Background: The burden of oral diseases has been identified as one of the major public health problems globally. Like many other African nations, Zambia faces a high burden of oral diseases. This study aimed to identify factors that influence oral health-seeking behaviour among adult dental patients at the Dental Training School in the Lusaka District of Zambia.
Methods: This was a cross-sectional study conducted at the Dental Training School in the Lusaka district on 384 adult dental patients (244 females and 140 males) selected using a systematic random sampling method. Data were collected using a modified World Health Organization questionnaire based on Andersen's behavioral model of health service use. The collected data were analyzed using the STATA 15.0 software. Descriptive and inferential statistical analysis was done mostly through frequency, percent (%), and multivariate analysis was conducted using binary logistic regression.
Results: The study found that the majority of the participants (81.2%) had oral diseases, and less than half of them (48.2%) had never visited the dentist in the last 12 months. The few participants (27.9%) who visited the dentist only did so when they had pain. Factors that influenced oral health-seeking behavior included being male (p-value = 0.02), being in the age group of 20-29 years (p-value = 0.044), and being unemployed (p-value = 0.011).
Conclusion: Most of the study participants did not seek oral health care services despite having dental diseases, and those that visited the dentist only did so when they had pain. Less than half of the study participants cited a lack of money as the main reason for not seeking oral healthcare.
Zambia, Health-seeking behavior, Oral health, Adult dental patients
Oral diseases pose a major health burden for many countries and affect people throughout their lifetime, causing pain, discomfort, disfigurement, and even death [1]. The impact of untreated oral diseases results in pain and impairment of function and ultimately affects the quality of life considerably [2]. These consequences are easily avoidable if people seek oral health care on time. Good oral health seeking behavior promotes not only early detection of oral diseases but also prompt clinical interventions.
In Africa, several factors, including poor oral health services, demographic factors, attitudes, and inadequate awareness information, are reported to be serious hindrances to treating dental diseases [3]. This notwithstanding, a few studies that have been done within Africa confirm the poor status of access to oral health care services [4]. In 2004, a study conducted in Burkina Faso found that 61% of people aged 35-44 had never visited a dentist [3]. Studies done in Nigeria reported that between 52 and 80% of the respondents had never been to a dentist [5-7]. According to additional studies conducted in Tanzania, only 26.5% of respondents who suffered from oral pain sought oral health services [8].
Despite the fact that many oral diseases are preventable, according to the WHO (2004), Zambia, like many other African countries, faces a massive oral disease burden, with 80% of the population reporting having been affected by oral diseases [9]. Although many studies have investigated oral health-seeking behavior elsewhere [10,11], there is a specific paucity of information on core factors that influence oral health-seeking behavior in Zambia. A study conducted in South Africa reported that low utilization of oral health was due to high dental service costs, long-distance travel, and bad dental services linked to the poor attitude of dental professionals [12]. However, there is limited literature published on the factors that influence oral health-seeking behaviour in Zambia. It is against this knowledge gap that this study aimed at identifying factors that influenced oral health-seeking behaviour among adult dental patients in the Lusaka district of Zambia.
This cross-sectional study was conducted at the Dental Training School Clinic in the Lusaka district of Zambia between September and October 2021. The sample size was 384. The study participants were adult dental patients coming from various parts of the Lusaka district seeking oral health services at the Dental Training School Clinic. Systematic random sampling was used to select the study participants. Informed consent was obtained prior to the administration of the questionnaire. Participants who had not lived in the Lusaka district for the previous twelve months or who had severe oral-related pain were excluded. The tool for data collection was a pre-tested, modified WHO questionnaire (2013) that had structured, closed-ended questions. The questionnaire elicited information on demography details, participant's knowledge and attitude towards oral healthcare, and health system barriers to oral health services. The questionnaire was administered by reading out the questions to the participants. Participants were given time to think before answering the questions. Data analysis was done using the STATA 15.0 software (Stata Corporation, College Station, USA), and data were presented in tabular and graphic form. Multivariate analysis was conducted using binary logistic regression. The P-values less 0.05 with 95% Confidence Intervals were used to assess statistical significance.
