Elective reconstruction in the valgus hindfoot is a complex and varied field of orthopaedic surgery. Often multiple procedures, both bony and soft tissue are required. The surgical aims are to create a plantigrade foot, restore hindfoot alignment and re-create the medial longitudinal arch in an attempt to allow more normal biomechanical function. Invariably a calcaneal osteotomy is required to correct hindfoot alignment. There are various methods of performing a calcaneal osteotomy [1] but no consensus as to which provides the best correction. Traditionally in our unit a medial displacement calcaneal osteotomy (MCDO) combined with lateral column lengthening (LCL) was used to do this. In this study we undertook radiological evaluation of the efficacy of a different type of osteotomy, the 'z-calcaneal osteotomy'.
Our aim was to assess the radiological improvement in various foot and ankle indices including talonavicular uncoverage, Meary's angle, incongruency angle and calcaneal pitch amongst others [2]. The study was performed retrospectively on 18 foot reconstructions in 14 patients where the z-calcaneal osteotomy was utilised. The surgeries were performed between 2012 and 2017 in Altnagelvin Hospital in Londonderry, Northern Ireland. A series of standardised weight bearing dorsoplantar (DP) and lateral radiographs and hindfoot alignment views were taken pre-operatively and post-operatively. Radiographic parameters were measured by two blinded investigators in both sets of radiographs to assess degree of correction after each reconstruction. The data was analysed using SPSS 22 for Windows and a paired student t-test used to compare the difference in means.
Dorsoplantar radiographic outcomes revealed a mean reduction of 15.7% in talonavicular uncoverage percentage (p = 0.001) and a mean reduction of 22.8 degrees in the incongruency angle (p = 0.01). The talonavicular uncoverage angle was improved by a mean of 16.1 degrees (p = 0.023). On the lateral radiographs the calcaneal pitch was increased by a mean of 6.5 degrees (p = 0.04) and Meary's angle was improved by a mean of 54.3 degrees. Hindfoot alignment was improved by a mean of 6.7 degrees (p = 0.03).
This study demonstrated significant improvements in the radiological indices measured when comparing pre-operative and post-operative radiographs in the cohort of foot reconstructions considered. As the z-calcaneal osteotomy was performed in conjunction with other bony and soft tissue procedures it is not possible to ascertain what degree of correction is attributable to the z-calcaneal osteotomy and what proportion is due to the other procedures.
The method we utilised for assessing hindfoot alignment was standard hindfoot alignment view (HAV) with angle measurement using standard Picture Archiving and Communication System (PACS) software. A long axial view may produce more reliable assessment of the hindfoot [3] and this is one of the limitations of this study. While the z-calcaneal osteotomy does appear to give good radiological correction of the valgus hindfoot, this was a small cohort of patients and the post-operative hindfoot imaging was not as complete as we would have liked. Further studies assessing both radiological improvement and clinical outcome are required to ascertain whether the z-osteotomy provides superior results than other established surgical techniques.
Calcaneal osteotomy, Z osteotomy, Valgus hindfoot, Acquired adult flatfoot deformity
Elective foot reconstruction is a complex and varied field of practice. The valgus hindfoot presents a particular challenge and often multiple procedures, both bony and soft tissue, are required to achieve the desired result. The valgus hindfoot can result from many conditions, such as, posterior tibial tendon dysfunction (PTTD), charcot foot, skewfoot and acquired adult flatfoot deformity (AAFD) amongst many others. In any of these conditions the biomechanics of the foot and ankle are altered, causing pain, deformity and functional impairment [4]. If the valgus hindfoot in the ambulating patient is left unattended, the deformity typically progresses, eventually leading to soft tissue breakdown, ulceration and infection. If neglected, often salvage procedures or amputation are the only viable options. It is therefore crucial to intervene in the at risk valgus hindfoot to arrest this cascade of events.
Reconstruction in the valgus hindfoot invariably requires a calcaneal osteotomy to correct hindfoot alignment. There are various methods of performing a calcaneal osteotomy [1] but no consensus as to which provides the best correction. Traditionally in our unit a medial displacement calcaneal osteotomy (MCDO) combined with lateral column lengthening (LCL) was used to do this. In this study we undertook radiological evaluation of the efficacy of a different type of osteotomy, the 'z-calcaneal osteotomy'.
In this study we carried out radiographic analysis of patients' feet pre-operatively and post-operatively following reconstructive surgery which utilised the z-calcaneal osteotomy. Our aim was to assess the radiographic change in various indices including hindfoot alignment, talonavicular uncoverage percentage, Meary's angle, calcaneal pitch and incongruency angle amongst others [2].
This was a retrospective study performed on 18 consecutive foot reconstructions in 14 patients where the z-calcaneal osteotomy was utilised. The surgeries were performed between 2012 and 2017 in Altnagelvin Hospital in Londonderry. The patients all had valgus hindfeet with varying aetiologies including pes planus, PTTD and skew foot. A series of standardised weight bearing dorso-plantar (DP), lateral and hindfoot alignment radiographs were taken pre-operatively and post-operatively. The hindfoot alignment views were taken with the x-ray beam inclined at 20 degrees to the horizontal which was our department's standard method of performing this view.
