Immediate implant placement in the esthetic zone, represents one of the biggest challenges in dentistry. It implies a multidisciplinary approach involving prosthetic and periodontal aspects to obtain long term stability, esthetic and functional results. A clinical case report is presented, taking into consideration periodontal and prosthetic management of an implant in the anterior zone, starting from the diagnosis, treatment plan, periodontal surgical procedures, provisionalization, and its definitive prosthetic rehabilitation.
When the loss of a tooth located in the esthetic zone is inevitable, the need for a prosthetic replacement is necessary. Nowadays, there are different prosthetic options; implant-supported prostheses are one of the most reliable treatment alternatives. Also, the possibility of immediate or early loading represents a satisfactory solution for the patients and the clinician, always considering the patients' individual characteristics [1].
The survival rate and the restoration of function for this type of treatment are high. However, to guarantee an aesthetically successful result is not always possible, due to the dimensional changes that occur in hard and soft tissues after the loss of a tooth [2]. For this reason, they are considered as a "Complex SAC" from the surgical and prosthetic point of view according to the International Team for Implantology (ITI). This treatment modality requires a team protocol, where the main planning, surgical and prosthetic aspects are taken into account to obtain the desired result [3].
From a periodontal point of view, an understanding of the dentogingival complex and its counterpart the peri-implant mucosa, as well as its biological and physiological responses are equally important. In the same way, it is necessary to take into consideration the intrinsic characteristics of the patient, the surgical procedure, and prosthetic management [4].
Within prosthetic management, it is necessary to determine if immediate provisionalization is possible at the moment of the surgery. There is a greater esthetic and functional demand from patients. Thus, it is also necessary to satisfy the need for a faster treatment and reduce discomfort during the healing period [5].
The latest concept is "Non-functionally loaded immediate provisionalization"; defined as a load where the provisional restoration is adjusted to clear all occlusal contacts in centric and eccentric movements. The non- functionally loaded immediate provisionalization protocol depends on optimal primary stability, adequate bone quality, and quantity. It will also depend on the alveolar anatomy after tooth extraction [6].
The main objective of immediate provisionalization is to preserve the gingival contours, maintain the natural emergence profile and to predict the final result. With this type of treatment, it is possible to place the final restoration 4 months after implant placement [7,8].
A 58-year-old female patient attended the periodontology department at Universidad Popular Autónoma del Estado Puebla (UPAEP) for consultation; "I want a full oral assessment". She did not report any important personal pathological history and was diagnosed with generalized periodontal disease stage I grade A [9]. After oral hygiene instructions, scaling and root planing, the patient was referred to a prosthetic assessment as part of the periodontal hygienic phase; in the restorative dentistry department, a clinical examination, intra- and extra-oral photography records, dental study models, and articulated diagnosis were carried out.
After prosthetic evaluation, a porcelain fused to metal crown with a metal cast post was removed in tooth 1.1 (Figure 1), which presented leakage and mismatched margins, as well as a dark coloration at the cervical margin level. Tooth 1.1 had no response to the vitality tests because it had a previous root canal treatment. When the restoration was removed, we could observe poor remaining tissue, dental walls with insufficient support and a compromised crown-root ratio, a Cone Beam was indicated to the patient, where insufficient remaining tissue was observed, poor root canal treatment and also a short root (Figure 2), due to these factors tooth extraction was indicated and an acrylic provisional was placed until the day of surgery.
 Figure 1: Initial situation.
View Figure 1
Figure 1: Initial situation.
View Figure 1
 Figure 2: Image of area surrounding tooth 1.1 in cone beam CT.
View Figure 2
Figure 2: Image of area surrounding tooth 1.1 in cone beam CT.
View Figure 2
A diagnostic wax-up and surgical guide were performed to continue with the surgical phase.