The study proposal was approved by the University of Zambia Biomedical Research Ethics Committee (UNZABREC approval no: 1481-2021), and permission to conduct the research was granted by the National Health Research Authority (Ref no: NHRA00003/4/05/2021).
The study included 384 people, with females accounting for 244 (63.54%) and males accounting for 140 (36.46%). The age of the mothers ranged from 20 years and above, with a mean average age of 37 years (SD 10.9). More than half of the participants were female (63.54 percent), 30-39 years-old (32.55 percent), married (54.95 percent), living in a low-cost area (43.08 percent), having tertiary education (46.61 percent), employed (35.42 percent), low-income (43.75 percent), and using public transportation to visit the clinic (65.10 percent) (Table 1).
Table 1: Demographic attributes of respondents (n = 384). View Table 1
The attitude of respondents towards oral health was assessed based on their responses to what made the participants seek oral health care. Those who visited the dentist only for pain relief were considered to have a negative attitude towards oral health. The results show that the majority of participants (82%) visited the dentist because of pain (toothache). This indicated a negative attitude toward oral health aimed at pain relief only (Figure 1).
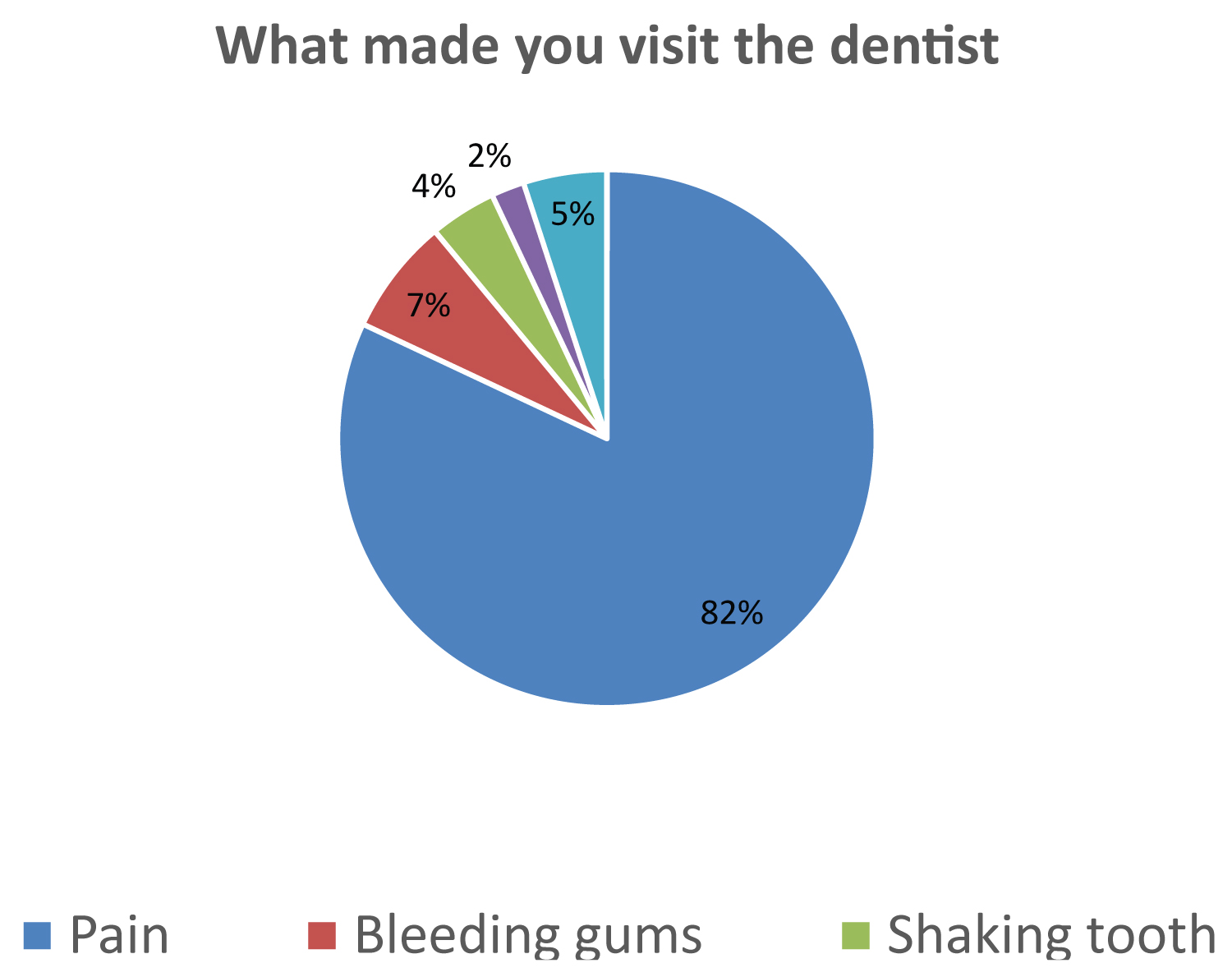 Figure 1: Attitude of patients towards oral health (n = 123).
View Figure 1
Figure 1: Attitude of patients towards oral health (n = 123).
View Figure 1
The level of knowledge was measured using fourteen (14) questions. The questions focused on causes of oral disease, oral hygiene, and oral health services. Those who correctly answered at least five questions were considered to have low knowledge of oral health care. The participants who answered five to ten questions correctly were considered to have moderate knowledge, while those who correctly answered more than ten questions were considered to have high knowledge of oral health care. The study found that less than half of the participants (45.57%) had moderate knowledge of oral health care, followed by those who had high and low knowledge, 42.87% and 11.46%, respectively (Figure 2).
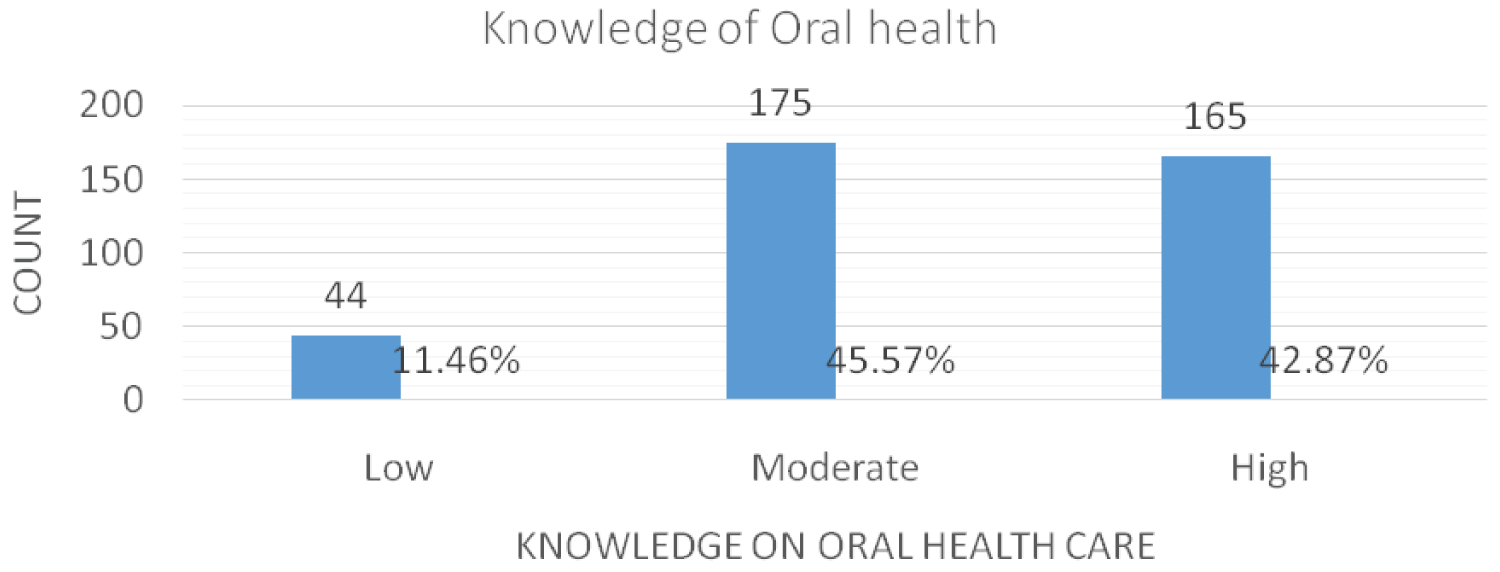 Figure 2: Knowledge of oral health.
