The purpose of this study was to investigate the influence of retention procedures on the percentage of occlusal loads experienced by single implant-supported crowns and tooth-supported crowns within the mouths of carefully selected human test subjects. Thirty subjects were selected: 20 received a single implant and full crown restoration; and 10 received a single crown restoration on a natural tooth. The percentage of occlusal loads on crowns was recorded before and after cementation or after hand tightening and torque tightening by computerized occlusal analysis (T-Scan III system). Three cementation methods were used: Method A: Biting directly with the opposing teeth during cementation; Method B: Biting on articulating papers against opposing teeth and Method C: Biting on a cotton roll interposed between restoration and opposing teeth. For cement-retained single implant crowns, the percentage of occlusal load showed no significant change after cementation in Method B. For tooth-supported crowns, the percentage of occlusal load exhibited no significant change after cementation in Method A. For screw-retained implant crowns, torque tightening induced significantly lower percentage of occlusal loads than hand tightening.
Occlusal load, Implant-supported crown, Tooth-supported crown
TMJ: Temporomandibular Joint; SPSS: Statistical Program for Social Sciences; 3D: Three Dimensions
Occlusal interferences could cause harmful effects to the teeth, restorations and TMJ (for example tooth mobility, fracture of restorations and occlusal discomfort) [1]. Moreover, overloading resulting from improper occlusion could cause complications and failure of dental implants [2,3]. In daily practice, a new occlusal interference or deflective contact of restorations might occur after cementation even after they have been completely removed before cementation. Cementation procedures might have an effect on occlusal load of restorations. Implants showed significantly less mobility both vertically and horizontally than natural teeth because of the lack of the periodontal ligament [4]. The effect of the cementation procedure on occlusal load for implant-supported crowns might be different from that for tooth-supported crowns.
By now, dental implants can be restored with either cement- or screw-retained prostheses. Different advantages and disadvantages have been presented for both types of retention methods [5,6]. Cement-retained implant crowns were selected because: Similarity to natural teeth, simplicity, aesthetic occlusal surfaces, and as a solution to problems with improperly inclined implants [7-10]. As for their disadvantages, removal of luting agent excess can be difficult and the presence of residual cement can be a risk factor of mucositis and peri-implantitis [11,12]. Sometimes screw-retained restorations were selected, because they could avoid residual cement; this might decrease the complications in the soft tissue [13]. Clinicians also could easily remove these restorations when repair of ceramic veneering is necessary [14]. Furthermore, compared with screw-retained crowns, cement-retained crowns showed different movement during retention procedures [15-17]. The internal cone implant system might allow apical displacement of the crowns during screw tightening [15,17]. Cement-retained crowns might exhibit occlusal displacement because crowns might be lifted by cement during cementation procedures [17]. Therefore, the change in occlusal loads of implant crowns during screw-retained procedures may differ from that during cement-retained procedures.
The purpose of this study was to investigate the influence of retention procedures on the percentage of occlusal loads experienced by single implant-supported crowns and tooth-supported crowns within the mouths of carefully selected human test subjects.
The study was approved by the ethics committee of Tongji University, Shanghai, China (no. 15,8200,0245,7132). Written informed consent was obtained from each subject with permission to use their data for scientific purposes. The study was conducted in accordance with the Declaration of Helsinki (1964). Thirty subjects were carefully selected: 20 received a single implant-supported crowns; and 10 received a single tooth-supported crowns. Inclusion criteria were set as the following: No temporomandibular disorders, no significant history of bruxism or clenching of the teeth determined by interviewing the patients, age of less than 70 years, minimal periodontal conditions as evaluated by a periodontist (maximum pocket depths around 3 mm with absence of signs of inflammation). Additional inclusion criteria for subjects to receive an implant-supported single crown were followed: No other tooth loss except one maxillary first molar and third molars, no other crown restoration except single implant crown restoration.
Twenty single dental implants (Φ4.1 mm, internal conical implant, BioHorizons Internal, Bego, AL, Germany) were placed for missing maxillary first molars in 20 subjects (11 men and 9 women; mean age, 38 years; range, 25 to 48 years) and were randomly divided into 2 groups of 10. Ten cement-retained single implant crowns and 10 screw-retained single implant crowns were fabricated respectively. In addition, 10 conventional tooth-supported single crowns were fabricated and placed on maxillary first molars in 10 subjects (6 men and 4 women; mean age, 36.5 years; range, 26 to 45 years).
