Extracutaneous melanoma is not a frequent situation, making a difficulty for the diagnosis. It is characterized by a poorer prognosis and rapid metastasis. The research for a primitive cutaneous melanoma is obligatory before retaining this entity. The dermatologist role is to eliminate a cutaneous primitive melanoma by the clinic and dermoscopic examination. We report five cases of non-cutaneous melanoma: Three mucosal melanoma, one choridian, and the fifth one is a parotid melanoma, and we will discuss this neoplasm via a literature review.
Extracutaneous melanoma is a rare neoplastic affection, its epidemiology is sparsely described, and reported studies upon the literature are limited by time, and by geographic gaps in available data [1]. Its prevalence is about 4-5% only [2] with an annual age-adjusted incidence rate of 8.2 per million in the population [3] it's biologically knozed to be more aggressive than cutaneous melanoma [4]. The Clark level and Breslow are not available in this entity [4]. We report five cases of extracutaneous melanoma (choroidian, vaginal, anal and parotid).
Herein we describe five cases of non-cutaneous melanoma of different locations, with a literature review.
A 38-year-old patient with no pathological history, suffering from a progressive decrease in visual acuity without eye pain or oculomotor paralysis. Ophthalmologic examination revealed a pigmented retinal tumor indicating enucleation. Histopathological examination showed choroidal melanoma (Figure 1). The patient was referred to our structure and the dermatological examination did not detect any suspicious lesions. This patient did not need additional treatment with a three-year follow-up without recurrence.
 Figure 1: Gx200, epithelioid proliferation on the choroid with evident pigmentation.
View Figure 1
Figure 1: Gx200, epithelioid proliferation on the choroid with evident pigmentation.
View Figure 1
