Aim: The aim of this study is to determine the prevalence of implants with progressive bone loss after a 5-year follow-up.
Material and methods: A total of 437 patients with 1814 dental implants placed at XXX University Dentistry Faculty, YYY, ZZZ; between 2014-2019 has included to study. Implants with radiographic bone loss of 2 mm or more were assessed as peri-implantitis (PI). Longitudinal data were collected retrospectively from digital dental records. SPSS 20.0 package program was used to analyze the collected data.
Results: Radiographic average bone loss of implants when compared to the baseline bone level was 0.13 ± 0.13 mm. The rate of PI was calculated as 23.1%. It has been shown that significantly increased marginal bone loss at implants in maxilla than in mandible (p < 0.001).
Conclusion: Radiographic findings are frequently used tools in the evaluation of PI. Useful information about the success of PI can be obtained with long-term follow-up cases.
Dental implants, Diagnosis, Epidemiology, Peri-implantitis, Retrospective study
Placing dental implants in totally or partially edentulous mouths has become a routine procedure for more than 20 years [1]. 4th European Workshop of Periodontology, explained that oral implant procedures as safe, reliable and predictable treatment. This statement is based on information provided in a systematic review on the incidence of only a small number of complications such as implant failure, peri-mucositis, peri-implantitis (PI), mobility and implant fractures [2]. 1st European Workshop of Periodontology evaluates the average marginal bone resorption during the first year after the prosthetic restorations is less than 1.5 mm followed by the annual bone loss of less than 0.2 mm as a success. PI is the leading cause of failure of dental implants [3]. In a review article, a bone loss of 2.5 mm in the bone tissue around the implant was shown as one of the diagnostic criteria for PI. Other studies define PI as the exposure of the implant threads in a year after prosthesis loading [4,5].
Patient-related factors such as smoking habits and history of chronic or aggressive periodontitis has found to be related with high risk of implant failure [6]. Studies of patients undergoing periodontal therapy, the survival rate of implants over a 10-year period was 95.3% and 94.7% [7,8]. Implant survival rate are greatly affected from genetic structure, systemic diseases such as poorly controlled diabetes mellitus (DM), alveolar bone quality and occlusal forces. Patients who do not pay enough attention to oral hygiene are 3.8 times more likely to have PI than patients with good oral hygiene [9].
Another factor that negatively affects the success of the implant is the factors that are not taken into account in the placement of the implant and/or the construction of the prosthetic superstructure. Failure rate in implants positioned close to teeth are more than implants placed in edentulous arches [10]. Studies have shown that PI prevalence are higher in the maxillary and mandibular anterior region from posterior maxilla, while implant failures are more predictable in the maxillary posterior region [6,11]. Implants placed adjacent to implant are more susceptible for horizontal bone resorption. Implants placed in bone-grafted sites have showed increased vertical bone loss [12]. Studies concluded that clinical presence of keratinized gingiva prevents dental implants from PI [13]. Malpositioned placed implants led to bone loss, mobility, PI (48.2%) and finally implant failure [14].
PI and early implant failure were more frequently associated with narrow diameter implants in studies [15,16]. Rough implant surfaces exposed due to bone loss are very suitable surfaces for plaque retention. A meta-analysis study found that the prevalence of PI in implants with a moderately rough surface was lower than in implants with minimal roughness and roughness [3]. Although there were many studies examining the relationship between different collar/platform designs and PI, the interaction has not been fully elucidated [9].
The objective of the present study was to assess the long-term radiographic bone loss outcome after dental implant placement therapy in a 5-years period.
This study is a longitudinal cohort study that evaluates the data obtained by retrospectively examining digital dental records. A total of 437 patients treated with 1814 dental implants between 2014-2019 at XXX University, Faculty of Dentistry, YYY were included for evaluation. The study was conducted in full accordance with the World Medical Association Declaration of Helsinki, approved by the Ethics Committee of XXX University, Dentistry Faculty in YYY (2020/8/47). The radiographic images to be included in the study were determined according to the availability of the individual's radiographic image both before the implant application and 5 years after the implant application. Age and sex variables were registered from the dental records.
The distance from reference point (implant-fixture/abutment connection) to the first visible apical bone-implant contact was measured in millimeters [17]. All radiographs were analyzed by another physician who was unrelated to the treatment of the patients. 30 radiographs were randomly selected to measure twofold to analyze intra-examiner reproducibility [18]. Implants with radiographic bone loss of 2 mm or more were assessed as PI.