The surgical protocol consisted of an atraumatic extraction of the central incisor tooth (1.1). With the help of a 15 C scalpel blade, sharp dissection of the supracrestal fibers, and a tunnel towards the vestibular plate was performed to obtain an "envelope" (Figure 3 and Figure 4), the extraction socket was carefully debrided and the osteotomy was prepared for the placement of a 3.9 × 10 mm (V3 MIS) prosthetically guided implant (Figure 5), a 2 mm labial "gap" was obtained and the implant shoulder was placed 4 mm from the future gingival margin.
 Figure 3: Sharp dissection.
View Figure 3
Figure 3: Sharp dissection.
View Figure 3
 Figure 4: Atraumatic tooth extraction.
View Figure 4
Figure 4: Atraumatic tooth extraction.
View Figure 4
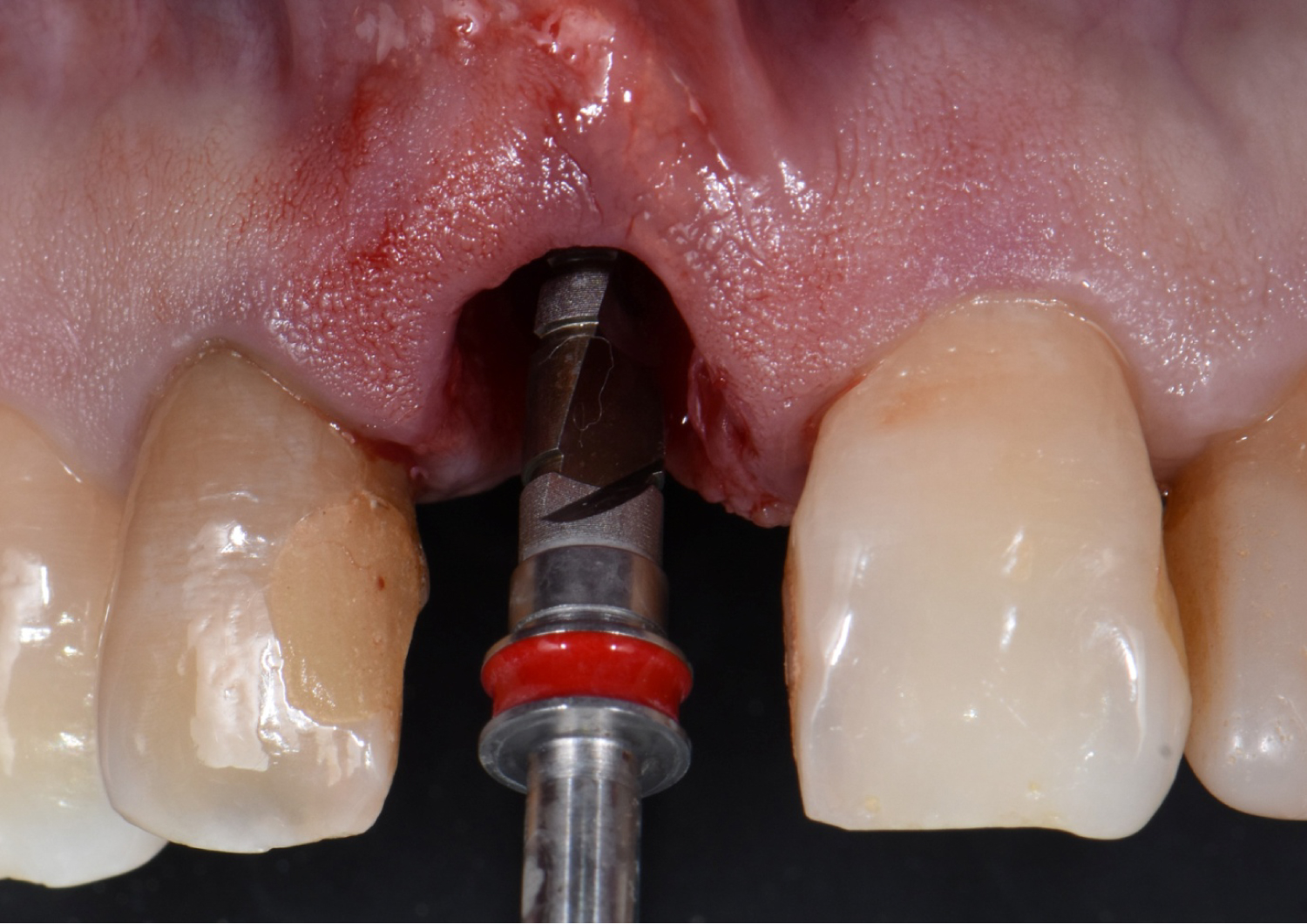 Figure 5: Implant osteotomy.