The Z-calcaneal osteotomy [5] is performed through a single lateral incision. The lateral side wall of the calcaneus is exposed, taking care to protect the peroneal tendons. The osteotomy is then performed in the position as shown in Figure 1. Care must be taken when extending the osteotomy to the medial wall of the calcaneus; we recommend using a small osteotome to tap through the final shell of cortex to avoid damaging medial structures. Once the osteotomy is complete a small osteotome can be inserted into either vertical portion of the osteotomy and used as a lever to achieve the desired amount of correction. A wedge shaped piece of iliac crest bone graft (ICBG) or a piece of bone substitute is inserted in the gap to maintain the correction. A single headless screw is then placed from the plantar aspect across the osteotomy. This osteotomy method achieves a translational correction coupled with a rotation dialled in at the osteotomy site and aids both medialisation of the calcaneal strike point and also re-creation of the medial longitudinal arch.
 Figure 1: Z-calcaneal osteotomy. View Figure 1
Figure 1: Z-calcaneal osteotomy. View Figure 1
Each of the pre-operative and post-operative x-rays were assessed and the following radiographic indices were measured using the techniques described by S J Ellis [2]. On the DP radiograph: Talo-navicular uncoverage angle, talonavicular uncoverage percentage, talar-1st metatarsal angle, incongruency distance and incongruency angle. On the lateral radiograph: Talocalcaneal angle, talar-1st metatarsal angle, calcaneal pitch, medial cuneiform-5th metatarsal height. On the hindfoot alignment radiograph the distance between the longitudinal axes of the calcaneus and tibia were measured as a surrogate of the hindfoot alignment.
Each radiograph was independently assessed by two orthopaedic trainees who were blinded to the patient details and the operating surgeon. An average was taken of their measurements to reduce inter-observer error. The orthopaedic trainees had been trained in the use of the Picture Archiving and Communication System (PACS) software used to perform the measurements. Data was entered into an Excel sheet and analysed using SPSS 22 for Windows. Continuous variables were expressed as mean and standard deviation. A paired student t-test was used to compare the differences observed between means. Unadjusted p-values were then calculated and a p-value less than 0.05 was considered statistically significant.
There were a number of statistically significant differences which are summarised in Table 1. Dorsoplantar radiographic outcomes revealed a mean reduction of 15.7% in talonavicular uncoverage percentage (p = 0.001) (Figure 2) and a mean reduction of 22.8 degrees in the incongruency angle (p = 0.01) (Figure 3). The talonavicular uncoverage angle was improved by a mean of 16.1 degrees (p = 0.023) (Figure 4). On the lateral radiographs the calcaneal pitch was increased by a mean of 6.5 degrees (p = 0.04) (Figure 5). Meary's angle (talar - 1st metatarsal angle on lateral x-ray) showed an improvement of 29.7 degrees but this result did not meet statistical significance (p = 0.296) (Figure 6).
 Figure 2: Talonavicular uncoverage percentage. View Figure 2
Figure 2: Talonavicular uncoverage percentage. View Figure 2
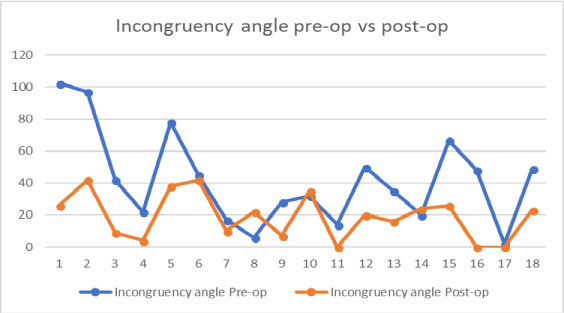 Figure 3: Incongruency angle pre-operatively vs. post-operatively. View Figure 3
Figure 3: Incongruency angle pre-operatively vs. post-operatively. View Figure 3
 Figure 4: Talonavicular coverage angle, pre-operatively vs. post-operatively. View Figure 4
Figure 4: Talonavicular coverage angle, pre-operatively vs. post-operatively. View Figure 4
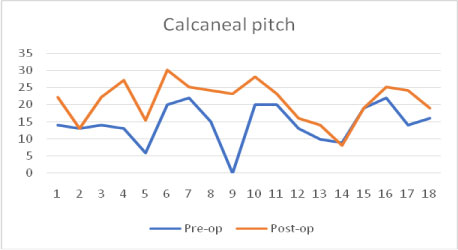 Figure 5: Calcaneal pitch, pre-operatively vs. post-operatively. View Figure 5
Figure 5: Calcaneal pitch, pre-operatively vs. post-operatively. View Figure 5
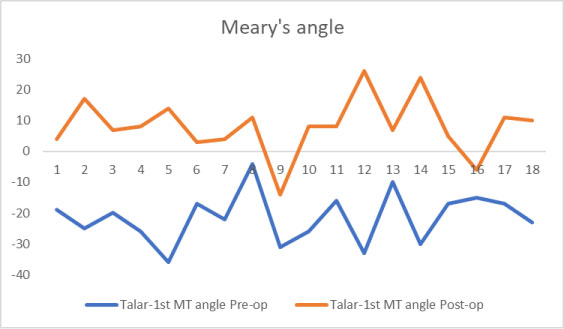 Figure 6: Meary's angle, pre-operatively vs. post-operatively. View Figure 6
Figure 6: Meary's angle, pre-operatively vs. post-operatively. View Figure 6
Table 1: Results summary. View Table 1
The hindfoot alignment view radiographs were performed in all but two cases. In two further cases the quality of the radiography was not sufficient to make an accurate assessment of hindfoot alignment, thus the data set is not as complete as for the other measurements. Of the 14 cases where pre-operative and post-operative measurement of hindfoot alignment was possible there was a mean improvement of 6.7 degrees (p = 0.03) (Figure 7).