Restoration started after 3 months of implant placement. No provisional implant-supported restorations for soft tissue conditioning were used. Impressions were made using polyvinyl siloxane (Silagum, DMG, Hamburg, Germany) with an open-tray technique. Ten cement-retained single implant crowns were fabricated. Anatomical straight abutments with 8.5 mm height and 1-2 mm gingival height (BioHorizons Internal, Bego, AL, Germany) were selected to support the restorations. The peripheral margins of the abutments were prepared 0.5 mm subgingivally in the form of deep rounded-shaped chamfer. The copings were casted with Ag-Ab alloy (Isifuku, Tokyo, Japan) and veneered with veneering porcelain (Vintage, Shofu, Tokyo, Japan). The titanium abutments were screwed to the implants using a torque driver set at 30 Ncm; screw channels were closed with dental wax (Wax Pak, 3M Unitek, Monrovia, CA, USA). To fabricate the screw-retained single implant crowns, a castable titanium abutment (internal conical implant-abutment connections, Bego, AL, Germany) were used.
For the tooth-supported single crowns, the abutment teeth received a successful root canal treatment and an adhesive composite build-up because of apical periodontitis or pulpitis. The first molars were prepared with a 0.5 mm-deep subgingival finish line in the form of deep rounded-shaped chamfer, with approximately 7 mm axial wall heights. A die spacer (Tru‐Fit, George Taub Products, Jersey City, NJ) was used to create space for the cement. The metal-ceramic crowns were fabricated with the same materials as the implant-supported crowns in the same dental laboratory. The marginal gaps of crowns were carefully examined on a profile projector (V-16D, Nikon, Japan) prior to placement, and were confirmed to be less than 100 um. Dental floss was used to check the tightness of proximal contact points which is between 50 μm and 100 μm. All tooth-supported crowns and implant-supported crowns were placed by the same prosthodontist (JT).