View Figure 5
Figure 5: Implant osteotomy.
View Figure 5
Primary stability was achieved in the apical third of the implant with a 35 N torque. The labial gap was filled with a small particle allograft, and a connective tissue graft from the palate (10 × 6 mm) was taken and fixed in the previously created envelope with a 5-0 absorbable suture (Figure 6).
 Figure 6: Soft and hard tissue graft.
View Figure 6
Figure 6: Soft and hard tissue graft.
View Figure 6
Provisionalization: After implant placement, the provisional restoration was prepared. First, the milled PMMA provisional prosthesis was oriented and screwed onto the implant, it was modified with the help of a silicone guide taken from the diagnostic wax-up (Figure 7). When the correct height and contours were achieved, a flowable composite was injected into the subgingival contours. The critical and subcritical profiles were designed to shape the gingival tissues. After modifying the profile, the clinical crown portion was made with a bys-acryl composite resin, using the same silicone guide.
 Figure 7: Silicone guide for provisional prosthesis.
View Figure 7
Figure 7: Silicone guide for provisional prosthesis.
View Figure 7
The temporary restoration was polished to avoid irritation, gingival migration, and dental biofilm accumulation (Figure 8). The restoration was left with no occlusal contact with the opposing arch during centric and eccentric movements, a control radiograph was taken and post-operative indications were given (Figure 9).
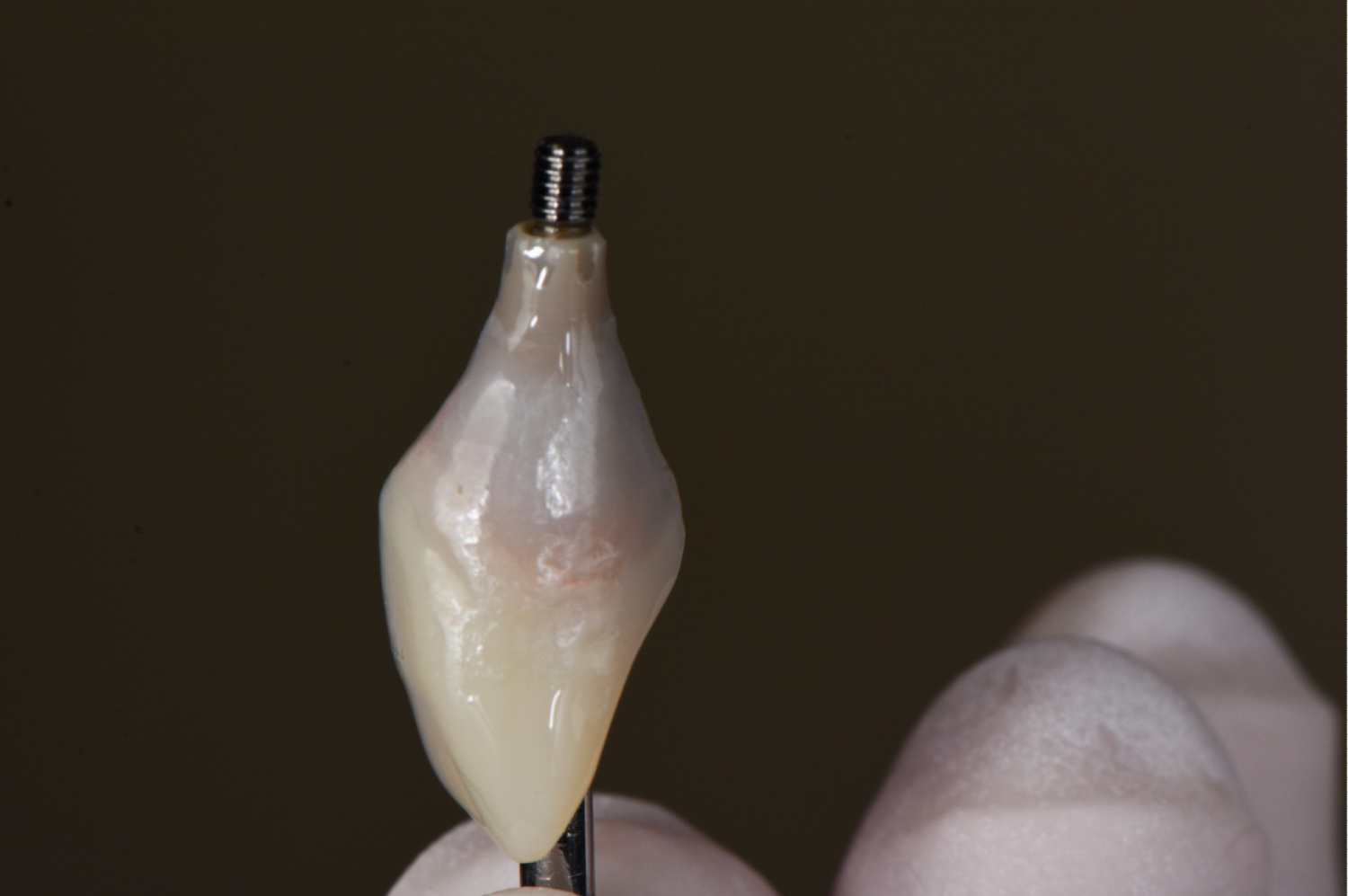 Figure 8: Provisional prosthesis.
View Figure 8
Figure 8: Provisional prosthesis.
View Figure 8
 Figure 9: Post-operative control radiograph.
View Figure 9
Figure 9: Post-operative control radiograph.
View Figure 9
Antibiotic and analgesic therapies were indicated. Also, to avoid brushing the surgical area for 3 weeks and rinse with 0.12% chlorhexidine for 2 weeks. Likewise, a soft diet, and to avoid physical activities.