A 41-year-old woman, had hematuria with the discovery of a pigmented polyploid tumor upon the ureteral meatus. Examination of the rest of the tegument did not objectify a suspicious skin lesion. After general anesthesia, surgical examination showed a pigmented periurethral swelling, tumor taking the meatus and the urethra with intravaginal extinction (Figure 2). A biopsy confirmed the diagnosis of Urethero-vaginal melanoma. The patient was judged not operable, and received chemotherapy after discovering lymphadenopathy and metastases in the assessment of extension. The treatment is still in progress.
 Figure 2: Black tumor arising in the uretheral meatus.
View Figure 2
Figure 2: Black tumor arising in the uretheral meatus.
View Figure 2
It's a 65-years-old man, who received an operation of the anal marge four years ago. The histologic examination was talking about an anal melanoma, the patient has been missed by a follow up, and came back to our structure after the apparition of an edema and a pigmented lesion of the left eyelid. Cutaneous metastasis of an anal melanoma has been retained and the scannographic imaging shoes diffuse metastasis, with cerebral, pulmonary locations (Figure 3). This patient died one month later without a specific cause.
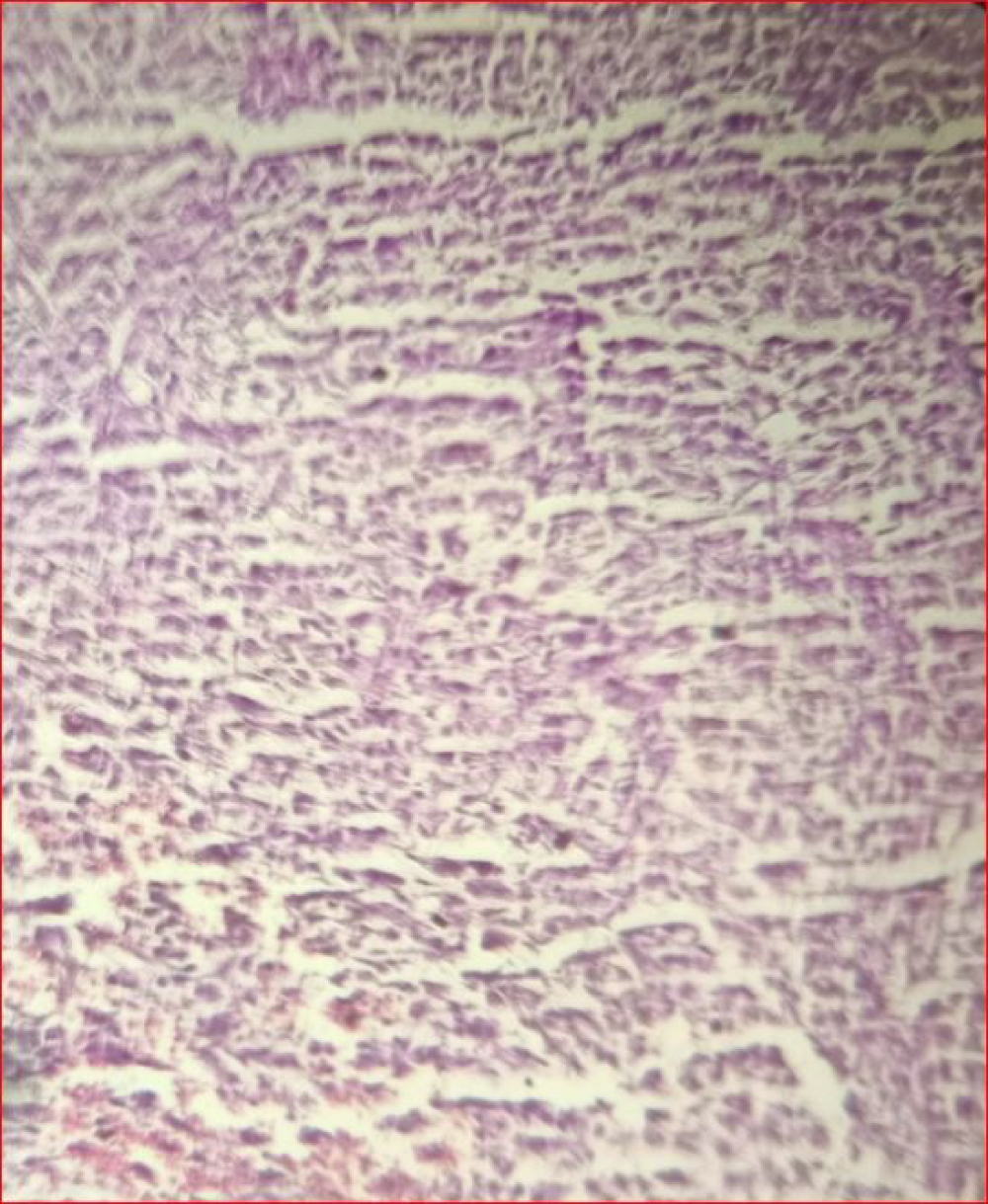 Figure 3: Gx400, epithelioid malignant proliferation on the rectum.
View Figure 3
Figure 3: Gx400, epithelioid malignant proliferation on the rectum.
View Figure 3
A patient of 71 years, having an antecedent of an explained nephrectomy of the right kidney 30 years ago suffered from an occlusive syndrome. After anorectal examination, a process of the rectum have been observed, the histological analysis found a melanoma of the rectum (Figure 4), and the patient benefited of an abdominopelvis amputation with definitive stomy. The extensif imaging showed hepatic and splenic secondary locations, the patient received adjuvant radiotherapy and chemotherapy after multidisciplinary decision. The patient was referred to our structure, and we did not found any suspicious lesion on clinic and dermoscopic examination.