View Figure 2
Figure 2: Knowledge of oral health.
View Figure 2
It is depicted in Figure 3 below that out of 123 respondents who visited the dentist in the last 12 months, less than one quarter of the participants (14.58%) had more than one (1) hour of waiting time, more than half of the participants (51.30%) indicated that the cost of dental treatment was expensive, and more than three quarters of the participants (77.86%) used out-of-pocket as a mode of payment for oral health services. While more than half of the participants (61.46% and 65.36% indicated that their past dental visit experience and the attitude of oral health workers were good respectively.
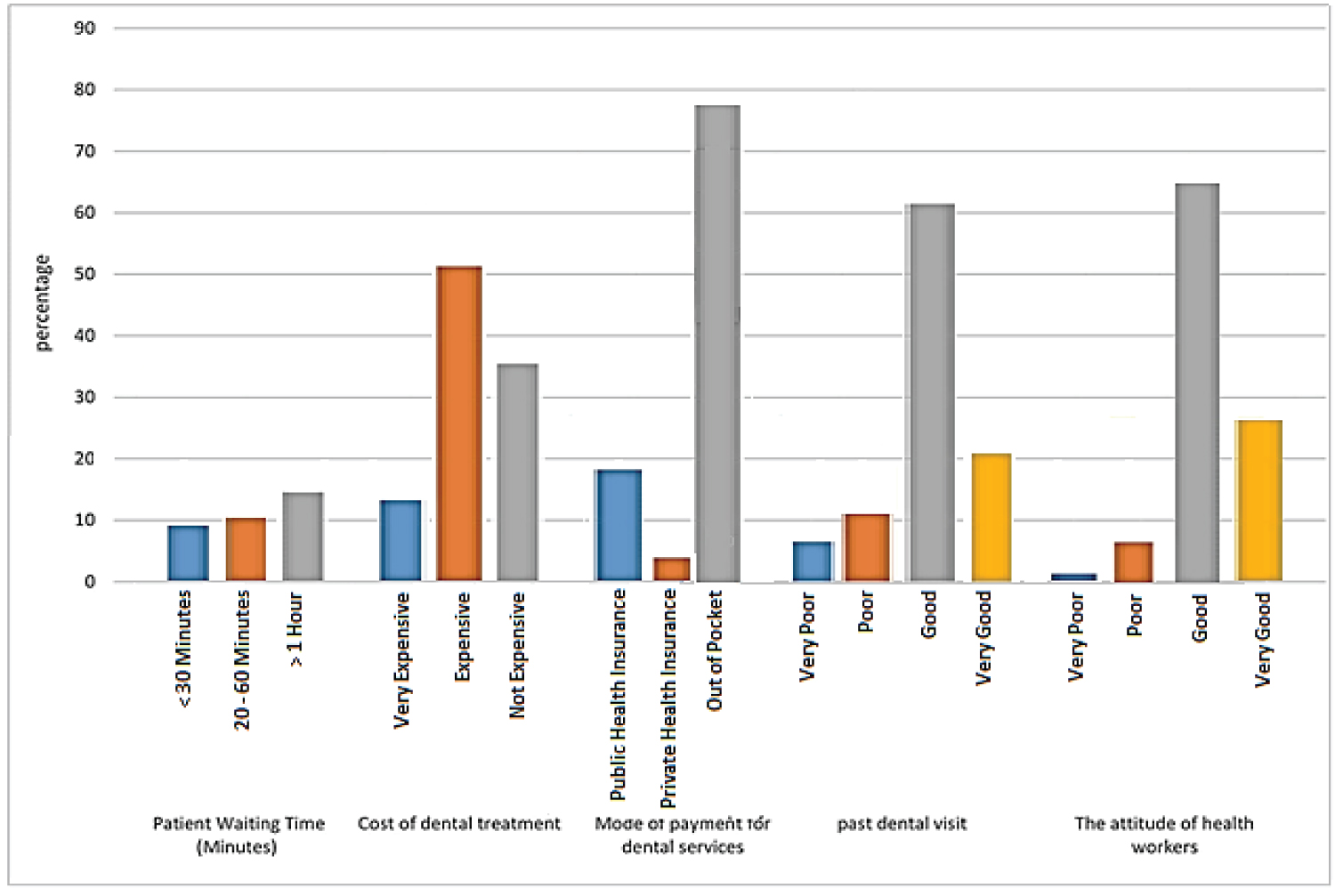 Figure 3: Healthcare system barriers (n = 384).
View Figure 3
Figure 3: Healthcare system barriers (n = 384).
View Figure 3
This revealed that the majority of the study participants (80.21%) experienced oral-related pain in the past 12 months. Despite the majority of the study participants having oral-related pain, about one-third of them (34%) sought oral healthcare. Further, the study indicated that less than half of the respondents (48.18%) did not visit the dentist in the past 12 months, and less than half of the participants cited a lack of money as the reason for not going to the dentist (Table 2).
Table 2: Oral health-seeking behaviour among adults (n = 384). View Table 2
To further validate the association of variables, a binary logistic regression analysis was conducted to establish the degree or further association of factors influencing oral health-seeking behaviour among adults for essential variables in the table below.
In Table 3, it is demonstrated that male participants were less likely to seek oral health care compared to female participants. This was statistically significant p-value of 0.02. When compared to respondents aged 50 and older, respondents aged 20 to 29 years were less likely to seek oral health care. This was statistically significant with a p-value of 0.044.