After 4 months, with adequate tissue healing (Figure 10), and the emergence profile correctly created (Figure 11), the final impression was taken. The following steps were used to make a custom-made impression coping:
 Figure 10: 4 months after surgery.
View Figure 10
Figure 10: 4 months after surgery.
View Figure 10
 Figure 11: Emergence profile.
View Figure 11
Figure 11: Emergence profile.
View Figure 11
1. The analog was submerged 2/3 into addition silicone.
2. The implant provisional was connected to the analog abutment.
3. Light body impression material was injected around the provisional restoration connected to the analog.
4. Flowable composite was injected into the space between the impression material and impression coping.
This technique was used to maintain the complete emergence profile and prevent the gingival tissue from collapsing at the time of impression taking.
Subsequently, the custom-made impression coping was taken along into the mouth and it was connected into the implant without making any modifications as the profile was established with the use of the temporary prosthesis (Figure 12). A final impression was taken with an open tray impression technique using an addition silicone material (Figure 13).
 Figure 12: Open-tray impression abutment with flowable composite in the emergence profile to replicate provisional prosthesis.
View Figure 12
Figure 12: Open-tray impression abutment with flowable composite in the emergence profile to replicate provisional prosthesis.
View Figure 12
 Figure 13: Final impression with addition silicone.
View Figure 13
Figure 13: Final impression with addition silicone.
View Figure 13
The impression was cast with type IV dental stone, and the laboratory process was carried out. A CAD/CAM milled titanium straight prosthetic abutment was used. The profile was conformed with pink feldspathic porcelain for a more natural appearance, and the implant abutment was opaqued in the coronal portion for aesthetic effects (Figure 14). A lithium disilicate crown was made, and it was stratified with feldspathic ceramic for aesthetic purposes.
 Figure 14: Opaqued CAD/CAM milled titanium abutment.