Computerized occlusal analysis was conducted using the T-Scan system (T-Scan III v8; TekscanInc, South Boston, MA, US). The system was first employed to perform computer-guided occlusal adjustment for all crowns. It was then used to record the percentage of the occlusal load for the crowns on the same day. Premature contacts were specifically positioned and adjusted based on the overloaded contact locations displayed within the system's 3D load/view panes (through colour coding) (Figure 1) and articulating paper locations (Figure 2). Corrective occlusal adjustments were carried out using the percentage of the occlusal load occurring on the teeth (Figure 3). For implant-supported single crowns, the occlusal scheme was designed to no contact at light bite and light contact at heavy bite [18]. After corrective occlusal adjustments, three consecutive recordings of the subjects' maximum intercuspal position were taken, ensuring a minimum of 60 s between each reading. The outcome measure for each crown was averaged. Single examiner (JT) recorded three maximum intercuspal position readings for each subject.
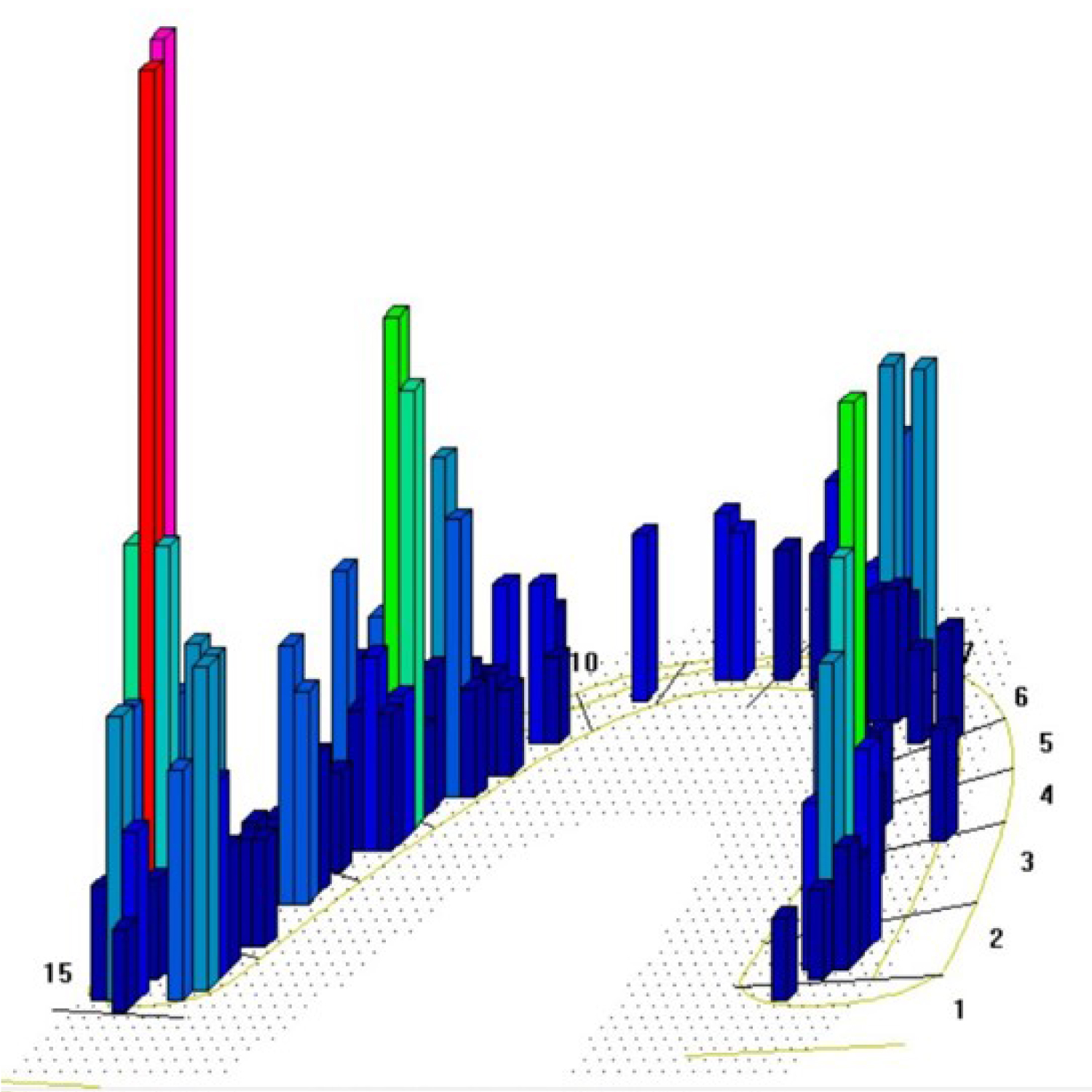 Figure 1: 3D load/view shows premature contacts at particular areas, indicated by red columns.
View Figure 1
Figure 1: 3D load/view shows premature contacts at particular areas, indicated by red columns.
View Figure 1
 Figure 2: Premature contacts location indicated by articulating paper (Red arrow).
View Figure 2
Figure 2: Premature contacts location indicated by articulating paper (Red arrow).
View Figure 2
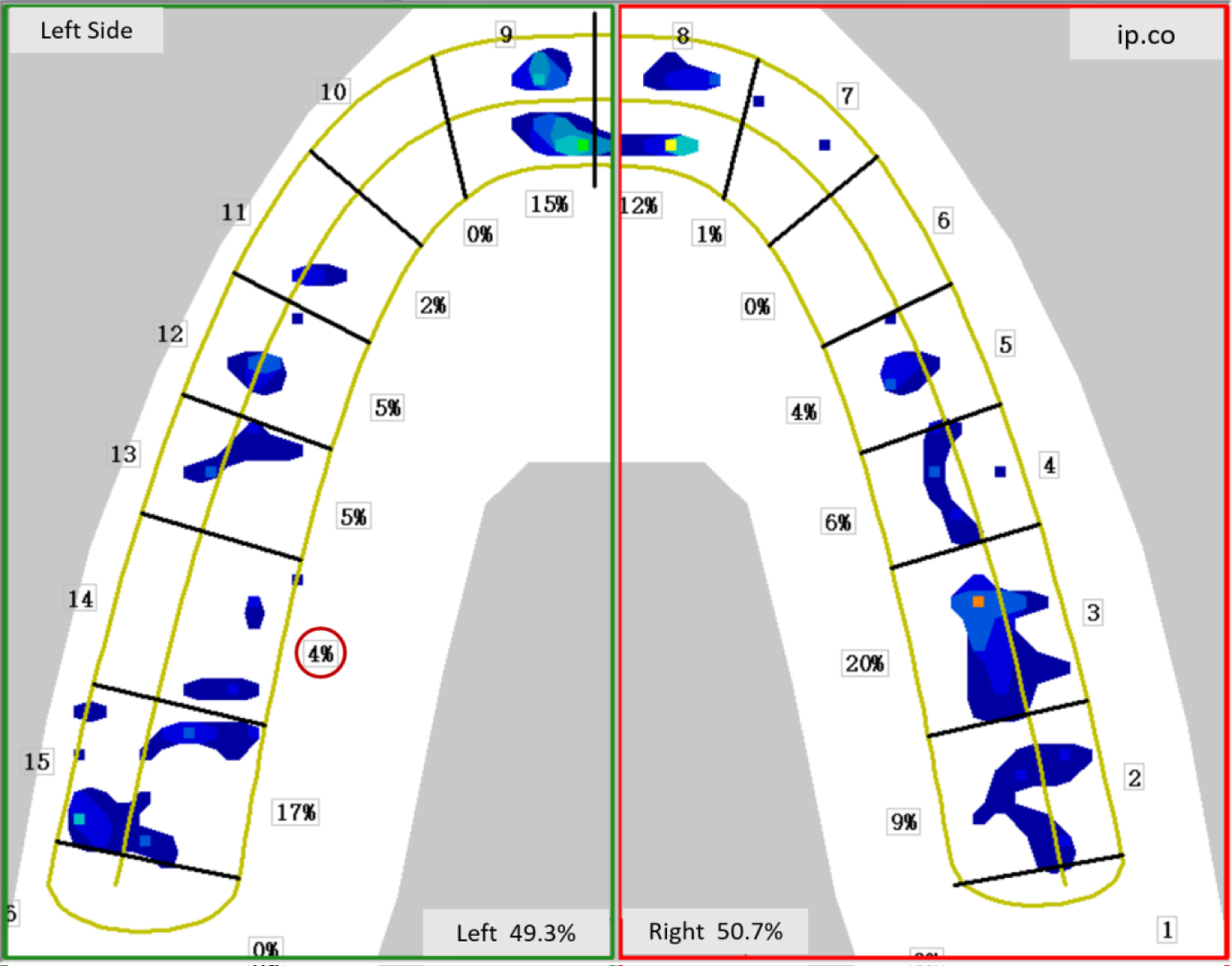 Figure 3: 2D load/view shows the percentage of the occlusal load (Red circle).
View Figure 3
Figure 3: 2D load/view shows the percentage of the occlusal load (Red circle).
View Figure 3