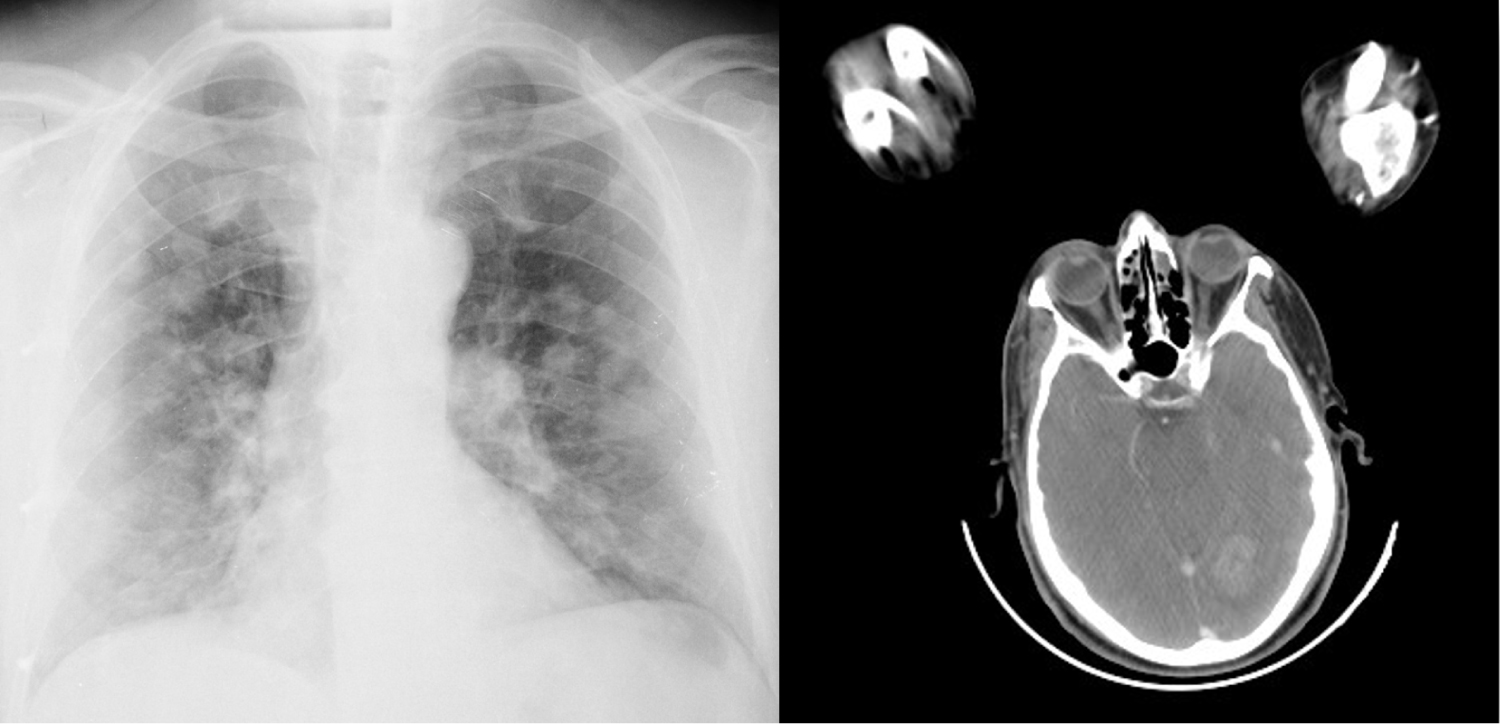 Figure 4: Pulmonary and cerebral metastasis of an anal melanoma.
View Figure 4
Figure 4: Pulmonary and cerebral metastasis of an anal melanoma.
View Figure 4
A 56-year-old woman, with a history of cerebral ischemic stroke four years ago. Presented for the past two years a palpable nodule in the left mandibular region, gradually increasing in size. Initial scannographic exploration showed an intraparotidian tissue process of 9 × 5 cm long axis projecting into the adjacent soft tissues with infiltration of the sternocleidomastoid muscle, The biopsy discovered a melanoma with positive immunohistochemistry (melan A HMB 45PS 100 and SOX-10)In addition, the patient had no cutaneous or mucosal lesions suggestive of malignancy. In the extension assessment, the patient benefited from a cerebro-thoraco abdominopelvic tomodensitometry showing secondary locations. Then the patient received radiotherapy with palliative chemotherapy (Table 1).
Table 1: Clinical characteristics of our case series of non-cutaneous melanoma. View Table 1
Generally, Melanoma is categorized on cutaneous, mucosal and ocular according to McLaulin, et al. In other words, extracutaneous melanoma included ocular, anorectal, mucosal, nail beds, conjunctival, vaginal, urogenital, orbital, esophageal, and leptomeningeal malignant melanomas [3].
There are such criteria defined by Ainsworth and colleagues and Carstens and colleagues respectively in 1976 and 1984 [5] to retain a non-cutaneous primitive melanoma.
Mucosal melanoma is a rare variety, representing only 1.4% of all melanomas [3]. This aggressive tumor occurs in elderly patients [3], the average age is 70 versus 44 for cutaneous melanoma [6]. Out of the buccal melanoma, the most frequent mucosal melanoma are respectively urogenital and anorectal mucosal melanoma.