View Figure 14
Figure 14: Opaqued CAD/CAM milled titanium abutment.
View Figure 14
The restoration was tried in the patient, and after approval, we proceeded to cementation. The titanium abutment was screwed with a torque of 35N and the restoration was cemented with dual resin cement (Figure 15).
 Figure 15: Cemented restoration.
View Figure 15
Figure 15: Cemented restoration.
View Figure 15
Monthly periodic appointments have been made for 2 years to observe treatment evolution; gingival tissue is intact, inflammation or bleeding has not been observed, color and thickness of gingival tissue are adequate, and the marginal levels have been maintained at an acceptable height in comparison to preclinical levels and adjacent teeth. In addition, patient's satisfaction with the final result (Figure 16).
 Figure 16: Final results.
View Figure 16
Figure 16: Final results.
View Figure 16
Immediate placement of dental implants has the advantage of reducing treatment time, and has a similar success to traditionally placed implants, likewise, offers the option of immediate provisionalization by allowing excellent aesthetic results and improving the patients' life quality [10,11].
However, multiple publications have reported recession and loss of crestal bone height. Although the vestibular placement of implants was the main cause of recession, in most cases, the phenotype and factors that affect crestal bone such as traumatism, played an important role [12,13].
A study in animals demonstrated that when implants are placed in a more palatal position, it is possible to maintain the vestibular wall and avoid the presence of recession, a commonly reported problem [14].
A drawback of implants with conventional technique is that after tooth extraction, certain bone resorption occurs, which can compromise the favorable position of the future implant and the restoration's esthetic outcome [15,16]. In 1989, a protocol that consisted of the post-extraction implant placement was introduced, such protocol has been adopted over the time due to the advantages it presents [17].
Nowadays, there are 4 types of implant placement protocols described and developed by the ITI, and their application will depend on the patient's clinical and radiographic preoperative planning [18]; this includes correct aesthetic diagnosis [19], atraumatic surgical techniques [20], surgical procedures for hard and soft tissue augmentations [21,22] and a previously planned placement by computed tomography (CBTC) [23].
The reported survival rates for early and late implant protocols (type 2-4) range from 97.17 to 98% [24], compared to immediate placement (type 1), which ranges from 93.80 to 100% [24,25]. Therefore, it could be an option to consider through prior evaluation of the patient since it reduces the total treatment time and increases patient comfort.
Retrospective studies have reported that the immediate placement of implants and the opportunity to graft the residual gap, as well as the placement of an immediate provisional, allow us to maintain the height and thickness of the peri-implant mucosa [2,26]. In addition, the placement of a soft tissue graft contributes to the stability of the gingival levels and the increase in the contours of the soft tissues [21], mainly in patients with a thin phenotype, where this type of procedure allows the thickening of the same.
During implant placement, primary stability, Resonance Frequency Analysis (RFA), and insertion torque are often the most commonly used criteria to select loading protocols [27]. In a systematic review by Schrott in 2014 [28], a minimum torque of 30 Ncm is indicated for immediate loading, a minimum stability ratio (ISQ) between 50 and 62 and an implant of at least 8 to 11 mm in length between the different studies reviewed; for immediate implant placement with immediate loading, a success rate of 87.5 to 100% can be expected [29]. In this case report, an insertion torque of 35 N was obtained with the placement of a 10 mm long implant. Therefore, immediate loading was possible, and an emergency profile with adequate dimensions was obtained.
The introduction of predictable surgical and prosthetic techniques, as well as biocompatible materials have made it possible to meet the aesthetic and functional demands of patients. Post-extraction implants can be placed with the option of immediate loading. This has proven to be a breakthrough in modern dentistry.
It is necessary to have a careful case selection, correct diagnosis and an appropriate treatment plan to accomplish a successful result. It is also important to take into account if a bone graft to fill the gap between the implant and the socket walls is necessary, the need of soft tissue grafts in patients with a thin phenotype, assess the possibility of immediate loading depending on the primary stability of the implant, soft tissue management with the provisional prosthesis and the material of the final restoration to obtain the desired results.