The cement-retained implant crowns and tooth-supported crowns were cemented with provisional cement (TempoCemNX, DMG, Hamburg, Germany). Provisional cement was mixed according to the manufacturer's instructions. The cement were placed at the crown margin in a 1⁄2 toroid shape with a 1-mm radius. The crown was seated onto the abutments with slight finger pressure, and then conducted with different cementation procedures. The cementation procedure was divided into three methods: Method A) Biting directly with the opposing teeth during cementation; Method B) Biting on 20 um-thick articulating papers against opposing teeth (Bausch, Koeln, Germany) and Method C) Biting on a cotton roll interposed between restoration and opposing teeth (Medicom Inc., Augusta, Ga, USA) (Figure 4). The articulating papers or cotton rolls were only used on the restoration side. Each crown was performed with three cementation methods. GC removal plier (GC, Tokyo, Japan) was used to remove the cemented crowns, the residual cement was completely removed with ultrasonic cleaner (DSA-50, Liangyou Inc., Zhejiang, China) and prepared for next cementation method. The cementation procedures were performed in the following order: Method A, Method B and Method C. In 15 minutes after every cementation, occlusal parameters were recorded again with the T-Scan system. For each subject, the same sensor was used before and after cementation. The sensor was held consistently in the same position with respect to the teeth. It was aligned to be parallel to the occlusal plane and centered on the midline between the central incisors [19].
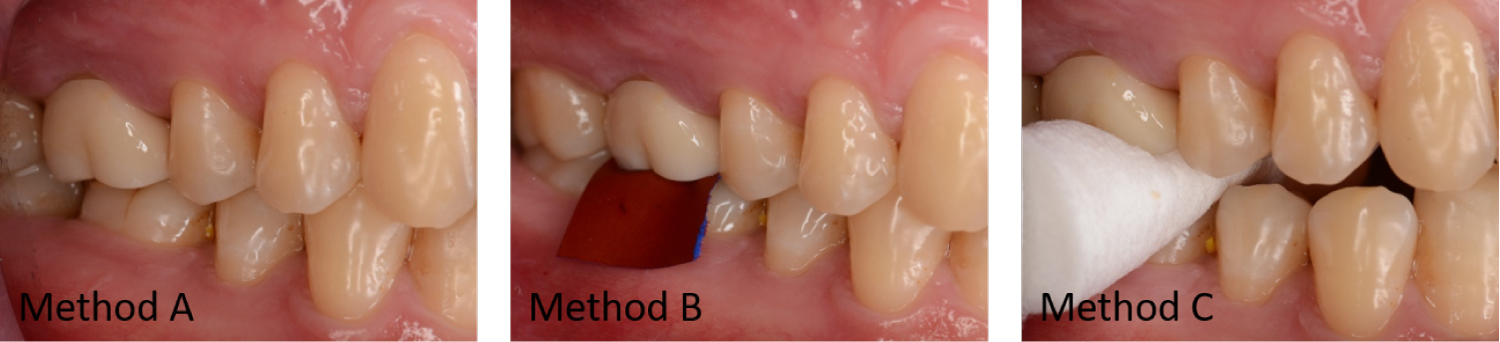 Figure 4: Clinical images of 3 cementation methods: Method A) Biting directly with the opposing teeth during cementation; Method B) Biting on articulating papers against opposing teeth: Method C) Biting on a cotton roll interposed between restoration and opposing teeth.
