential treatment options. There is a wide variation in disease severity and the inherent potential complications associated with the severity of disease. Improvement in patient outcomes and mortality is possible with a better understanding of this disease and better algorithm for therapy [29]. The heterogeneity of this disease warrants tailored therapy to each patient as well as close attention and aggressive risk factor modification.
The authors declare that there is no conflict of interest regarding the publication of this article. The authors received no specific funding for this work.
All authors contributed to this report equally.
The authors received no specific funding for this work.