Marginal alveolar bone level of implants on digital dental radiographs was estimated using Pro-max®, PlanmecaOy (Helsinki, Finland) dental imaging software. A calibration tool was already available in the software program used to calculate distances in millimeters. At implants on radiographs, the implant length reported by the manufacturer was used for calibration.
SPSS 20.0 (SPSS Inc, Chicago, IL, USA) package program was used to analyze the collected data. The results were described as the mean ± standard deviation (SD). The normal distribution suitability of the parameters was determined by the Kolmogorov-Smirnov test. Because all parameters were normalized, comparisons between independent groups were performed statistically using the t-test. The value of p < 0.05 was considered to be statistically significant.
1814 implants of 437 patients were evaluated for analysis. There was no significant difference between population in terms of gender. The numbers of included implants/patients, average bone loss and frequency of PI for each gender, age group, jaw and location presented in Table 1.
Table 1: Distribution of marginal bone loss and frequency of PI (1814 implants). View Table 1
Periimplantitis was diagnosed around 419 implants, out of 1814 dental implants examined in the study. On the radiographs the average bone loss of all implants when compared with the baseline radiographs was 0.13 ± 0.13 mm. The ratio of PI observed at radiographs was 23.1% among all. There was significantly increased marginal bone loss at implants in maxilla than in mandible (p < 0.001) (Table 1).
Table 2 represents the ratio of distribution of PI in terms of implant number. The highest rate of PI was observed among the implants placed in areas 32 and 42 (33.3%). The lowest ratio was observed as 13.7% in implants of site 44.
Table 2: Ratio of distribution of peri-implantitis in terms of implant site. View Table 2
Figure 1 shows the PI number qualitatively based on the site where it is applied. Although the PI rate is less than 24%, the number of implants with the highest number of peri-implanter bone loss was detected in implant sites 36 and 46. There were only 2 implants recorded as PI at the site 41 and 3 implants at the site 31.
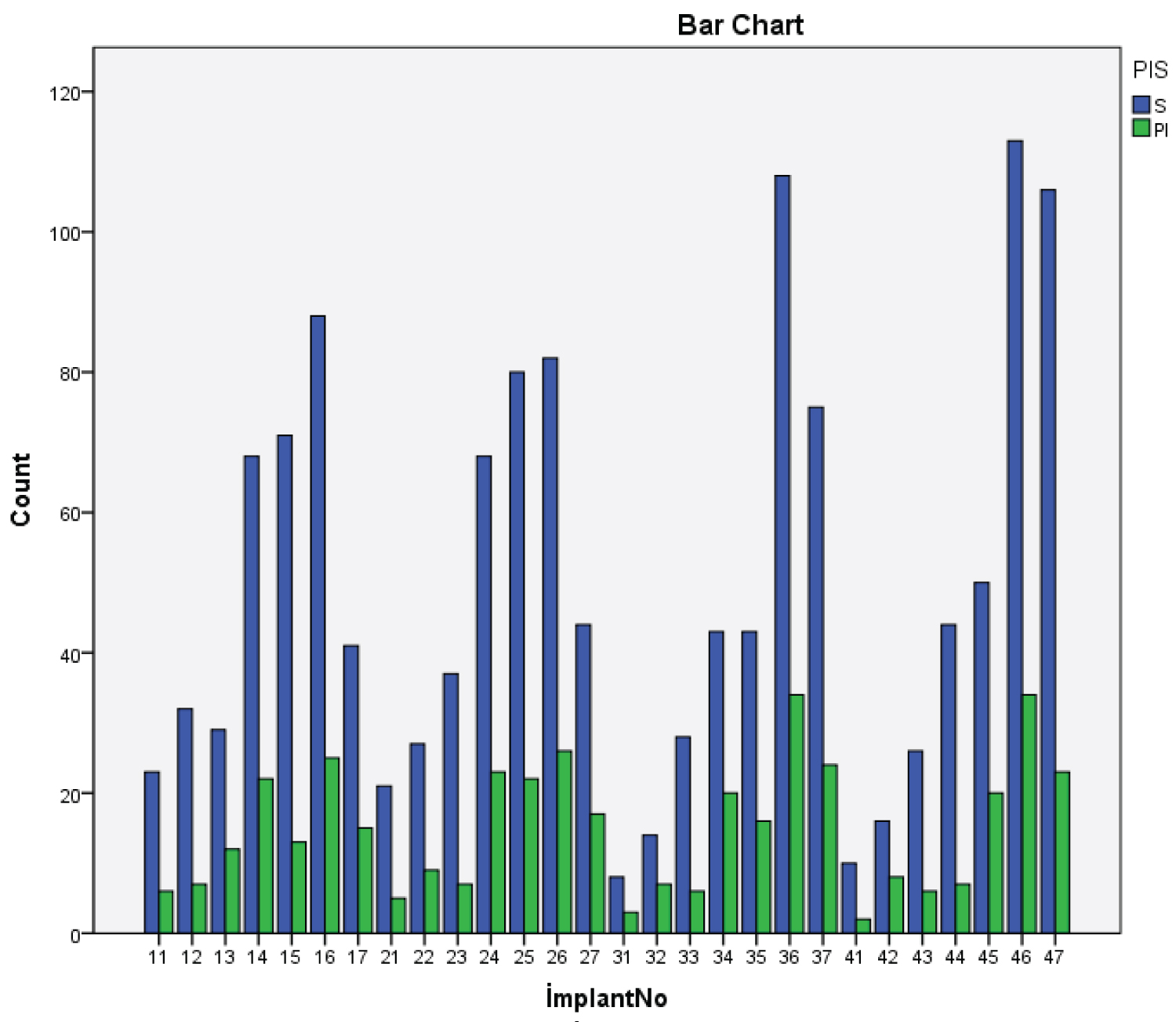 Figure 1: Number of peri-implantitis in terms of implant number.
Figure 1: Number of peri-implantitis in terms of implant number.
PI: Peri-implantitis; S: Healthy
View Figure 1
This retrospective study investigating the long-term marginal bone loss of a large number of dental implants was carried out to detail the data in which relatively few implants were evaluated in the literature. Among the 1814 dental implants examined in the research, 419 implants with PI were determined a prevalence of 23.1%. Epidemiological studies are complex due to the diversity of definitions in peri-implanter diseases [19]. Retrospective follow-up studies are cornerstones for dental implant treatment modalities. Radiographs showing bone loss around the implants are among the most important parameters used in long-term follow-up studies. Panoramic radiographs are frequently used in the evaluation of marginal bone loss around the implant, except in single implant cases. Panoramic radiographs are preferred due to being more comfortable for patients and causing lower doses of radiation in multiple implant applications [20].