View Figure 4
Figure 4: Clinical images of 3 cementation methods: Method A) Biting directly with the opposing teeth during cementation; Method B) Biting on articulating papers against opposing teeth: Method C) Biting on a cotton roll interposed between restoration and opposing teeth.
View Figure 4
For screw-retained single implant crowns, after the crowns were hand tightened (15 Ncm) in clinic, occlusal adjustment was performed in the same way as the cement-retained implant crowns. Then, the percentage of the occlusal load for crowns was recorded using the T-Scan system. Finally, the crowns were tightened using a torque driver set at 30 Ncm and occlusal parameters were re-evaluated.
The methodology and results of the study were reviewed by an independent statistician. SPSS 22.0 (IBM, Armonk, NY, USA) was used for data analysis. The Kolmogorov-Smirnov test of normality was conducted for the data of the occlusal load percentage pre-retention and post-retention. Most of the variables were not found to be normally distributed. Data were, therefore, statistically analyzed with the Wilcoxon signed-rank test. Level of significance was set as α = 0.05.
The percentage of occlusal load before and after cementation for tooth-supported crowns is shown in Figure 5. The percentage of occlusal load was 12.1 ± 3.2, 12.5 ± 4.1, 14.2 ± 9.1 and 17.9 ± 11.2, respectively for before cementation and after cementation (Method A, Method B and Method C). The percentage of occlusal load showed no significant change after cementation in Method A (biting directly with the opposing teeth during cementation).
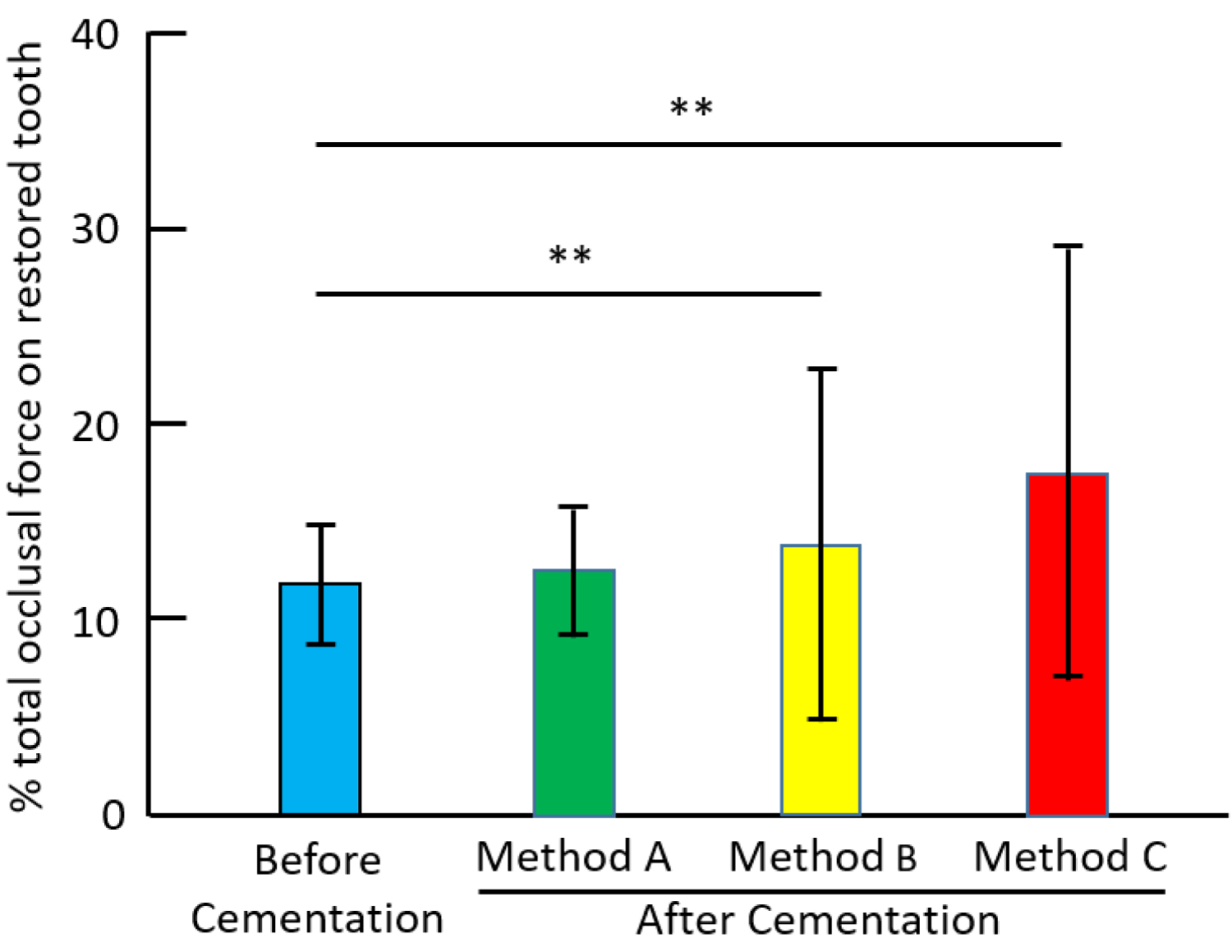 Figure 5: The percentage of occlusal load before cementation and after cementation for tooth-supported single crowns: Method A) Biting directly with the opposing teeth during cementation; Method B) Biting on articulating papers against opposing teeth; Method C) Biting on a cotton roll interposed between restoration and opposing teeth; **P < 0.01.