Genitourinary and precisely the vulvovaginal location are the most frequent mucosal melanoma, that explain its frequencies on female versus male [7], with a sex ratio of 0.54 [3], compared to the cutaneous melanoma, the Multifocal and amelanotic character is more frequent in this entity [8]. It's quite rare and consisting on less than 3% of malignant vaginal tumors [9] manifesting by a pigmented macula with irregular borders associated to pruritus or bleeding. Imaging findings shows an infiltrating parietal mass with isotohyperintense signal on T1-weighted MRI and usually hyperintensesignal on T2-weighted images [6]. Rapid spreading and fatal evolution are habitual, and resection is generally difficult. Either tumoral resection has been successful, the prognosis is almost poor, with a median survival of 12-25 months, both of our patients having this location have a poor prognosis which concords of the literature data [10-12]. The mainstay therapy is the surgical excision, if the tumor spreads to the bladder or rectum, an anterior or posterior extenteration [4], the hysterectomy is indicated if the tumor is in the upper vaginal third part [13].
It represents a few parts of the colorectal malignancies, 0.05 percent of all tumors of this area [14]. It has been proved that HIV infection increases the risk of anorectal melanoma [15]. Rectal location is the most reported (42%), followed by the anal canal (33%) [14]. It's is usually seen as an intraluminal fungating or polypoid mass in the anal canal or the distal part of rectum with Perirectal infiltration [6]. Abdominoperineal resection is the recommended treatment, with a considerable comorbidity [13,16]. That was the case of our patient. In additional, lymph node resection has not been recommended because there is no effective amelioration of the median survival with such radical surgery [16-18]. As like as all metastatic melanoma, a systemic chemotherapy or immunotherapy is recommended (Dacarbazin, Mimustine, Vincristine and Interferon beta).
Ocular melanoma is a Uveal melanoma in 80% of the cases [3]. It is the most common ocular tumor, including iris, ciliary body and choroid. Its incidence is about 5.1 per million habitant annually.
It affects white race people 97.8% versus 0.8% of black race people [19], and may be associated with ota naevus [20]. This affection is first detected by the ophtalmologists, then ultrasonography can be a useful imaging but not sufficient, MRI is necessary for the exact delineation of the tumor and evaluation of optic nerve involvement and extraocular extension [6]. Clinical and histological manifestation of uveal melanoma is variable, making so difficult to clinically differentiate it from other neuroectodermal tumors with melanin content such as melanocytoma, melanotic meningioma, schwannoma and neurofibroma [21-23].
Radiation is the mainstay therapy, but large and unsuitably located melanoma of the choroid must be treated by enucleation and that was the case of our patient. Radiosurgery with the gamma knife may be benefic with 98% of local control during the three first years during the follow up [24].
Parotid melanoma with unknown primary is recognized in the literature but still be incompletely described. There is a study published by Scott, et al. in 2016 concluding that patients having a primary melanoma of the parotid with unknown primitive tumor have a poorer prognosis compared to parotid melanoma with known primary tumor [25]. In this study, there was a lack to differentiate between a primary melanoma of the parotid and a parotidian melanoma with an unknown primitive tumor. Several studies are needed to clarify this confusion and define this entity of primary parotid melanoma (Figure 5).
 Figure 5: Melanoma of the parotid: Bilobed ulcerated amelanotic tumor.
View Figure 5
Figure 5: Melanoma of the parotid: Bilobed ulcerated amelanotic tumor.
View Figure 5
Finally, other localizations are well described in the literature. Among them, we cite the primary melanoma of the lung, which represent 0.01% of all lung tumors [26], melanoma of the tractus digest if whose incidence is increasing [15]. An anecdotal reported location is the retroperitoine, where the diagnostic of primary melanoma was a challenge [5].
Extracutaneous melanoma is a well-defined entity. Its pathogenesis remain unclear with more aggressively and high risk of metastasis. Dermatological examination is indispensable to retain the diagnosis by eliminating a cutaneous primitive melanoma. The Management of this pathology requires a multidisciplinary collaboration with a closed follow up.
The authors declare no competing interest.
All the authors contributed to the conduct of this work. All authors also state that they have read and approved the final version of the manuscript.
We are indebted to our patients for giving us the consent for the publication.