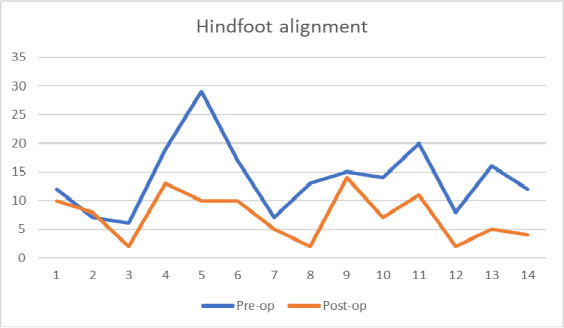 Figure 7: Hindfoot alignment, pre-operatively vs. post-operatively. View Figure 7
Figure 7: Hindfoot alignment, pre-operatively vs. post-operatively. View Figure 7
The surgical correction of the valgus hindfoot invariably involves a variety of surgical procedures. The goals are to create a plantigrade foot, correct hindfoot alignment and restore the medial longitudinal arch to achieve a more biomechanically normal foot. Often a calcaneal osteotomy is required [4], primarily to correct hindfoot alignment and secondarily contributes to re-creation of the medial longitudinal arch. There are various methods and approaches described for performing a calcaneal osteotomy [1]. The osteotomy can be a single plane translational osteotomy, a lengthening osteotomy, closing wedge osteotomy (in the varus hindfoot) or a complex osteotomy which allows movement and correction in all three planes [1]. There is no consensus as to which osteotomy provides the best correction in the valgus hindfoot. Hintermann reported excellent results in a cohort of patients with PTTD treated with lateral column lengthening and soft tissue reconstruction [6], but there is a risk of non-union with this procedure [7].
This study focuses on the use of the z-calcaneal osteotomy in the correction of the valgus hindfoot. The z-osteotomy is a complex osteotomy [1] which allow correction in all three planes. This procedure was performed in conjunction with various soft tissue and bony procedures [4] depending on the exact nature of the deformity and degree of correction required. Thus, it is not possible to ascertain what degree of correction is induced by the z-calcaneal osteotomy in isolation which represents a limitation of our study. Similarly it is not feasible to perform a direct comparison between the z-calcaneal osteotomy and medial displacement calcaneal osteotomy (MDCO) as both are performed in conjunction with multiple other procedures.
There are several methods for assessing hindfoot alignment radiographically [3,8]. Key to this assessment is the protocol for taking the radiograph and the standardisation of foot position to minimise error. The traditional method used in most departments in our region was popularised by Saltzman, et al. [8] in 1995. In a more recent paper it has been suggested that the long axial view is a more reliable view from which to assess the alignment of the hindfoot [3]. The long axial view is taken with the x-ray beam at an inclination of 45 degrees to the horizontal. In our study a standard hindfoot alignment view was taken with the x-ray beam at an inclination of 20 degrees with respect to the horizontal. Attempts to establish the use of the long axial view were not universally adopted by the radiology department so we opted to continue with the standard hindfoot alignment view for this study. This may represent a limitation in our study and infer less reliable measurement of hindfoot alignment [3]. The measurement of the alignment was performed using a standard PACS tool kit which allowed lines and angles to be annotated onto the radiographs. Measurements were performed by two orthopaedic trainees who were blinded with respect to patient details and performing surgeon. Both the pre-operative and post-operative radiographs had the same angles and distances measured by each of the two investigators using the same methods as described previously. An average was then taken of these measurements. There was no formal assessment of interobserver error which is a limitation of the study.
In conclusion, the z-calcaneal osteotomy does appear to give good radiological correction of the valgus hindfoot, however this was a small cohort of patients and the post-operative hindfoot imaging was not as complete as we would have liked. Further studies assessing both radiological improvement and clinical outcome are required to ascertain whether the z-osteotomy provides superior results than other established calcaneal osteotomy techniques.