View Figure 5
Figure 5: The percentage of occlusal load before cementation and after cementation for tooth-supported single crowns: Method A) Biting directly with the opposing teeth during cementation; Method B) Biting on articulating papers against opposing teeth; Method C) Biting on a cotton roll interposed between restoration and opposing teeth; **P < 0.01.
View Figure 5
Figure 6 shows the percentage of occlusal load before and after cementation for cement-retained single implant crowns. The percentage of occlusal load was 7.4 ± 3.1, 15.7 ± 7.8, 8.6 ± 2.3 and 8.9 ± 2.5, respectively for before cementation and after cementation (Method A, Method B and Method C). The percentage of occlusal load exhibited no significant change after cementation in Method B (biting on articulating papers).
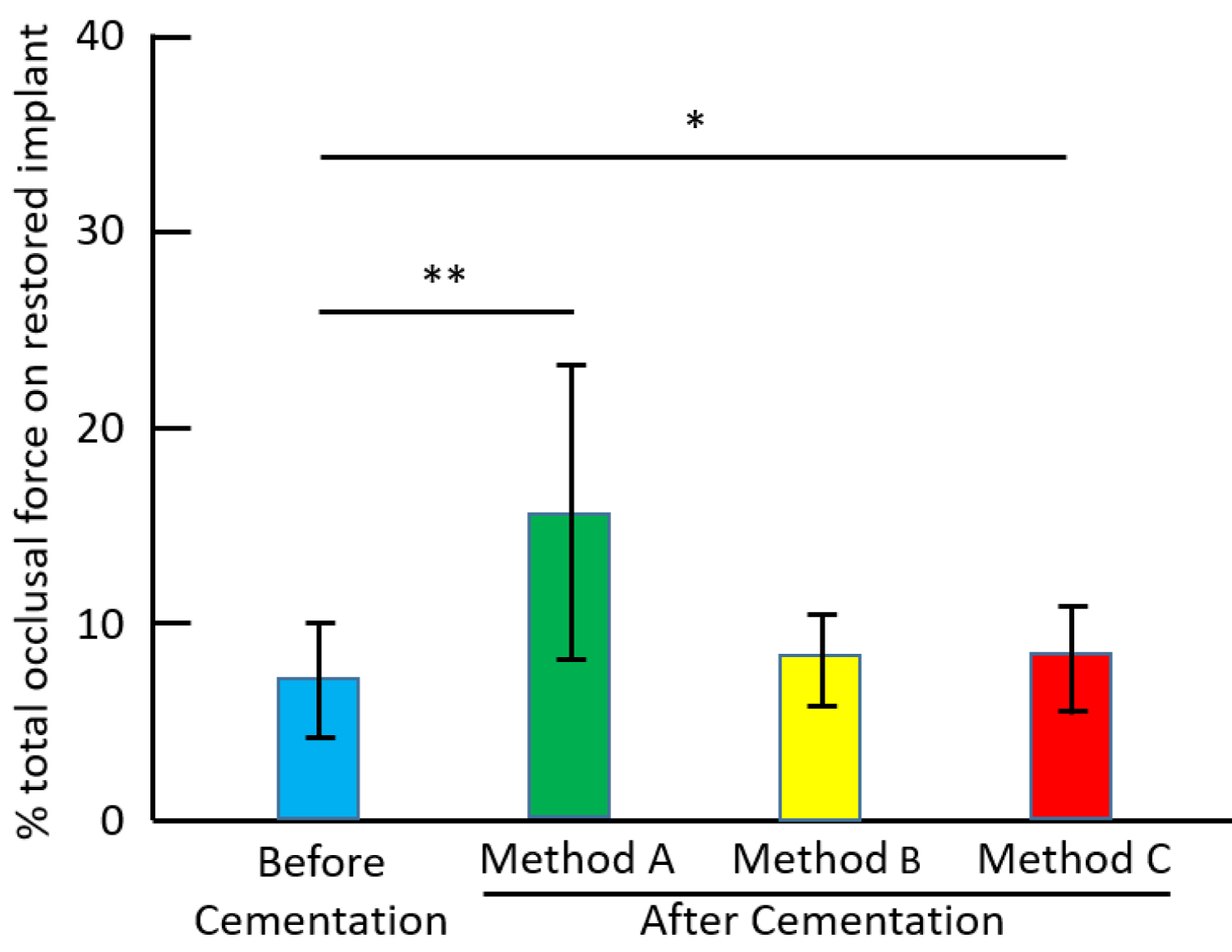 Figure 6: The percentage of occlusalload before cementation and after cementation for cement-retained single implant crowns (*P < 0.05, **P < 0.01).
View Figure 6
Figure 6: The percentage of occlusalload before cementation and after cementation for cement-retained single implant crowns (*P < 0.05, **P < 0.01).
View Figure 6
Figure 7 shows the percentage of occlusal load for screw-retained single implant crowns. The percentage of occlusal load after torque tightening was 6.7 ± 4.4, significantly lower than that after hand tightening (9.4 ± 4.5).
 Figure 7: The percentage of occlusal load after hand tightening and torque tightening for screw-retained single implant crowns (**P < 0.01).
View Figure 7
Figure 7: The percentage of occlusal load after hand tightening and torque tightening for screw-retained single implant crowns (**P < 0.01).
View Figure 7