Table 3: Binary logistics regression. View Table 3
Furthermore, being unemployed reduced the chances of seeking oral health care when compared to respondents in formal employment. This was statistically significant with a p-value of 0.011. In addition, the participants who earned an income of 500 ZMK had a high likelihood of seeking oral health services compared to respondents who earned 2501 ZMK, and this was statistically significant with a p-value of 0.027. Furthermore, participants who earned between 501-1500ZMK were more likely to seek oral health compared to respondents that earned 2501ZMK, and this was statistically significant with a p-value of 0.027.
The study aimed at identifying factors that influenced oral health-seeking behaviour among adult dental patients at the Dental Training School in the Lusaka district of Zambia. The study found that the majority of the participants (81.2%) had oral diseases, and almost half of the study participants (48.2%) never visited the dentist in the last 12 months despite having oral diseases. Less than half of the study participants reported a lack of money as one of the reasons for not seeking oral health services. This finding is consistent with the report by the Ministry of Health of Zambia that revealed that the country faced a huge burden of oral diseases, with 80% of the population reporting being affected [9]. Concerning lack of money for oral health services, this study accords well with other previous studies done in the region that reported that many patients have poor access to oral health services due to their inability to pay for dental services [8,10,11].
Despite the majority of the participants (81.2%) having oral diseases, only one-third of the respondents (32%) visited the dentist in the last twelve (12) months. This finding is similar to studies done in Burkina Faso and Nigeria that found only 28% of respondents used oral health facilities in the last twelve (12) months and only 20.5% utilized oral health facilities, respectively [11,12].