The prevalence of PI reported as 0-14.4% in 2002; 16% in 2004; 16% in 2006; 23.7% in 2011; 24.4% in 2019 in studies and found as 23.1% in the present study in 2020 [18,21,22]. In addition, in a review, the prevalence of peri-implant diseases has recently been reported that ranging from 1% to 47% [23].
This study demonstrates the high survival rate in radiographic examination of implants after 5 years of loading, regardless of gender and age. In the study published by Mumcu in 2019, it was shown that bone loss around the implant is related neither age nor gender [24]. In a study examining the success rate of implants in patients with a history of periodontal disease and periodontologically healthy individuals, it was found that age and gender were not factors affecting PI in both groups [25]. The data in the present study is similar to the results presented by Attard and Zarb [26]. Additionally, Hopp, et al. suggest that female patients are prone to show a 2-fold risk than males for severe peri-implanter bone loss [27]. Increased PI prevalence in female gender has also previously been reported in another study [28].
There was statistically significant difference between implants inserted in the maxilla and the mandible in terms of PI. A higher amount of peri-implanter bone loss was observed in the maxilla. Alsaadi reported less implant loss in the mandible than in the maxilla in study [29]. When the anterior and posterior regions of the jaws were evaluated; similar amount of peri-implanter bone loss was observed in the premolar/molar area in comparison with anterior sites. In a study investigating the prevalence of implant loss, there was no difference between maxilla and mandible; however it has been shown that there is an increase in implant loss in the posterior region [30].
The major limitation of this study is that clinical measurements were not performed in addition to radiographic examination in the evaluation of PI. Another limitation is that the 5-year follow-up period may be considered short. Further studies with clinical measurements and longer follow-up period are needed.
A combination of several factors may lead to early or late implant loss due to PI. There are studies in the literature suggests that PI usually appears five years after the prosthetic loading. Additionally, there are also another contributing factors related to PI. Therefore, further work is needed to evaluate the prevalence of PI and reveal the factors related to peri-implanter bone loss by using clinical and radiographic parameters both.
There is no conflict of interest between the authors in this study.