The computerized occlusal analysis T-Scan system was found to be considerably accurate and has been implemented in different clinical dental applications [20]. The T-Scan system recorded the distribution of relative load values around the tooth row, but not absolute load values [21]. However, several studies investigated the reliability and sensitivity of the T-Scan system and reported that the sensors did not have the same accuracy among themselves [21,22]. The reliability of the T-Scan III was reported to be increased with initial tempering of the sensor, reuse of personalised sensors for each patient and standardised positioning of the sensor holder [23]. The T-Scan III showed a high degree of reproducibility when used to perform consecutive measurements [20,24]. In this study, the percentage of total occlusal load on each tooth was recorded before and after cementation following a similar protocol devised by Gallagher, et al. [23].
Because the physiological movement of natural teeth is greater than that of implants, when natural teeth and an implant prosthesis in the same dentition occlude with opposing teeth simultaneously, the implant prosthesis receive most of the occlusal load. The excessive occlusal load is transmitted to the abutment connection and to the supporting bone, which may impede the long-term prosthesis integrity and osseointegration of implants [2,3]. Therefore, in mixed implant-natural tooth independent occlusal schemes, the optimal clinical situation is that the implant prosthesis commences occluding and occludes slightly after the natural teeth have depressed partway into their periodontal ligament fibers and began to meet resistance by the surrounding alveolar bone [19,25]. For this reason, the occlusal scheme was designed to no contact at light bite and light contact at heavy bite in this study [25].
Non-mobile posterior teeth depress into their periodontal ligament fibers about 28 µm vertically [26]. Conversely, well osseointegrated implants exhibit a mean 5-µm vertical depression [27]. Therefore, the 20 µm-thick articulating papers were used during cementation in Method B.