Gender has been identified as one of the influencing factors in health-seeking behaviour. This study revealed that more females (68.3%) visited the dentist in the last 12 months compared to male participants (31.7%). Similarly, Zyambo, et al. [13] found that women utilized health services more often than men in urban areas [13]. These findings were also consistent with the studies done in the region [14]. Choi, et al. argued that women have a greater demand for oral health services because they are more concerned with esthetic appearances than men [15]. However, the present study finding contrasts the study findings in India that concluded that women utilized oral health services less due to high work demands in the field of agriculture [16], and it is speculated that the possible reason might be the difference in culture and lifestyles.
The age group of 30-39 years (33.5%) sought oral health services more than the other age groups. This finding is consistent with Bommireddy, et al. who concluded that seeking dental care was found to increase with an increase in age [16]. These findings are also consistent with other international studies [17,18]. However, the current study's findings differ from those of previous studies conducted in Burkina Faso [11] and India [19]. The differences in findings in India and Burkina Faso could be attributed to the fact that the majority of respondents in this study were relatively young and the study respondents were those who visited the oral facility, respectively.
As regards knowledge and attitude towards oral health care, less than three-quarters of the respondents (71.35%) knew that they can only visit a dentist when they are in pain (toothache). This is similar to the study conducted by Chambisha, et al. among primary school teachers from public schools in Ndola district, Zambia, which concluded that the most common reasons for dental visits were relief of pain (66.2%), regular (preventive) visits (28.9%), and bleeding gums (17.4%) [20]. This finding is also consistent with the two studies done in Nigeria, which concluded that 66% of respondents visited dentists for acute pain relief [12] and 55.8% consulted the dentists only when there was pain, while 27.3% had never visited the dentist [10]. Similarly, these findings reveal a lack of oral health awareness about the complications of oral diseases. Furthermore, these findings provide a foundation for the formulation of community oral health education messages.
Long waiting times impact negatively on oral health-seeking behaviour causing increased anxiety about dental treatment [21]. Only less than a quarter of the respondents who had visited the dentist in the past 12 months had to wait more than an hour to be seen. These findings are in consonance with those reported for South Africa [22] and Malaysia [23]. The possible reasons for the long waiting time could be due to the fact that Dental Training School is a referral center, easy accessibility makes the clinic vulnerable to self-referral, and there may be a shortage of dental staff. Concerning the shortage of oral health personnel, the Ministry of Health report revealed that the shortage of dental staff in the country stood at 63.4% in 2011 and 66% in 2016 [24]. However, measures aimed at addressing long waiting times at oral health facilities are highly recommended.
Evidence supports that effective interpersonal communication between the dentist and the patient helps to reduce anxiety about dental treatment and promotes good oral health-seeking behavior [22]. More than half of the participants indicated that the attitude of oral health workers and their past dental experiences were good. However, this study's findings contrast with the results reported by Broder, et al. [25], who concluded that poor interpersonal communication by dental professionals was a significant barrier for dental patients seeking oral health services in the United States of America. The possible explanation could be due to differences in sample sizes.
The results of this study are specific to Lusaka District and cannot be generalized to the rest of Zambia. In addition, because this study was carried out at a health facility, the respondents may have felt compelled to indicate that they attended dental services. Secondly, the cross-sectional design precludes causal inferences, and only associations can be drawn from the study. However, this study has provided some necessary information that might help plan appropriate oral health intervention programs and offer a foundation for future studies among the study group.
The majority of the study participants did not seek oral healthcare services despite having oral diseases, and those that visited the dentist only did so when they were in pain. The study participants complained of a lack of money as the main reason for not visiting the dentist.
The author declares that there is no conflict of interest regarding the publication of this paper.
The author would like to acknowledge the support rendered by the management and staff at the Dental Training School, as well as the academic staff of the University of Zambia, School of Public Health.
LEM conceived the study, and did data collection, BB and LEM developed the conceptual framework, provided insights in introduction, methodology and discussion. RF and LEM performed the data analysis. Then LEM and RF reviewed and edited the final copy of the Manuscript.
No financial support was received for this study.