For tooth-supported crowns, the similar percentages of occlusal load were observed before and after cementation in Method A. On the other hand, Method B and Method C, exhibited significantly greater percentage of the occlusal load after cementation than before cementation. Biting on articulating papers or a cotton roll could induce lateral excursion because the biting side worked as the working side. Occlusal contacts of the working side in Methods B and C were different from that before cementation in the maximum intercuspal position. The difference of occlusal contacts might cause lateral displacement of crowns during cementation, therefore, result in the change in the percentage of occlusal load after cementation. If the fitness of crowns is worse, the displacement of crowns might become more obvious.
For cement-retained single implant crowns, Method A exhibited the significantly greater percentage of occlusal load after cementation than before cementation. In this study, the occlusion of implant-supported crowns was adjusted to light contact at heavy bite before cementation. As a consequence, the crown was lifted by the cement due to nothing interposed between crowns and opposing teeth in Method A. Crowns cemented with Method B almost showed no post-cementation displacement because there was an interference of the thin articulating papers during cementation. While the implant-supported crowns were fabricated directly on prosthetic cylinders, the tooth-supported crowns were made on stone die. It was suggested that the inner fitness of implant-supported crowns is better than that of the tooth-supported crowns [28]. In Method C, the implant-supported crowns sunk vertically, lateral displacement of crowns was smaller compared with tooth-supported crowns. This is why Method C exhibited much greater effect on occlusal load for tooth-supported crowns than implant-supported crowns.
For screw-retained single implant crowns, the percentage of occlusal load after torque tightening became lower than that after hand tightening. In this study, the internal conical implant-abutment connections without platform implant system (Bego, Germany) were used. The result of present study is consistent with Yilmaz's study [16]. Yilmaz reported that there were vertical and horizontal differences in crown position between hand tightening and torque tightening for internal conical implant-abutment connections without platform implant system. An apical displacement of 43 µm was recorded after torque tightening than that of hand tightening state [16]. Therefore, the difference of occlusal load between hand tightening and torque tightening should be taken into consideration during clinical procedure to prevent functional complications such as looser occlusal contact.
After cementation, occlusal contact is usually checked again to remove the occlusal interference that occurred during cementation. In order to reduce the occlusal adjustment time after cementation, different cementation methods should be chosen according to tooth-supported crowns and implant-supported crowns. Biting directly with the opposing teeth during cementation would be selected for tooth-supported single crowns. On the other hand, biting on articulating papers should be used for implant-supported single crowns since it had no significant effect on occlusal load of crowns after cementation.
In order to reuse the crowns, the provisional cement was used in this study. The hydraulic force of provisional cement is different from the permanent cements. Although the hydraulic force of cement has influence on absolute value of occlusal load after cementation, it might not significantly change the effect of the cementation method on occlusal load of crowns.
A major limitation of this study was the small sample size, which reduces the external validity of the results. Many variable factors such as neuromuscular performance, tooth mobility, tooth morphology, type of occlusal surface and roughness of occlusal surface may influence occlusal analysis result. Therefore, further investigation of the total effects of these confounding factors based on a larger sample size and clinical trial study is necessary.
Within the limitations of this study, the following conclusions were drawn. The effect of the cementation method on occlusal load for cement-retained single implant crowns differed from that for tooth-supported single crowns. For cement-retained single implant crowns, biting on articulating papers during cementation induced no significant change in crowns' occlusal load after cementation. However, biting directly with the opposing teeth during cementation caused no significant change of occlusal load for tooth-supported crowns. For screw-retained single implant crowns, torque tightening induced lower percentage of occlusal load than hand tightening.
These findings suggest that, to prevent occlusal interference occurring during cementation, biting on articulating papers during cementation should be used for cement-retained single implant crowns. Furthermore, for screw-retained single implant crowns, occlusal adjustment should be performed after torque tightening rather than hand tightening to prevent the looser occlusal contact induced by torque tightening.
The study was supported by Shanghai Municipal Commission of Health and Family Planning, China (201840169) and the National Natural Science Foundation of China (81970962). None of the authors has a financial interest in Tekscan, Inc. The participation of volunteers was greatly appreciated. The statistical analysis of the study was performed by Dr. Jie Zhang, who is an independent statistician at Laboratory of Epidemiology and Biomedical Statistics, School of Medicine, Tongji University. The authors thank him for his contribution.
This work was financially supported by Shanghai Municipal Commission of Health and Family Planning, China (201840169) and the National Natural Science Foundation of China (81970962).
Shanghai Municipal Commission of Health and Family Planning, China and the National Natural Science Foundation of China.
The authors report no conflicts of interest related to this study.
All patients gave their written consent to participate in the study. The study protocol was approved by the ethics committee of School of Stomatology, Tongji University (No.15,8200,0245,7132).